Mastering the Anterolateral Approach to the Elbow: Anatomy & Surgical Applications
Key Takeaway
The anterolateral approach to the elbow is a versatile surgical exposure providing safe access to the lateral and anterior compartments. It's crucial for treating complex capitellum and radial head fractures, nerve entrapments like radial tunnel syndrome, and distal biceps avulsions. This approach leverages specific internervous planes, protecting vital neurovascular structures, particularly the radial nerve.
Introduction & Epidemiology
The anterolateral approach to the elbow is a versatile and fundamental surgical exposure providing access to the lateral and anterior compartments of the elbow joint and the proximal forearm. It is a critical pathway for addressing a myriad of pathologies involving the distal humerus, proximal radius, and their associated soft tissues. This approach leverages specific internervous planes, offering a relatively safe corridor to articulate structures and surrounding neurovascular elements, particularly the radial nerve and its branches.
Historically, surgical approaches to the elbow have evolved to minimize iatrogenic injury while maximizing visualization. The anterolateral approach gained prominence due to its efficacy in treating complex fractures, nerve entrapments, and other conditions that require direct anterior access to the radiocapitellar joint and proximal radius. Its design minimizes disruption to major muscle groups and preserves the integrity of the critical lateral collateral ligament (LCL) complex, which is paramount for elbow stability.
Epidemiologically, the conditions addressed by the anterolateral approach are diverse. Capitellum fractures, while relatively uncommon (approximately 1% of all elbow fractures), are intra-articular and often require precise open reduction and internal fixation to restore articular congruity and prevent post-traumatic arthrosis. Radial head fractures, significantly more common (17-20% of all elbow fractures), can occasionally necessitate an anterolateral approach, particularly for complex patterns, associated nerve palsies, or when combined with other injuries. Nerve compression syndromes, such as radial tunnel syndrome involving the posterior interosseous nerve (PIN), are less frequent but debilitating, and this approach provides direct access for decompression. Distal biceps avulsions, though less common than shoulder biceps pathologies, are functionally significant and often require operative repair via an anterolateral approach to restore supination and flexion strength. The utility of this approach across these varied pathologies underscores its importance in the orthopedic surgeon's armamentarium for elbow reconstruction and trauma.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy and biomechanics is paramount for safe and effective execution of the anterolateral approach.
Osteology
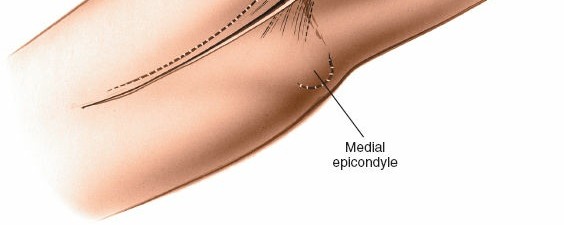
- Distal Humerus : The capitellum forms the lateral articulating surface, important for radiocapitellar articulation. The lateral epicondyle serves as the origin for the common extensor tendon.
- Proximal Radius : The radial head articulates with the capitellum and the radial notch of the ulna. The radial neck connects the head to the radial tuberosity, the insertion point for the biceps brachii tendon.
- Proximal Ulna : The coronoid process is a key stabilizer, and the radial notch articulates with the radial head.
Ligamentous Structures
The anterolateral approach generally avoids direct violation of the critical
Lateral Collateral Ligament (LCL) complex
, which includes:
*
Radial collateral ligament (RCL)
: Originates from the lateral epicondyle, blending with the annular ligament.
*
Lateral ulnar collateral ligament (LUCL)
: Originates from the lateral epicondyle and inserts onto the supinator crest of the ulna. This is the primary posterolateral stabilizer of the elbow.
*
Annular ligament
: Encircles the radial head, maintaining its articulation with the ulna.
The anterior capsule is often incised during the approach to gain joint access, but careful repair is crucial.
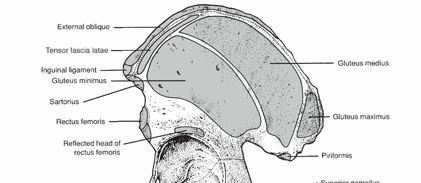
Musculature
The approach navigates between several muscle groups:
*
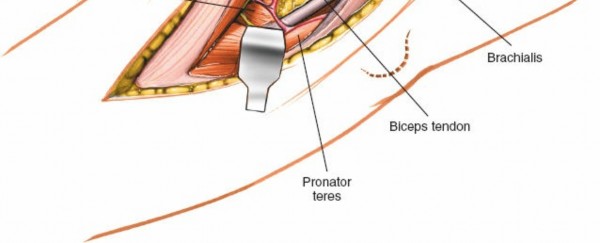
Brachialis
: Originates from the anterior humerus, inserts onto the coronoid process and ulnar tuberosity. Innervated by the musculocutaneous nerve (and a small contribution from the radial nerve).
*
Brachioradialis
: Originates from the lateral supracondylar ridge of the humerus, inserts onto the styloid process of the radius. Innervated by the radial nerve.
*
Extensor Carpi Radialis Longus (ECRL)
: Originates from the lateral supracondylar ridge, inserts onto the base of the second metacarpal. Innervated by the radial nerve.
*
Extensor Carpi Radialis Brevis (ECRB)
: Originates from the lateral epicondyle, inserts onto the base of the third metacarpal. Innervated by the radial nerve (deep branch).
*
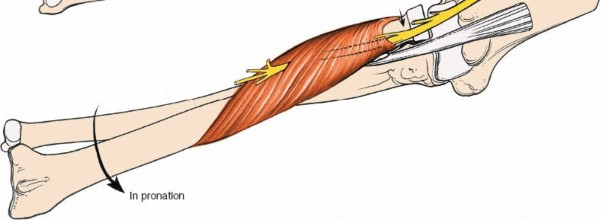
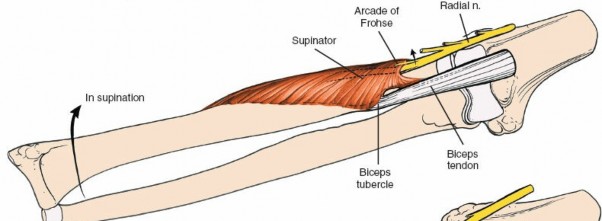
Supinator
: Originates from the lateral epicondyle, supinator crest of the ulna, and LCL complex. Inserts onto the proximal radius. The posterior interosseous nerve (PIN) passes through it. Innervated by the posterior interosseous nerve.
*
Biceps Brachii
: Inserts onto the radial tuberosity. Innervated by the musculocutaneous nerve.
Neurovascular Structures
-
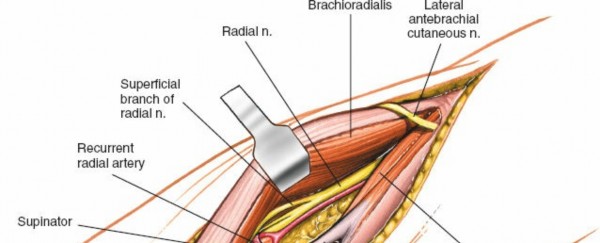
Radial Nerve
: This is the most critical structure to identify and protect. Proximal to the elbow, it courses anterior to the lateral epicondyle, deep to the brachioradialis and ECRL. At the level of the radial head, it typically divides into:
- Superficial Radial Nerve (SRN) : Sensory branch, often closely associated with the brachioradialis.
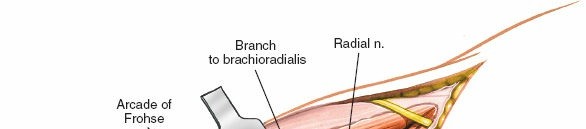
- Posterior Interosseous Nerve (PIN) : Motor branch, dives into the supinator muscle, passing through the Arcade of Frohse (a fibrous arch formed by the superficial head of the supinator).
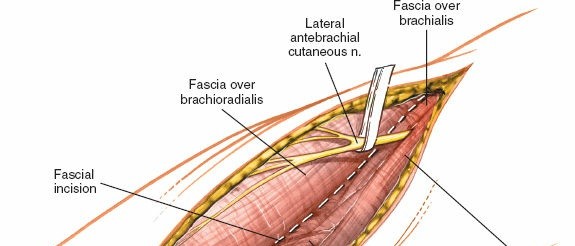
- Lateral Antebrachial Cutaneous Nerve (LABCN) : A sensory branch of the musculocutaneous nerve, located subcutaneously anterior to the elbow joint, often accompanies the cephalic vein. At risk during skin incision and superficial dissection.
- Radial Recurrent Artery : Arises from the radial artery and ascends proximally between the brachioradialis and brachialis, forming an anastomotic network around the elbow. It can be encountered during deep dissection.
Internervous Plane
The anterolateral approach utilizes a safe internervous plane between:
*
Medial/Anteriorly
: Brachialis muscle (innervated by the musculocutaneous nerve, and sometimes a branch from the radial nerve).
*
Lateral/Posteriorly
: Brachioradialis and Extensor Carpi Radialis Longus (innervated by the radial nerve).
This plane allows for retraction of muscle groups without compromising their innervation, provided the radial nerve proper is carefully identified and protected, particularly as it exits from under the brachioradialis and ECRL and subsequently divides.
Biomechanics
The elbow is a complex hinge joint with rotation capabilities. Stability is conferred by the congruent articular surfaces and the collateral ligament complexes. The radiocapitellar joint bears a significant portion of axial load, and its integrity is vital for load transmission and pronation/supination. Injuries to the capitellum or radial head can significantly disrupt elbow kinematics, leading to pain, stiffness, instability, or arthrosis if not anatomically reduced and stabilized. The biceps tendon is a powerful supinator and elbow flexor, and its avulsion results in significant functional deficit.
Indications & Contraindications
The anterolateral approach is highly versatile, indicated for a range of pathologies affecting the lateral and anterior elbow compartments.
Indications
- Open Reduction and Internal Fixation (ORIF) of Capitellum Fractures : This includes classical Hahn-Steinthal (coronal shear) and Kocher-Lorenz (osteochondral) fractures. The approach provides direct visualization for anatomical reduction and stable fixation, often with headless compression screws.
- Excision of Tumors of the Proximal Radius : Benign or low-grade malignant lesions such as osteochondromas, giant cell tumors, or aneurysmal bone cysts can be accessed for marginal or en bloc excision.
- Treatment of Aseptic Necrosis of the Capitellum : Conditions like Panner's disease (osteochondrosis in children) or osteochondritis dissecans (OCD) in adolescents and young adults may necessitate débridement, loose body removal, or drilling procedures.
- Drainage of Infection from the Elbow Joint : Particularly for septic arthritis affecting the anterior or lateral compartments, allowing for thorough irrigation and débridement.
-
Treatment of Neural Compression Lesions
:
- Proximal Posterior Interosseous Nerve (PIN) Compression : Decompression of the PIN, most commonly at the Arcade of Frohse (radial tunnel syndrome), or other fibrous bands within the supinator.
- Proximal Superficial Radial Nerve Compression : Less common, but can be accessed.
- Radial Head Fractures with Radial Nerve or PIN Palsy : Direct exposure allows for assessment and repair/decompression of the nerve alongside fracture management.
- Treatment of Distal Biceps Avulsion : Repair of the biceps tendon to the radial tuberosity, often involving bone tunnel fixation techniques.
- Total Elbow Replacements (TER) : While posterior approaches are more common for primary TER, the anterolateral approach can be utilized for specific unconstrained or semi-constrained prostheses, or in revision cases where extensive anterior exposure is required.
- Open Reduction and Internal Fixation (ORIF) or Excision/Replacement of Radial Head Fractures : For complex or comminuted radial head fractures (Mason type III, IV), particularly when associated with other injuries (e.g., terrible triad) or requiring specific plating configurations.
- Excision of Symptomatic Osteophytes or Loose Bodies : From the anterior and lateral compartments of the elbow.
- Synovectomy : For inflammatory arthropathies when anterior synovial pannus is significant.
Contraindications
- Active Local Infection (relative) : While indicated for drainage, performing complex ORIF or implant insertion in the presence of active, uncontrolled infection is generally contraindicated.
- Severe Soft Tissue Compromise or Scarring : From previous surgeries, trauma, or burns, which may increase the risk of wound complications or difficulty identifying critical structures.
- Known Severe Vascular Compromise : Of the extremity, which could be exacerbated by tourniquet use or surgical manipulation.
- Pathologies Better Addressed by Other Approaches : E.g., medial epicondyle fractures (medial approach), posterior elbow instability (direct posterior), or complex ulnar nerve entrapment (medial).
- Extensive Comminution with Limited Fixation Points : In some severe fracture patterns, the approach may not provide adequate visualization of all fragments or sufficient access for stable fixation.
Operative vs. Non-Operative Indications
| Indication Type | Operative Treatment (Anterolateral Approach) | Non-Operative Treatment |
|---|---|---|
| Fractures | Displaced capitellum fractures (Hahn-Steinthal, Kocher-Lorenz) | Non-displaced capitellum fractures (rarely, short immobilization) |
| Unstable radial head fractures (Mason II-IV) requiring ORIF/replacement | Stable, minimally displaced radial head fractures (Mason I, some II) | |
| Radial head fractures with associated nerve palsy requiring direct decompression | Radial head fractures without nerve symptoms | |
| Tendinous | Complete distal biceps tendon avulsion from radial tuberosity | Partial biceps tendon tears (often managed non-operatively initially) |
| Nerve Entrapment | Symptomatic radial tunnel syndrome (PIN compression) refractory to conservative measures | Early or mild radial tunnel syndrome (rest, activity modification, NSAIDs, PT) |
| Acute iatrogenic radial nerve injury with functional deficit | Neuropraxia observed with spontaneous recovery | |
| Other | Symptomatic tumors/lesions of proximal radius (e.g., GCT, osteochondroma) | Asymptomatic, stable bone lesions |
| Symptomatic aseptic necrosis of capitellum (OCD) requiring débridement/drilling, loose body removal | Early-stage Panner's disease, asymptomatic OCD with intact cartilage | |
| Septic arthritis (anterior/lateral compartments) requiring open irrigation and débridement | Early septic arthritis responding to aspiration and antibiotics (less common) | |
| Recalcitrant symptomatic loose bodies or osteophytes | Asymptomatic loose bodies or osteophytes |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing exposure, minimizing complications, and ensuring surgical efficiency.
Pre-Operative Planning
- Clinical Assessment : A comprehensive history focusing on mechanism of injury, prior surgeries, and comorbidities. A detailed physical examination to assess neurovascular status, range of motion (if possible), and soft tissue integrity.
-
Imaging Review
:
- Standard Radiographs : AP, lateral, and oblique views of the elbow.
- Computed Tomography (CT) Scan : Essential for complex intra-articular fractures (capitellum, radial head), providing detailed information on fracture morphology, displacement, comminution, and articular involvement. 3D reconstructions are invaluable for pre-operative templating.
- Magnetic Resonance Imaging (MRI) : Indicated for soft tissue pathologies such as tumors, osteochondral lesions (OCD), aseptic necrosis, and nerve compression syndromes. It can delineate tumor margins, cartilage damage, and nerve pathology.
- Nerve Conduction Studies/EMG : For suspected nerve entrapment syndromes, to confirm diagnosis and localize compression.
- Surgical Strategy : Based on imaging, determine the exact pathology, fixation requirements (plate type, screw size/length, number of screws), need for bone grafting, implant choice (e.g., radial head prosthesis), and anticipated steps for nerve decompression or tendon repair.
- Equipment Preparation : Ensure all necessary instrumentation is available, including specific fracture trays, nerve dissection tools, vascular loops for nerve retraction, appropriate implants (screws, plates, radial head implants, suture anchors), and fluoroscopy unit.
- Anesthetic Consultation : Discuss regional nerve blocks (e.g., supraclavicular or interscalene brachial plexus block) in addition to general anesthesia for post-operative pain management.
- Antibiotic Prophylaxis : Administer intravenous prophylactic antibiotics pre-incision.
Patient Positioning
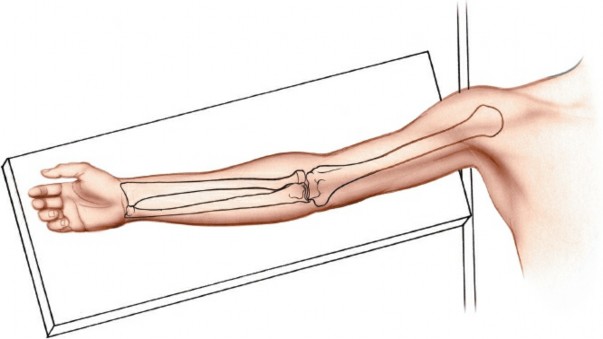
- Supine Position : The patient is placed supine on the operating table.
- Arm Board Placement : The ipsilateral arm is abducted and placed on a well-padded arm board, positioned perpendicular to the body. This allows for elbow flexion and extension during the procedure to assess reduction and stability.
-
Tourniquet Application
: A pneumatic tourniquet is applied high on the upper arm, over adequate padding.
- Exsanguination : The limb is exsanguinated either by elevation for 3 to 5 minutes or by applying a soft rubber bandage (Esmarch bandage) prior to inflating the tourniquet to a pressure typically 100-150 mmHg above systolic blood pressure.
- Draping : The limb is sterilely prepped and draped from the mid-humerus to the hand, allowing for full range of motion of the elbow and wrist intraoperatively. C-arm draping should also be considered if fluoroscopy is anticipated.
Detailed Surgical Approach / Technique
The anterolateral approach requires meticulous dissection to protect critical neurovascular structures while achieving adequate exposure of the pathology.
1. Skin Incision
-
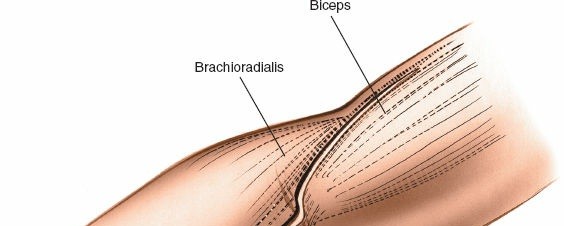
A longitudinal skin incision is made, typically 8-12 cm in length, centered over the lateral epicondyle. It starts approximately 3-4 cm proximal to the lateral epicondyle and extends distally along the forearm, aligning with the intermuscular interval between the brachialis and brachioradialis/ECRL. The incision should be generous enough to allow for appropriate retraction without excessive tension.

- Pitfall : Incising too far anteriorly risks injury to the lateral antebrachial cutaneous nerve.
-
Technique
: Incise the skin and subcutaneous tissue. Identify and protect any superficial veins and the lateral antebrachial cutaneous nerve, which is typically found anterior to the elbow joint.
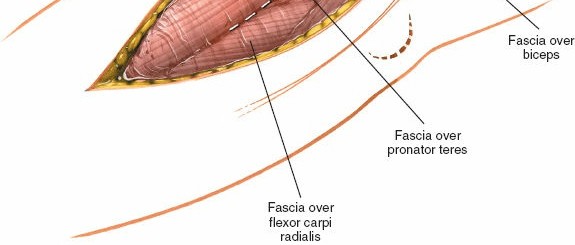
2. Deep Fascia and Muscle Identification
-
Incise the deep fascia longitudinally. The underlying muscles, primarily the brachioradialis and extensor carpi radialis longus (ECRL) laterally, and the brachialis more medially/anteriorly, are identified.

-
Internervous Plane
: The key to this approach is entering the internervous plane between the brachialis (innervated by the musculocutaneous nerve) and the brachioradialis/ECRL (innervated by the radial nerve). This plane is located slightly anterior to the lateral epicondyle.
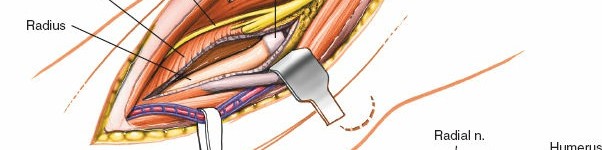
3. Radial Nerve Identification and Protection
-
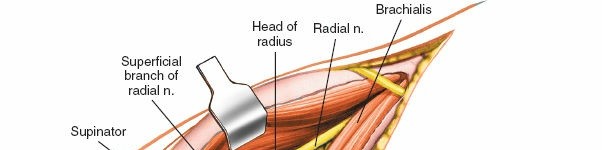
The radial nerve is the most crucial structure to protect. It lies deep to the brachioradialis and ECRL. Retract the brachioradialis and ECRL muscles laterally/posteriorly. This exposes the deeper structures including the radial nerve.

- Carefully dissect through the fat and connective tissue. The radial nerve will be identified typically anterior to the lateral epicondyle, between the brachialis and brachioradialis/ECRL. Proximal to the elbow, it passes between the brachialis and brachioradialis.
- As the dissection proceeds distally, the radial nerve divides into its superficial radial nerve (SRN) and posterior interosseous nerve (PIN) branches. The SRN continues distally with the brachioradialis, while the PIN dives into the supinator muscle.
-
Critical Step
: Identify the radial nerve proper and gently isolate it. It is often secured with a vascular loop or small rubber vessel loop for careful retraction.
-
For access to the proximal radius and PIN, the supinator muscle must be addressed. The PIN passes through the two heads of the supinator, often beneath the fibrous band known as the
Arcade of Frohse
.
-
Careful dissection and release of the Arcade of Frohse or the superficial head of the supinator may be necessary to expose the PIN and underlying proximal radius.
- Warning : Avoid aggressive traction or direct trauma to the radial nerve and its branches.
4. Joint Exposure (Capsulotomy/Arthrotomy)
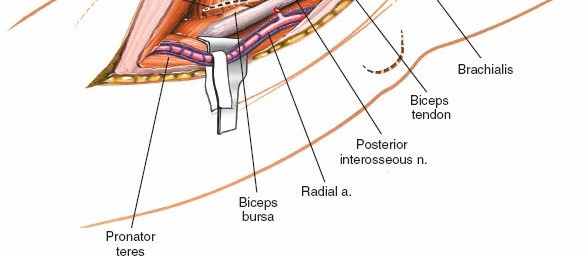
- Once the radial nerve and its branches are protected and retracted, the anterior joint capsule can be visualized.
-
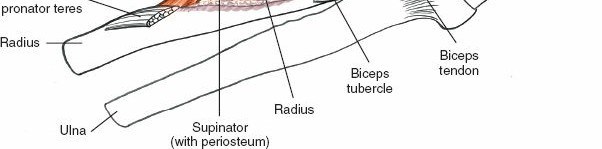
The capsule is incised longitudinally, typically anterior to the lateral collateral ligament complex, to expose the radiocapitellar joint and the anterior aspect of the distal humerus and proximal radius.

-
Exposure
: Retraction of the brachialis and brachioradialis/ECRL (with the radial nerve) provides an excellent view of the capitellum, radial head, and often the coronoid process.
5. Procedure-Specific Steps
a. Capitellum Fracture ORIF
-
Fracture Visualization
: The capitellum fracture, often a coronal shear type, is clearly visible. Loose fragments may be present.

- Reduction : Gentle manipulation, often involving elbow flexion/extension and pronation/supination, combined with direct pressure, is used to achieve anatomical reduction of the capitellum fragment to the distal humerus. Articular congruity is paramount.
- Temporary Fixation : K-wires are often used for temporary stabilization once reduction is achieved.
-
Definitive Fixation
: Typically achieved with one or more small-profile, headless compression screws inserted from posterior to anterior, across the fracture site. Alternatively, a small anterior plate may be used for specific fracture patterns. The screws should be countersunk and not protrude into the joint.
- Assessment : Evaluate stability and range of motion through a full arc, confirming no impingement or loss of reduction. Fluoroscopy can confirm screw placement and reduction.
b. Radial Head Fracture ORIF/Excision/Replacement
- Exposure : The radial head is exposed. If comminuted, fragments are carefully assessed.
- ORIF : For simple, displaced fractures, reduction and fixation with small headless screws or a low-profile radial head plate can be performed.
- Excision : For severely comminuted or irreparable fractures where replacement is not indicated, radial head excision may be performed.
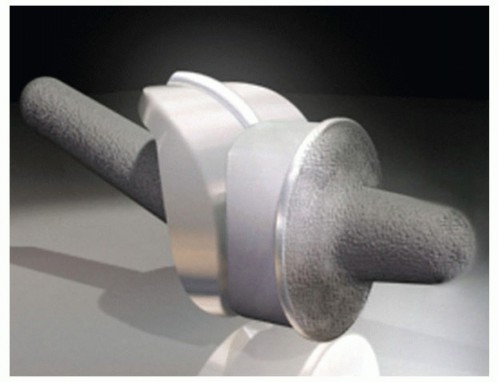
- Radial Head Replacement : For specific Mason type III fractures or those associated with terrible triad injuries, a radial head prosthesis may be inserted. The size is templated, and the component is press-fit or cemented.
c. Posterior Interosseous Nerve Decompression
- After identifying and protecting the radial nerve and its bifurcation, the PIN is traced as it enters the supinator.
- Arcade of Frohse Release : The fibrous arch of the Arcade of Frohse is carefully incised longitudinally, releasing the nerve. Any other constricting bands within the supinator or at its distal exit are also released.
- Confirm free gliding of the nerve.
d. Distal Biceps Tendon Repair
- The ruptured distal biceps tendon is identified. Often, it has retracted proximally.
- The radial tuberosity is prepared. A single- or two-incision technique can be used, but the anterolateral approach provides access to the tuberosity.
- The tendon is retrieved, débrided, and reattached to the radial tuberosity, typically using suture anchors or through bone tunnels.
6. Closure
- Capsule Repair : The anterior joint capsule is meticulously repaired with absorbable sutures to help restore joint stability and prevent capsular scarring.
- Muscle Reapproximation : The muscle layers are reapproximated anatomicaly. The brachioradialis and ECRL are allowed to fall back into place, covering the radial nerve.
- Deep Fascia : Repair the deep fascia.
-
Subcutaneous Tissue and Skin
: Close in layers with absorbable sutures for subcutaneous tissue and non-absorbable sutures or staples for the skin.

-
Dressing and Immobilization
: Apply a sterile dressing and typically a bulky soft dressing or a splint (e.g., posterior long arm splint) to protect the repair and provide comfort.
Complications & Management
Despite meticulous surgical technique, complications can arise following an anterolateral approach to the elbow. Understanding their incidence and appropriate management strategies is crucial.
| Complication | Incidence (Approx.) | Salvage / Management Strategies |
|---|---|---|
| Radial Nerve/PIN Palsy | 0.5-5% | Post-op: Observe for spontaneous recovery (up to 6-12 months). Persistent: Nerve conduction studies/EMG to confirm injury type. Neuropraxia: Conservative management (splinting, PT). Axonotmesis/Neurotmesis: Surgical exploration, neurolysis, repair, or grafting; tendon transfers for irreparable deficits. |
| Lateral Antebrachial Cutaneous Nerve (LABCN) Injury | 5-15% (sensory) | Post-op: Primarily sensory loss or neuroma formation. Management: Reassurance, desensitization therapy. Persistent Symptomatic Neuroma: Surgical excision or burial. |
| Infection | 1-3% | Superficial: Oral antibiotics, local wound care. Deep: Urgent surgical irrigation and débridement, IV antibiotics (culture-guided), possible hardware removal; retention of stable implants with debridement. |
| Heterotopic Ossification (HO) | 5-20% (clinical) | Prophylaxis: Indomethacin (NSAIDs) for 3-6 weeks post-op or low-dose radiation in high-risk patients. Established HO: Aggressive physical therapy. Symptomatic HO (impinging ROM): Surgical excision after maturation (6-12 months). |
| Stiffness / Loss of Motion | 10-30% | Early: Aggressive physical therapy, dynamic/static splinting. Persistent: Manipulation under anesthesia, arthroscopic or open arthrolysis/capsulectomy. |
| Nonunion / Malunion (Fractures) | 5-10% (fracture dependent) | Nonunion: Revision ORIF with bone grafting, biomechanically stronger fixation. Malunion: Corrective osteotomy (if symptomatic and functional deficit). |
| Hardware-Related Issues | 10-20% | Prominence/Pain: Hardware removal after fracture healing is complete. Loose/Broken Hardware: Revision fixation, addressing underlying causes (e.g., nonunion). |
| Vascular Injury | <0.1% | Acute: Immediate vascular repair by microsurgical techniques. |
| Lateral Epicondylitis / Tendinopathy | Variable | Post-op: Rest, NSAIDs, physical therapy. Persistent: Local injections, rarely surgical release. |
Detailed Management Considerations
- Radial Nerve/PIN Palsy : This is the most feared complication. Traction injury is common, leading to neuropraxia which typically resolves within weeks to months. Direct transection is rare but devastating. Meticulous identification, isolation, and protection of the radial nerve and its branches during the approach are paramount. If a post-operative deficit is noted, serial neurological exams are critical. Electrophysiological studies (EMG/NCS) can help differentiate neuropraxia from axonotmesis or neurotmesis. For persistent or complete deficits, surgical exploration should be considered.
- Infection : Early recognition and aggressive management are key. Deep infections typically require prompt surgical débridement, copious irrigation, culture-directed intravenous antibiotics, and potentially hardware removal after bony consolidation.
- Heterotopic Ossification (HO) : Can severely limit elbow range of motion. Risk factors include extensive soft tissue trauma, prolonged immobilization, and specific patient conditions (e.g., head injury). Prophylactic measures (e.g., NSAIDs like indomethacin or pre-operative/post-operative radiation therapy) are often used in high-risk cases. Surgical excision of mature HO may be necessary if it significantly restricts function.
- Stiffness : A common sequela of elbow surgery due to capsular scarring, HO, or inadequate rehabilitation. Early, controlled motion protocols are crucial to mitigate this. If stiffness persists despite aggressive therapy, manipulation under anesthesia or formal open/arthroscopic arthrolysis may be required to restore functional range of motion.
- Nonunion/Malunion : Particularly relevant in fracture cases. Causes can include inadequate reduction, unstable fixation, poor bone quality, or insufficient biological healing. Revision surgery with robust fixation and bone grafting (autograft or allograft) may be necessary. Corrective osteotomy may be indicated for symptomatic malunions.
- Hardware-Related Issues : Common due to the superficial location of some hardware, especially around the lateral epicondyle. Symptomatic hardware, such as prominent screws or plates, typically warrants removal once fracture healing is complete.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing outcomes and restoring function after an anterolateral elbow approach. Protocols vary depending on the specific pathology, surgical repair stability, and patient factors. The general principles include protecting the surgical repair, managing pain and swelling, and progressively restoring range of motion and strength.
General Principles
- Pain Management : Adequate analgesia is essential to facilitate early mobilization.
- Swelling Reduction : Elevation and gentle compression (e.g., soft bandage) help minimize edema.
- Wound Care : Regular inspection of the incision for signs of infection.
- Protection of Repair : The specific surgical repair (e.g., fracture fixation, tendon repair) dictates the initial level of immobilization and controlled motion.
- Patient Education : Clear instructions on activity restrictions, exercises, and warning signs.
Phase 1: Immobilization and Early Protected Motion (Weeks 0-2/3)
- Goals : Protect surgical repair, minimize pain and swelling, initiate gentle motion (within safe limits).
-
Immobilization
:
- Often a posterior long arm splint or hinged elbow brace is applied post-operatively, typically set at an arc that protects the repair (e.g., 30-90 degrees flexion for capitellum fractures, or specific limitations for biceps repair).
- For PIN decompression, immobilization is usually minimal, focused on comfort.
-
Motion
:
- Gentle, gravity-assisted passive range of motion (PROM) or active-assisted range of motion (AAROM) of the elbow, within physician-defined safe arcs.
- Forearm pronation/supination (if allowed and stable), wrist and hand exercises.
- Shoulder ROM exercises to prevent stiffness.
- NO active resisted elbow flexion or supination for distal biceps repair.
- Therapeutic Modalities : Ice, elevation.
- Nerve Glides : If PIN decompression performed, gentle radial nerve gliding exercises may be initiated.
Phase 2: Intermediate Mobility and Gradual Strengthening (Weeks 3-6/8)
- Goals : Increase elbow ROM, begin gentle strengthening, manage scar tissue.
-
Immobilization
:
- Transition from static splint to a dynamic or hinged elbow brace, gradually increasing the allowed arc of motion as tolerated and as dictated by healing.
- The brace may be removed for exercises.
-
Motion
:
- Progressive increase in active and passive elbow flexion/extension, and pronation/supination, aiming for near full physiological motion by the end of this phase.
- Joint mobilization techniques by therapist.
-
Strengthening
:
- Light isometric exercises for elbow flexors, extensors, pronators, and supinators (if not contraindicated by tendon repair).
- Gentle grip strengthening.
- Scar Management : Massage, silicone sheeting.
Phase 3: Advanced Strengthening and Functional Return (Weeks 8-12+)
- Goals : Achieve full pain-free ROM, restore strength, improve endurance and proprioception.
- Brace : Discontinue brace as appropriate, based on stability and patient confidence.
-
Strengthening
:
- Progressive resisted exercises for all elbow and forearm muscles using resistance bands, light weights, and body weight.
- Eccentric strengthening.
- Core and scapular stabilization exercises.
- Proprioception and Neuromuscular Control : Exercises such as weight-bearing activities (e.g., closed kinetic chain exercises), balance boards, and sport-specific drills.
- Functional Activities : Gradual return to light daily activities.
Phase 4: Return to Activity / Sport-Specific Training (Months 3-6+)
- Goals : Maximizing strength, power, endurance, and sport/work-specific function.
-
Training
:
- High-level strengthening and conditioning.
- Plyometric exercises (if appropriate and cleared).
- Sport-specific drills, gradual increase in intensity and volume.
- Return to Play/Work : Gradual, physician-guided return to unrestricted sports or heavy occupational activities once strength, ROM, and stability are fully restored and pain-free. This phase can extend significantly depending on the nature of the original injury and the demands of the patient's activities.
Specific Considerations for Different Pathologies
- Capitellum Fractures : Strict adherence to ROM limits in early phases to protect fixation, especially if small fragments or tenuous fixation.
- Distal Biceps Repair : Avoid active resisted supination and elbow flexion for 6-8 weeks. Protect the repair in a flexed position initially.
- Nerve Decompression : Early, gentle nerve gliding exercises are encouraged. No specific restrictions on elbow motion other than comfort.
Regular communication between the surgeon, physical therapist, and patient is paramount to tailor the rehabilitation program and ensure adherence while navigating potential complications like stiffness or pain.
Summary of Key Literature / Guidelines
The anterolateral approach to the elbow is well-established in orthopedic literature, with guidelines informed by decades of clinical experience and anatomical studies. Key themes revolve around minimizing neurovascular injury, achieving anatomical reduction, and implementing appropriate post-operative rehabilitation.
Surgical Anatomy and Radial Nerve Protection:
Classic anatomical studies by Spinner (1968) and more contemporary works by Brand (1998) and others have meticulously detailed the course of the radial nerve and its branches around the elbow, emphasizing the importance of identifying the internervous plane between the brachialis and brachioradialis/ECRL. These studies highlight the variability of the radial nerve's bifurcation and the Arcade of Frohse, underscoring the need for careful, layer-by-layer dissection. The AO Foundation principles consistently advocate for direct visualization and protection of the radial nerve during any lateral-based elbow approach.
Capitellum Fractures:
The management of capitellum fractures, particularly the coronal shear patterns (Hahn-Steinthal, Kocher-Lorenz), has seen a strong consensus shift towards anatomical open reduction and internal fixation (ORIF) to restore articular congruity. Techniques often involve the use of small-profile headless compression screws inserted from posterior to anterior, providing stable fixation while avoiding joint surface prominence. Key literature, including comprehensive reviews and case series, demonstrates superior outcomes with ORIF compared to historical methods of excision or non-operative management for displaced fractures, emphasizing the importance of this approach for direct visualization and precise reduction.
Radial Head Fractures:
While the posterolateral (Kocher) approach is often favored for radial head fractures due to its exposure and minimal neurovascular risk, the anterolateral approach gains utility in specific scenarios. This includes situations requiring anterior plating, concurrent repair of the distal biceps, or when dealing with complex fractures where the radial nerve is suspected to be involved or entrapped. Studies on radial head arthroplasty sometimes discuss the anterolateral approach as an alternative, offering direct visualization of the radial tuberosity for potential biceps repair, though it might not provide as broad a view of the radial neck as other approaches.
Posterior Interosseous Nerve (PIN) Decompression (Radial Tunnel Syndrome):
The anterolateral approach is the standard for surgical decompression of the PIN in cases of radial tunnel syndrome refractory to conservative management. Landmark papers and surgical texts describe the identification and release of potential compression points, including the fibrous bands of the superficial head of the supinator (Arcade of Frohse), recurrent radial vessels, fibrous edge of the ECRB, and fascia of the brachialis. Outcomes are generally favorable for correctly diagnosed and surgically managed cases, with improvement in pain and motor function.
Distal Biceps Tendon Repair:
The anterolateral approach, either as a single anterior incision or part of a two-incision technique, is widely accepted for distal biceps tendon repair. Literature comparing single-incision (anterior) versus two-incision techniques suggests comparable functional outcomes, with the single-incision anterolateral approach potentially reducing the risk of synostosis. However, meticulous nerve protection remains crucial.
Total Elbow Arthroplasty (TEA):
While the posterior approach (e.g., triceps-splitting, triceps-sparing) is predominantly used for TEA, the anterolateral approach can be considered for specific unconstrained prostheses or in revision scenarios where the anterior capsule and structures require direct access. Its role in primary TEA is less common due to the extensive dissection required for full articular visualization compared to posterior options.
Rehabilitation Protocols:
Guidelines from various orthopedic societies (e.g., AAOS, AO Trauma) consistently emphasize early controlled motion and progressive strengthening, tailored to the specific injury and stability of the surgical repair. The literature supports structured, progressive rehabilitation programs to prevent stiffness, promote healing, and restore functional independence, with variations based on fracture stability, tendon integrity, and nerve status.
In conclusion, the anterolateral approach is a robust and versatile surgical pathway for addressing a focused spectrum of elbow pathologies. Its continued relevance is supported by its ability to provide direct access to critical structures while, when performed meticulously, minimizing iatrogenic injury to surrounding neurovascular elements. Adherence to established anatomical principles, careful surgical technique, and structured post-operative rehabilitation remains paramount for achieving optimal clinical outcomes.
Clinical & Radiographic Imaging


You Might Also Like