Conservative Hip Surgery: Relief for Bilateral Dysplasia

Key Takeaway
Learn more about Conservative Hip Surgery: Relief for Bilateral Dysplasia and how to manage it. Conservative hip surgery addresses conditions like Developmental Dysplasia of the Hip (DDH) in patients such as a 47-year-old female experiencing severe bilateral groin pain and activity limitations. This joint-preserving approach targets underlying anatomical abnormalities, evident from positive impingement tests, to reduce pain, improve hip function, and potentially avoid or postpone total hip replacement, considering the patient's specific health profile.
Conservative Hip Surgery: Relief for Bilateral Dysplasia
Introduction & Epidemiology
Developmental Dysplasia of the Hip (DDH), or congenital hip dysplasia, represents a spectrum of abnormalities in hip joint development, ranging from mild acetabular dysplasia to frank dislocation. While often presenting unilaterally, a significant proportion of cases, up to 30-50% in some series, manifest bilaterally. Bilateral acetabular dysplasia poses unique challenges, often delaying diagnosis and requiring comprehensive, staged management strategies. The inherent biomechanical instability and altered load distribution in dysplastic hips predispose patients to premature degenerative changes, labral tears, and eventual osteoarthritis, particularly in the weight-bearing zones.
Conservative hip surgery, primarily encompassing joint-preserving osteotomies, aims to restore normal hip anatomy, optimize joint congruency, and redistribute articular contact pressures, thereby mitigating the progression of degenerative disease. The periacetabular osteotomy (PAO), initially described by Ganz, has become the gold standard for acetabular reorientation in skeletally mature adolescents and young adults with symptomatic hip dysplasia, demonstrating excellent long-term outcomes in preserving native hip function. Other osteotomies, such as the Dega, Pemberton, and triple osteotomy, are typically reserved for skeletally immature patients or specific deformity patterns. This review focuses on the current understanding, surgical principles, and outcomes of conservative hip surgery, with particular emphasis on the management of bilateral dysplasia in the adult and near-adult population.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy and the biomechanical sequelae of acetabular dysplasia is paramount for successful surgical planning and execution. The normal acetabulum provides comprehensive coverage of the femoral head, with a spherical articulation that distributes loads across a wide surface area. Key radiographic parameters, such as the lateral center-edge (LCE) angle of Wiberg (normal >25°), the anterior center-edge (ACE) angle (normal >20°), the Tönnis angle (acetabular index, normal <10°), and calculations of anterior, posterior, and superior acetabular coverage, are critical in quantifying the degree and pattern of dysplasia.
In acetabular dysplasia, the acetabulum is typically shallow, anteverted, and/or laterally displaced, leading to inadequate femoral head coverage. This results in:
*
Reduced Contact Area:
Concentrated stress on a smaller area of articular cartilage, predominantly in the superolateral and anterior aspects of the femoral head and acetabulum.
*
Increased Shear Forces:
Due to the more vertical orientation of the superior acetabulum, leading to labral hypertrophy and eventual tearing, as well as cartilage delamination.
*
Femoral Head Subluxation:
The femoral head may migrate superolaterally, altering the lever arm mechanics of the abductor musculature and necessitating increased muscle effort for stability.
*
Ligamentous Laxity:
The capsule and ligamentum teres may be stretched, contributing to instability.
The goals of acetabular reorientation are to normalize these parameters, increase the weight-bearing surface, improve abductor muscle mechanics, and protect the labrum and articular cartilage. The osteotomies performed in PAO selectively detach the acetabular fragment while preserving the posterior column and the blood supply via the superior gluteal vessels and obturator artery branches, allowing for precise three-dimensional reorientation without compromising pelvic ring stability.
Indications & Contraindications
The decision to proceed with conservative hip surgery for dysplasia is multifaceted, weighing patient symptoms, radiographic findings, age, and potential for long-term joint preservation. The ideal candidate is a skeletally mature patient (Risser stage 4-5) with symptomatic acetabular dysplasia, typically evidenced by hip pain (groin, lateral, or posterior), activity limitation, and radiographic signs of inadequate acetabular coverage.
Indications:
*
Symptomatic Acetabular Dysplasia:
Chronic hip pain, often activity-related, unresponsive to conservative management.
*
Radiographic Evidence of Dysplasia:
* LCE angle <20° (definite dysplasia) or 20-25° (borderline dysplasia).
* Increased Tönnis angle (>10-12°).
* Reduced anterior/posterior acetabular coverage.
* Evidence of lateral femoral head subluxation.
*
Young Adult/Adolescent Patient:
Typically 15-40 years old, with good bone quality.
*
Minimal Arthritic Change:
Tönnis grade 0 or 1 arthritis. Mild outerbridge grade 1-2 chondral changes may be acceptable if localized.
*
Intact Articular Cartilage:
Preservation of viable articular cartilage is crucial for long-term success.
*
Bilateral Dysplasia:
Management of bilateral symptomatic dysplasia often involves staged procedures. Simultaneous bilateral PAO is generally discouraged due to increased surgical time, blood loss, and prolonged rehabilitation, although some centers with high volume and specific patient selection may consider it.
Contraindications:
*
Advanced Osteoarthritis:
Tönnis grade 2 or 3 arthritis (moderate to severe joint space narrowing, large osteophytes, subchondral cysts). PAO is not effective in reversing significant arthritic changes and total hip arthroplasty (THA) is typically indicated.
*
Skeletal Immaturity:
For PAO, open triradiate cartilage (pre-Risser 4-5) is a contraindication due to potential for growth disturbance. Other osteotomies (e.g., Dega, Pemberton) are used in this population.
*
Significant Femoral Head Deformity:
Severe femoral head asphericity or necrosis that would preclude a congruent reduction within a reoriented acetabulum.
*
Active Infection:
Local or systemic.
*
Neuromuscular Disorders:
Conditions significantly impacting ambulation or muscle control (e.g., cerebral palsy with spasticity, severe polio sequelae) may compromise rehabilitation and outcomes.
*
Severe Osteoporosis:
Compromised bone quality may hinder osteotomy healing and hardware fixation.
*
Prior Hip Surgery:
Extensive scarring or hardware from previous pelvic osteotomies may complicate the approach.
*
Medical Comorbidities:
Uncontrolled systemic diseases that significantly increase surgical risk.
| Category | Operative Indications | Non-Operative Indications / Contraindications |
|---|---|---|
| Patient Profile | Skeletally mature (Risser 4-5), <40-45 years, symptomatic | Skeletally immature (for PAO), >45-50 years, asymptomatic |
| Radiographic | LCE <20-25°, Tönnis Angle >10°, Lateral subluxation | Tönnis Grade 2-3 OA, severe femoral head deformity |
| Clinical | Persistent pain despite conservative treatment, activity limitation | Asymptomatic, severe neuromuscular disorders |
| Articular Status | Intact or minimal chondral wear (Tönnis Grade 0-1) | Advanced chondral damage, large osteophytes, subchondral cysts |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes and minimizing complications.
Imaging Assessment
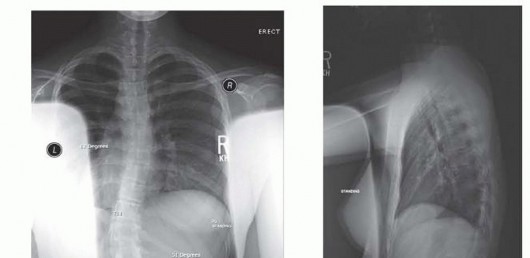
- Standard Radiographs: AP pelvis, cross-table lateral, false profile views are essential to assess LCE angle, Tönnis angle, femoral head coverage, and identify subtle retroversion or femoral anteversion.
- Computed Tomography (CT) with 3D Reconstruction: Provides invaluable information regarding acetabular morphology, femoral head sphericity, presence of osteophytes, and allows for precise planning of osteotomy cuts and anticipated acetabular fragment rotation. This is particularly useful for bilateral cases to plan staged approaches.
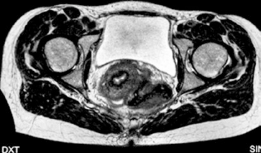
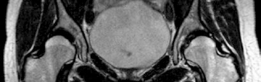
- Magnetic Resonance Imaging (MRI) / MR Arthrography: Delineates labral integrity, articular cartilage status, and can identify other intra-articular pathologies such as loose bodies or ligamentum teres tears, guiding concomitant arthroscopic procedures.
Templating
Digital templating software allows surgeons to simulate acetabular reorientation, determining the optimal vector of rotation and translation required to achieve desired coverage and minimize impingement. This helps predict the necessary screw length and trajectory for fixation. Consideration for femoral head-neck offset is also important to address any concurrent femoroacetabular impingement (FAI).
Patient Positioning
The patient is typically positioned supine on a radiolucent table.
*
Standard PAO:
A small bump or roll under the ipsilateral hip can facilitate exposure. The affected hip is slightly abducted and externally rotated initially. Image intensifier access (anteroposterior and lateral projections) must be confirmed pre-draping.
*
Bilateral Staging:
If a staged approach is planned, the contralateral hip remains draped out of the surgical field to avoid contamination. For the second side, the patient is repositioned and redraped.
*
Anatomical Landmarks:
Palpable landmarks such as the anterior superior iliac spine (ASIS), iliac crest, pubic symphysis, and greater trochanter are marked.
Detailed Surgical Approach / Technique
The modified Smith-Petersen (anterior bikini) approach is commonly employed for PAO due to its extensile exposure and ability to address intra-articular pathology concurrently if needed.
1. Incision and Exposure
- Incision: A curvilinear "bikini" incision follows the iliac crest laterally and curves distally over the anterior hip, approximately 2-3 cm inferior to the ASIS. This provides excellent cosmetic results and can be extended if necessary.
- Internervous Plane: The fascial interval between the sartorius (femoral nerve) and the tensor fascia lata (superior gluteal nerve) is identified and developed.
- Subperiosteal Dissection: The rectus femoris muscle is identified, and its direct head is detached from the AIIS, while the reflected head (if necessary) is detached from the superior acetabular rim. The iliopsoas muscle and capsule are retracted medially. The neurovascular bundle (femoral nerve, artery, vein) is protected and retracted medially.
2. Osteotomy Cuts (Ganz PAO)
The PAO involves four distinct osteotomy cuts designed to create a mobile acetabular fragment while preserving its blood supply and the posterior pelvic column.
-
First Osteotomy (Supra-acetabular Ilium):
- Subperiosteal dissection is performed along the inner and outer tables of the ilium, superior to the acetabulum, extending posteriorly toward the SI joint.
- A curved osteotome or saw is used to make an oblique cut from posterior to anterior, just above the acetabulum. This cut must stay lateral to the sacroiliac joint to avoid instability and medial to the superior gluteal neurovascular bundle.
-
Care is taken to avoid injury to the superior gluteal vessels exiting the greater sciatic notch.

-
Second Osteotomy (Ischium):
- Subperiosteal dissection along the posterior column and lesser sciatic notch.
- A curved osteotome is carefully advanced from the anterior aspect of the ischium, through the obturator foramen, towards the posterior column. Palpation of the posterior column ensures correct trajectory.
- The ischial cut extends to the posterior column, just distal to the acetabulum. This cut should remain medial to the sciatic nerve.
-
Third Osteotomy (Pubis):
- Subperiosteal dissection along the superior pubic ramus is performed.
- An osteotome or saw is used to make a cut from the lateral aspect of the superior pubic ramus, aiming towards the obturator foramen. This cut is just lateral to the origin of the pectineus.
- Care is taken to protect the obturator nerve and vessels, which exit the obturator foramen.
-
Fourth Osteotomy (Completion - Ischium):
- This cut connects the ischial and pubic osteotomies. Often, a straight osteotome is used, carefully guided along the anterior aspect of the ischium, medial to the acetabulum.
- The goal is to free the entire acetabular fragment, leaving it attached only posteriorly to the posterior column, which maintains its vascularity.
- Throughout these steps, radiographic control (fluoroscopy) is vital to confirm osteotomy placement and avoid penetration into the joint or neurovascular structures.
3. Acetabular Mobilization and Reorientation
- Once all osteotomies are complete, the acetabular fragment is carefully mobilized using a blunt elevator or bone hook inserted into the osteotomy sites.
-
The fragment is then repositioned three-dimensionally. The primary goals are:
- Lateralization: Moving the fragment laterally to increase femoral head coverage.
- Anteriorization: Correcting excessive retroversion or increasing anterior coverage.
- Rotation: Tilting the fragment to normalize the LCE and Tönnis angles.
- The repositioning is guided by visual inspection, palpation for impingement (e.g., performing a flexion-adduction-internal rotation maneuver), and fluoroscopic images. The target is typically an LCE angle >25° and a Tönnis angle <10°. Dynamic fluoroscopy can assess stability and impingement zones.
- Care must be taken to avoid over-correction, which can lead to pincer-type FAI, or subluxation during manipulation.
4. Fixation
- Once the desired position is achieved, the acetabular fragment is secured to the ilium.
- Typically, 3-4 cortical or cancellous screws (e.g., 4.5mm or 6.5mm) are used, placed from the repositioned fragment into the stable iliac bone superiorly.
- The screws must be placed to ensure robust fixation and avoid penetration into the joint space or damage to neurovascular structures. Fluoroscopic verification of screw length and position is mandatory.
5. Closure
- The detached rectus femoris is reattached to the AIIS.
- The wound is irrigated thoroughly.
- Layered closure of the muscle fascia, subcutaneous tissue, and skin.
-
A drain may be placed to manage anticipated blood loss, especially with bilateral procedures.
Complications & Management
While PAO is a highly effective procedure, it is technically demanding and associated with potential complications.
| Complication | Incidence | Management / Salvage Strategy |
|---|---|---|
| Lateral Femoral Cutaneous Nerve (LFCN) Neurapraxia | 10-20% | Conservative: Observation, nerve blocks. Surgical: Neurolysis in persistent cases. Often resolves spontaneously within 6-12 months. |
| Superior Gluteal Nerve/Vessel Injury | <1% | Prevention: Careful dissection and protection during supra-acetabular osteotomy. Management: Vascular repair, nerve repair if transected. Can lead to abductor weakness (Trendelenburg gait) or hematoma. |
| Intraoperative Fracture | 2-5% | Management depends on location: Pelvic ring fracture (fixation), acetabular articular fracture (reduction and fixation). May require modification of fixation strategy. |
| Nonunion/Malunion | 1-3% | Nonunion: Revision surgery with bone grafting and rigid fixation. Malunion: Revision osteotomy for symptomatic malposition or excessive impingement. |
| Infection (Deep) | <1% | Surgical debridement, intravenous antibiotics, hardware removal if persistent. |
| Heterotopic Ossification (HO) | 5-15% (mild-moderate) | Prophylaxis: Indomethacin or radiation. Management: Excision for symptomatic or functional impairment, often after skeletal maturity. |
| DVT/Pulmonary Embolism (PE) | 1-2% | Prophylaxis: Chemical (LMWH) and mechanical (SCDs). Management: Anticoagulation. |
| Femoral Nerve/Vessel Injury | <1% | Prevention: Meticulous retraction and protection of femoral neurovascular bundle. Management: Vascular repair, nerve repair. |
| Avascular Necrosis (AVN) of Acetabular Fragment | Rare (<0.5%) | Prevention: Preservation of posterior column vascularity. Management: If significant, may compromise long-term outcome and necessitate THA earlier. |
| Hardware-related Pain | 5-10% | Surgical hardware removal after bone healing (typically 6-12 months post-op) if symptoms persist. |
| Residual Dysplasia/Impingement | Variable | Post-operative imaging review. May require revision PAO or arthroscopic FAI treatment if symptomatic. |

Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is crucial for optimizing functional recovery and protecting the surgical repair. While specific protocols vary between institutions and surgeons, the general principles remain consistent.
Phase 1: Immediate Post-Operative (Weeks 0-6)
- Weight-Bearing: Strict non-weight bearing (NWB) or touch-down weight bearing (TDWB) on the operative extremity for 4-6 weeks to protect osteotomy healing. Crutches or a walker are used.
-
Range of Motion (ROM):
Protected ROM exercises within a pain-free arc.
- Avoid excessive hip flexion (>90°) and internal rotation, which can stress the anterior capsule and osteotomy site.
- Continuous Passive Motion (CPM) machine may be used to reduce stiffness and aid cartilage nutrition.
- Muscle Activation: Isometric exercises for quadriceps, hamstrings, and gluteal muscles (e.g., gluteal sets, quadriceps sets) to maintain muscle tone and prevent atrophy.
- Circulation: Ankle pumps, heel slides.
- Pain Management: Multimodal analgesia.
Phase 2: Early Mobilization (Weeks 6-12)
- Weight-Bearing: Gradual progression to partial weight-bearing (PWB), typically 25-50% body weight, progressing to full weight-bearing (FWB) as bone healing is confirmed radiographically.
- ROM: Continue with progressive ROM exercises, focusing on restoring full, pain-free motion while respecting surgical precautions.
- Strengthening: Introduction of light resistance exercises for hip abductors, adductors, flexors, and extensors (e.g., straight leg raises, clam shells, seated knee extension). Emphasis on core stability.
- Gait Training: Focus on normalized gait pattern without assistive devices once FWB is achieved.
Phase 3: Intermediate Strengthening and Functional Return (Months 3-6)
- Strengthening: Advance to moderate resistance exercises, functional movements (e.g., lunges, squats with proper form), balance, and proprioception training.
- Endurance: Stationary cycling, swimming, elliptical trainer.
- Sport-Specific Training: For athletes, gradual introduction of sport-specific drills, avoiding high-impact activities initially.
- Bilateral Considerations: If staged, rehabilitation for the first side will be further advanced, but care must be taken not to overload the contralateral, potentially dysplastic, hip.
Phase 4: Return to Activity (Months 6+)
- Full Activity: Gradual return to full activities, including sports, based on functional assessment, strength recovery, and absence of pain.
- Maintenance: Continued emphasis on strength, flexibility, and core stability to prevent recurrence of symptoms or complications.
- Long-term Follow-up: Regular clinical and radiographic follow-up to monitor joint health and identify any late complications.


Summary of Key Literature / Guidelines
The landscape of conservative hip surgery for dysplasia has been significantly shaped by landmark studies and evolving consensus guidelines.
-
Ganz PAO Outcomes: The original series by Ganz and subsequent long-term follow-up studies have consistently demonstrated the efficacy of PAO in preserving the native hip joint. Studies report hip survival rates of 70-90% at 20 years post-surgery in well-selected patients, often delaying or preventing the need for total hip arthroplasty. The key prognostic factors for long-term success include younger age at surgery, minimal pre-existing degenerative changes, and optimal acetabular correction.
- Siebenrock et al. (2003) showed 20-year survival rates of 75% for PAO, emphasizing the importance of preventing or minimizing osteoarthritis.
- Leunig et al. (2009) highlighted the critical role of avoiding residual impingement and achieving adequate coverage in all planes.
-
Role of Arthroscopy: The integration of hip arthroscopy with PAO (or as a primary treatment for borderline dysplasia) has become more prevalent. Arthroscopy can address concomitant intra-articular pathologies such as labral tears, chondral defects, and femoroacetabular impingement (FAI) that may not be fully corrected by osteotomy alone. This combined approach aims to optimize the intra-articular environment prior to or during acetabular reorientation.
-
Bilateral Dysplasia Management: While PAO is effective unilaterally, the management of bilateral dysplasia requires careful consideration.
- Staged Procedures: The overwhelming consensus favors staged bilateral PAO, with an interval of typically 3-6 months between procedures. This allows for adequate recovery from the first surgery, minimizes operative risks (e.g., blood loss, prolonged anesthesia, DVT risk), and facilitates a more manageable rehabilitation process for the patient.
- Simultaneous Bilateral PAO: Rarely performed, primarily in highly specialized centers with strict selection criteria, due to significantly increased blood loss, operative time, higher risk of complications (e.g., severe anemia, coagulopathy, prolonged ileus, greater systemic stress), and more challenging immediate post-operative care and rehabilitation. The decision to pursue simultaneous surgery requires careful discussion with the patient regarding these risks and benefits.
- Outcome Differences: Studies on staged bilateral PAO have shown comparable clinical outcomes to unilateral PAO, with similar rates of pain relief and functional improvement, despite the extended overall recovery period.
-
Predictors of Failure: Identified predictors of less favorable outcomes or failure include older age (>40-45 years) at surgery, advanced pre-operative osteoarthritis (Tönnis grade >1), presence of severe labral damage or significant cartilage loss, and inadequate surgical correction (residual dysplasia or impingement).
-
Imaging Guidelines: The use of advanced imaging (CT with 3D reconstruction, MRI) is standard of care for comprehensive pre-operative assessment. These modalities are crucial for quantifying dysplasia, assessing articular cartilage and labral status, and planning the osteotomy vectors.
-
Rehabilitation Guidelines: While standardized protocols exist, individualized rehabilitation plans are essential, adapting to patient progress, bone healing, and potential complications. Early, protected motion and gradual weight-bearing progression are cornerstones.

Conservative hip surgery, particularly the PAO, represents a significant advancement in the management of symptomatic hip dysplasia, offering a durable joint-preserving option for selected patients. For those with bilateral dysplasia, a carefully staged approach remains the standard of care, maximizing patient safety and optimizing long-term functional outcomes. Continuous research and refinement of techniques, coupled with stringent patient selection, will further enhance the efficacy and expand the indications for these complex yet rewarding procedures.
Clinical & Radiographic Imaging


You Might Also Like