Precision Anterolateral Approach: Joint & Subacromial Surgery Guide
Key Takeaway
This topic focuses on Precision Anterolateral Approach: Joint & Subacromial Surgery Guide, The anterolateral approach offers excellent exposure of the acromioclavicular joint and subacromial space, including the underlying coracoacromial ligament and supraspinatus tendon. Its uses include anterior shoulder decompression, rotator cuff repair, biceps tendon stabilization, and excision of acromioclavicular joint osteophytes. This approach remains clinically relevant for extensive degenerative rotator cuff disease.
Precision Anterolateral Approach: Joint & Subacromial Surgery Guide
Introduction & Epidemiology
The anterolateral approach to the shoulder offers a versatile and effective exposure for a myriad of pathologies affecting the acromioclavicular (AC) joint and the subacromial space. Historically, open approaches were the mainstay for shoulder surgery, providing direct visualization and tactile feedback. While arthroscopic techniques have revolutionized many aspects of shoulder care, the open anterolateral approach retains significant relevance for specific indications, complex revisions, or when direct, robust exposure is deemed advantageous. Its principal utility lies in addressing conditions such as subacromial impingement, rotator cuff tears, long head of biceps tendon pathology, and degenerative or traumatic afflictions of the AC joint.
The prevalence of shoulder pathologies requiring surgical intervention is substantial. Rotator cuff tears affect a significant portion of the adult population, with incidence increasing with age. Subacromial impingement syndrome remains a leading cause of shoulder pain, often coexisting with rotator cuff pathology. AC joint osteoarthritis and traumatic AC joint separations are also common, contributing to considerable patient morbidity. Understanding the nuances of the anterolateral approach is therefore crucial for orthopedic surgeons managing these prevalent conditions, enabling precise surgical execution and optimal patient outcomes. This guide aims to provide a comprehensive, high-yield overview of the anterolateral approach from a medical educator's perspective, tailored for orthopedic surgeons, residents, and medical students.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is paramount for safe and effective execution of the anterolateral approach.
Bony Landmarks
- Acromion: The lateral extension of the scapular spine, forming the roof of the subacromial space. Its morphology (Type I-III, flat, curved, hooked) influences subacromial impingement.
- Clavicle: The superior border of the shoulder girdle. The lateral aspect articulates with the acromion to form the AC joint.
- Coracoid Process: A hook-like bony projection from the superior border of the scapula, inferomedial to the glenoid. It serves as an attachment point for numerous muscles and ligaments, including the short head of the biceps, coracobrachialis, pectoralis minor, coracoacromial ligament, and coracoclavicular ligaments.
- Greater Tuberosity: The most lateral prominence of the proximal humerus, serving as the insertion site for the supraspinatus, infraspinatus, and teres minor tendons.
Muscular Anatomy
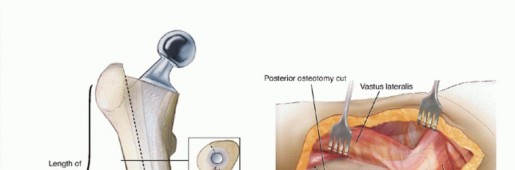
- Deltoid: A large, powerful muscle forming the rounded contour of the shoulder. It comprises anterior, middle, and posterior fibers. The anterolateral approach typically utilizes a split between the anterior and middle fibers or within the anterior fibers, which facilitates access to the subacromial space and rotator cuff. Care must be taken to limit the distal extent of the deltoid split to avoid injury to the axillary nerve.
- Rotator Cuff: Composed of the supraspinatus, infraspinatus, teres minor, and subscapularis muscles. The supraspinatus tendon lies directly beneath the acromion and coracoacromial ligament, making it the primary target for repair via this approach.
- Biceps Brachii (Long Head): Its tendon originates from the supraglenoid tubercle, courses through the bicipital groove, and can be easily accessed anteriorly.
Ligamentous Structures
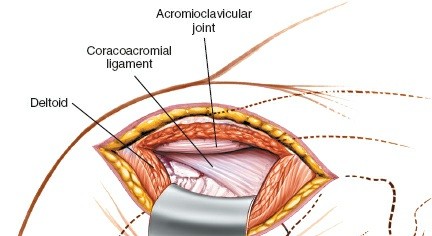
- Coracoacromial Ligament (CAL): Spans between the coracoid process and the acromion. It forms the anterior-inferior boundary of the subacromial space. Resection of this ligament is a key component of subacromial decompression.
- Acromioclavicular Ligaments: Provide primary stability to the AC joint capsule (superior, inferior, anterior, posterior).
- Coracoclavicular Ligaments (Conoid and Trapezoid): Critical for vertical stability of the AC joint, connecting the coracoid process to the inferior aspect of the clavicle. They are spared or protected during distal clavicle excision unless AC joint reconstruction is simultaneously performed.
Neurovascular Structures
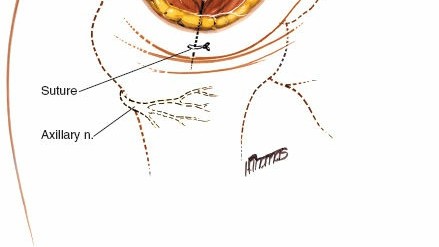
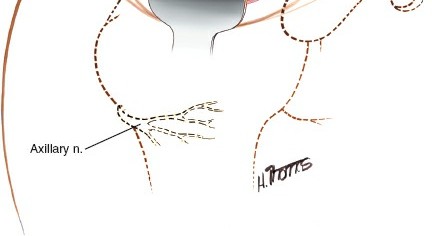
- Axillary Nerve: Courses inferior to the glenohumeral joint and wraps around the surgical neck of the humerus, innervating the deltoid and teres minor muscles. It is highly vulnerable during deltoid splitting, typically found 5-7 cm distal to the lateral acromial edge. Deltoid splits should not extend beyond 5 cm distally from the acromion to mitigate this risk.
- Cephalic Vein: Located in the deltopectoral groove. While the anterolateral approach is primarily deltoid-splitting rather than deltopectoral, superficial branches may be encountered and require ligation or careful retraction.
- Suprascapular Nerve: Deeply situated, it can be at risk during aggressive posterior retraction or capsular release, particularly where it passes through the suprascapular notch.
Biomechanics
The anterolateral approach primarily targets structures involved in the biomechanics of shoulder elevation and stability. Pathologies leading to subacromial impingement often involve the CAL, acromial morphology, and rotator cuff integrity. Resection of the CAL and creation of a flat acromial undersurface aim to increase the subacromial clearance, thereby reducing mechanical impingement on the supraspinatus tendon. Rotator cuff integrity is fundamental for glenohumeral stability and efficient force transmission during arm elevation. AC joint stability relies on the combined action of the AC and coracoclavicular ligaments; disruption leads to altered kinematics and often pain.
Indications & Contraindications
The anterolateral approach is indicated for a range of conditions affecting the subacromial space and AC joint.
Indications
- Anterior Subacromial Decompression: For chronic subacromial impingement syndrome refractory to conservative management, particularly with Type II or Type III acromial morphology, osteophytes, or hypertrophic CAL. This involves acromioplasty and CAL release.
- Rotator Cuff Repair: Especially for isolated supraspinatus tears, small to medium-sized full-thickness tears, or as part of a larger repair. The open approach allows direct visualization and robust suture placement.
- Long Head of Biceps Tendon Pathology: Indicated for biceps tenodesis or tenotomy in cases of instability, tendinitis, or partial tears, often concomitant with rotator cuff repair.
-
Acromioclavicular Joint Pathology:
- Distal Clavicle Excision (Mumford Procedure): For symptomatic AC joint osteoarthritis or osteolysis refractory to conservative management.
- AC Joint Reconstruction/Stabilization: For chronic, symptomatic AC joint separations (e.g., Rockwood Type III, IV, V) requiring restoration of stability, often combined with augmentation techniques.
- Calcific Tendinopathy: Excision of large, symptomatic calcific deposits within the rotator cuff.
- Greater Tuberosity Fracture Fixation: While often managed arthroscopically or with other approaches, the anterolateral approach can provide direct access for reduction and fixation of certain greater tuberosity fractures.
Contraindications
- Active Infection: Absolute contraindication due to risk of spreading infection.
- Severe Systemic Illness: Uncontrolled comorbidities precluding safe anesthesia or surgical stress.
- Extensive Posterior Pathology: This approach does not provide adequate visualization for primary posterior glenohumeral or rotator cuff pathology.
- Significant Deltoid Compromise: Prior extensive deltoid detachment, denervation, or severe scarring may make a deltoid-splitting approach problematic.
- Unrealistic Patient Expectations: Poor understanding of surgical limitations, recovery, or potential complications.
- Unwillingness to Participate in Post-Operative Rehabilitation: Crucial for successful outcomes.
Table: Operative vs. Non-Operative Indications for Anterolateral Approach Target Pathologies
| Pathology | Non-Operative Indications | Operative Indications (Anterolateral Approach) |
|---|---|---|
| Subacromial Impingement | Initial acute/subacute symptoms, mild-moderate pain, good ROM, failed conservative measures (rest, NSAIDs, PT, injections). | Chronic symptoms >3-6 months, failed conservative management, specific anatomical impingement (Type II/III acromion, osteophytes), rotator cuff partial tear. |
| Rotator Cuff Tear | Small, asymptomatic partial tears; elderly, low-demand patients; good function despite tear; failed PT. | Symptomatic full-thickness tears, progressive tears, young/active patients, significant functional deficit, failed conservative treatment. |
| Long Head Biceps Tendinopathy | Mild pain, good function, failed conservative measures (rest, NSAIDs, PT, injections). | Persistent pain, mechanical symptoms (popping), instability, significant tendinosis/partial tear, often concomitant with rotator cuff pathology. |
| AC Joint Osteoarthritis/Osteolysis | Mild pain, activity modification, NSAIDs, local injections, early degenerative changes. | Chronic, severe pain refractory to conservative care, functional limitations, significant osteophytes, distal clavicle osteolysis. |
| AC Joint Separation | Rockwood Type I & II (stable, minimal displacement). | Rockwood Type III (symptomatic, failure of conservative management), Type IV, V, VI (unstable, significant displacement requiring reconstruction). |
| Calcific Tendinopathy | Mild symptoms, small deposits, failed NSAIDs/PT/ESWT. | Large, persistent, severely painful deposits refractory to all non-operative measures. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing surgical exposure, minimizing complications, and ensuring a safe procedure.
Pre-Operative Planning
- Clinical Assessment: A thorough history and physical examination are essential to confirm the diagnosis, assess neurovascular status, and identify any comorbidities.
-
Imaging Review:
- Radiographs: AP, Y-scapular, and axillary views are standard to evaluate bony anatomy, acromial morphology, AC joint arthritis, and calcifications.
- MRI: The gold standard for soft tissue evaluation, providing detailed information on rotator cuff integrity, biceps pathology, and labral tears.
- CT Scan: Useful for complex bony pathologies, fracture assessment, or pre-operative templating for AC joint reconstruction.
- Anesthesia Consultation: Discussion regarding general anesthesia versus regional nerve block (e.g., interscalene block) for post-operative pain management.
- Informed Consent: Detailed discussion with the patient regarding the procedure, expected outcomes, potential risks, and alternatives.
- Equipment Preparation: Ensure all necessary instruments, implants (suture anchors, fixation devices for AC joint reconstruction), and retractors are available and sterile.
- Antibiotic Prophylaxis: Administer pre-operative intravenous antibiotics as per institutional protocol (e.g., Cefazolin).
Patient Positioning
The anterolateral approach is typically performed with the patient in the beach chair position . This position offers excellent visualization, allows free manipulation of the arm, and is generally well-tolerated.
- Operating Table Setup: The patient is placed supine on the operating table. The table is then flexed at the hips and knees to achieve a semi-sitting position.
- Head and Neck: The head is secured in a well-padded headrest, maintaining neutral alignment to prevent cervical strain or brachial plexus stretch. Ensure adequate padding for the occiput.
-
Torso:
A
sandbag or bolster
is placed beneath the ipsilateral scapula and medial border to elevate the shoulder and push the affected side forward. This protracts the scapula, improving anterior exposure and making the superior shoulder easier to access.

Caption: Patient positioned in the beach chair position, with a sandbag placed under the ipsilateral scapula to protract the shoulder. - Legs: Legs are secured in a well-padded leg holder, with careful attention to pressure points, particularly the heels and calves, to prevent nerve compression or skin breakdown.
- Arm Preparation: The entire limb, from the hand to the shoulder, is prepped and draped freely. This allows the surgical assistant to move the arm throughout the range of motion during the procedure, facilitating visualization of various structures and tensioning of the rotator cuff. A sterile stockinette or impervious drape is applied to the arm.
- Padding: All pressure points (e.g., elbows, heels, sacrum, occiput, ulnar nerves) are meticulously padded to prevent iatrogenic injury.
- Tourniquet: A tourniquet is typically not required for shoulder surgery but should be readily available on the upper arm for emergent use if needed.
Detailed Surgical Approach / Technique
The anterolateral approach provides excellent exposure of the superior aspect of the glenohumeral joint, subacromial space, and AC joint.
Landmarks and Incision
-
Palpation: Key anatomical landmarks are identified and marked on the skin:
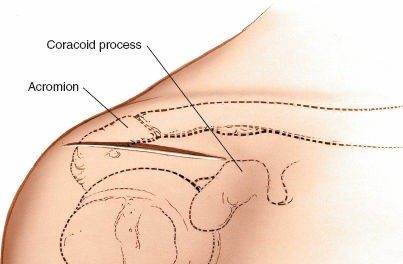
- Acromion: The lateral tip and anterior border.
- Clavicle: The lateral half.
- Acromioclavicular (AC) Joint: The palpable depression between the lateral clavicle and acromion.
- Coracoid Process: Palpated inferomedial to the humeral head, deep to the pectoralis major.
- Greater Tuberosity: Palpable with internal and external rotation of the arm.
-
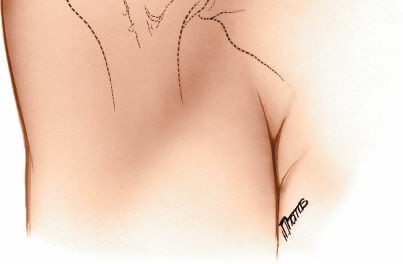
Incision: The skin incision is typically 5-8 cm long, centered over the anterolateral aspect of the acromion.
- For subacromial decompression and rotator cuff repair, a curved incision starting posterior to the posterolateral corner of the acromion, following the Langer's lines over the acromion, and curving anteriorly and slightly distally along the deltoid fibers, provides excellent exposure.
-
For isolated AC joint procedures (e.g., distal clavicle excision), a more transverse or slightly oblique incision directly over the AC joint may be preferred.

Caption: Skin incision marked. The incision is typically curved, extending from the posterolateral acromion, over the acromion, and then anteriorly along the deltoid fibers.
Dissection (Step-by-Step)
-
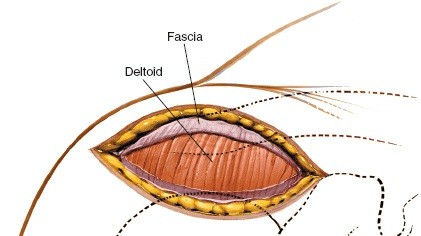
Skin and Subcutaneous Tissue: The incision is carried through the skin and subcutaneous tissue. Hemostasis is achieved. The subcutaneous fat is dissected to expose the underlying deltoid fascia. Identify and ligate or carefully retract any superficial veins, including branches of the cephalic vein.
-
Deltoid Split:
- The deltoid fascia is incised longitudinally, typically in line with the anterior deltoid fibers or in the interval between the anterior and middle deltoid, commencing at the acromion.
-
Using blunt dissection (e.g., with scissors or a finger), the deltoid fibers are carefully separated. The deltoid split should extend distally no more than
5 cm
from the lateral acromial edge to avoid iatrogenic injury to the axillary nerve, which wraps around the surgical neck of the humerus approximately 5-7 cm distal to the acromial edge.
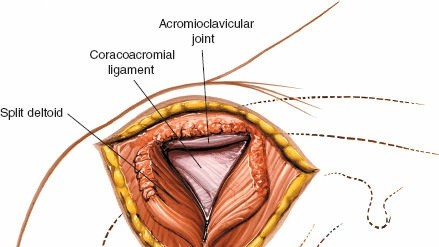
Caption: The deltoid fascia has been incised, and the deltoid fibers are being carefully split using blunt dissection. Note the limited distal extension to protect the axillary nerve.
-
Subacromial Space Exposure:
- Self-retaining retractors are placed to gently hold open the deltoid split, exposing the subacromial bursa.
-
The
subacromial bursa
is often inflamed and hypertrophic in cases of impingement or rotator cuff tears. It is systematically excised using electrocautery and dissecting scissors to improve visualization of the underlying rotator cuff and the coracoacromial ligament.
Caption: The subacromial bursa is being excised, revealing the underlying rotator cuff and coracoacromial ligament.
-
Coracoacromial Ligament (CAL) Release and Acromioplasty:
- The CAL is identified running from the coracoid process anteriorly to the undersurface of the acromion. In cases of impingement, the CAL is often thickened.
- The anterior aspect of the CAL is released from its acromial attachment.
-
An anterior
acromioplasty
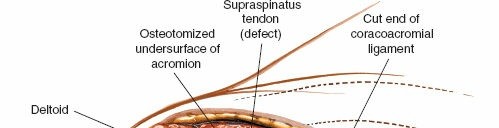
is performed to flatten the undersurface of the acromion and increase the subacromial space. This is typically achieved using an osteotome or a burr. The anterior 1-1.5 cm of the acromion is resected, paying attention to remove any spurs or hook formations. Care must be taken to preserve the acromial origin of the deltoid as much as possible, especially the lateral portion, to prevent deltoid insufficiency.
Caption: The coracoacromial ligament has been released, and an acromioplasty is being performed using a burr to resect the anterior and inferior aspects of the acromion.
-
Rotator Cuff Exposure and Repair:
- With the bursa excised and acromioplasty complete, the supraspinatus tendon becomes clearly visible, lying directly superior to the humeral head. The arm can be externally and internally rotated to bring the different parts of the rotator cuff (infraspinatus, subscapularis) into view.
- The extent of the rotator cuff tear is assessed. The tendon edges are debrided to healthy tissue.
- The footprint on the greater tuberosity is prepared by decortication to promote healing.
-
Repair:
Suture anchors (biocomposite or metallic) are placed into the bone of the greater tuberosity. The torn tendon is then mobilized and brought back to its anatomical insertion using various suture configurations (e.g., simple sutures, mattress sutures, suture bridges). The repair is tensioned adequately, and knot security is ensured.
Caption: The supraspinatus tendon is exposed following subacromial decompression. A full-thickness tear is visible, exposing the humeral head.

Caption: Rotator cuff repair nearing completion. Suture anchors have been placed, and the tendon is secured to its footprint on the greater tuberosity.
-
Acromioclavicular (AC) Joint Management:
- If distal clavicle excision (Mumford procedure) is indicated for AC joint arthritis, the periosteum over the distal clavicle and acromion is incised. A portion (typically 8-10 mm) of the lateral clavicle is resected using an oscillating saw or osteotome. Care is taken to protect the underlying coracoclavicular ligaments and soft tissues.
-
For
AC joint reconstruction
, the AC joint capsule and surrounding ligaments are typically repaired or reconstructed using various techniques (e.g., semitendinosus autograft, synthetic ligament augmentation, hook plate) depending on the specific instability pattern.
Caption: Distal clavicle excision (Mumford procedure) in progress. A portion of the lateral clavicle is being resected to alleviate AC joint arthritis.
Caption: AC joint reconstruction demonstrated with a hook plate, bridging the clavicle and acromion to stabilize a severe AC joint separation.
-
Long Head of Biceps Tendon Management:
- The long head of the biceps tendon can be identified in the bicipital groove anteriorly.
- If indicated, a biceps tenodesis can be performed. This involves releasing the tendon from its superior labral origin and reattaching it to the humerus, either within the bicipital groove or more proximally/distally, using screws or suture anchors.
-
Alternatively, a
biceps tenotomy
(simple release) may be performed, especially in older, less active patients.

Caption: The long head of the biceps tendon is visible in the bicipital groove. It can be addressed via tenodesis or tenotomy as needed.
Closure
- Hemostasis: Ensure meticulous hemostasis to prevent post-operative hematoma.
- Deltoid Repair: The deltoid split is meticulously repaired using strong, non-absorbable sutures (e.g., #2 or #0 Ethibond). This is critical to restore deltoid function and prevent deltoid dehiscence, which can lead to significant functional impairment. The repair should reapproximate the fibers without excessive tension.
-
Subcutaneous and Skin Closure:
The subcutaneous layer is closed with absorbable sutures. The skin is closed with staples or intradermal sutures, depending on surgeon preference.
Caption: The deltoid muscle has been meticulously repaired, and the subcutaneous tissue is being closed before skin closure.
Complications & Management
While the anterolateral approach is generally safe, understanding potential complications and their management is crucial.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.) | Etiology / Contributing Factors | Management & Salvage Strategies |
|---|---|---|---|
| Axillary Nerve Injury | Rare (<1-2%) | Excessive distal deltoid split (>5cm from acromion), aggressive retraction, direct trauma. | Observation: Most neurapraxias recover spontaneously within 3-6 months. Nerve Study (EMG/NCS): If no recovery. Neurolysis/Repair: For severe injuries (transection) if indicated and feasible. Tendon Transfer: (e.g., latissimus dorsi to deltoid) for persistent, debilitating deltoid paralysis. |
| Deltoid Detachment / Dehiscence | 2-5% | Inadequate deltoid repair, excessive tension, avulsion from acromial attachment, poor tissue quality. | Surgical Repair: Meticulous revision repair with strong, non-absorbable sutures to bone (if possible) or remnant deltoid. Allograft/Autograft Patch: For large defects. Activity Restriction: Prolonged immobilization and protected rehabilitation. |
| Infection | 1-2% | Surgical site contamination, compromised host immunity, prolonged surgery. | Superficial: Oral/IV antibiotics. Deep: Surgical debridement, washout, IV antibiotics. Removal of hardware if infected. Flap Coverage: For persistent, complex wound issues. |
| Stiffness / Adhesive Capsulitis | 5-10% | Inadequate early mobilization, excessive inflammation, pre-existing stiffness risk factors (diabetes, thyroid disease). | Aggressive Physical Therapy: Home exercise program, supervised PT. NSAIDs/Steroid Injections: To reduce inflammation. Manipulation Under Anesthesia (MUA): For severe cases. Arthroscopic Capsular Release: Surgical option for recalcitrant stiffness. |
| Rotator Cuff Re-tear (after repair) | 5-30% (variable) | Poor tendon quality, large/massive tears, patient non-compliance, technical failure, premature loading. | Observation: Small, asymptomatic re-tears. Physical Therapy: Focus on strength and function. Revision Repair: For symptomatic, reparable tears in appropriate candidates. Tendon Transfer / Superior Capsular Reconstruction: For irreparable tears. |
| Persistent Pain | Up to 10-15% | Incomplete decompression, residual impingement, nerve irritation, underlying glenohumeral arthritis, complex regional pain syndrome (CRPS). | Thorough Diagnostic Workup: Imaging (MRI/CT), diagnostic injections. Targeted Injections: Subacromial, AC joint, nerve blocks. Pain Management Referral: For chronic pain. Revision Surgery: For identifiable and addressable pathology. |
| AC Joint Instability (after DCR) | 5-10% | Inadequate resection leading to bony impingement, failure of associated stabilization (if performed). | Revision Distal Clavicle Excision: If inadequate bone resection. AC Joint Reconstruction: If persistent instability and pain. |
| Hematoma / Seroma | 1-3% | Inadequate hemostasis during surgery. | Observation: For small, non-expanding collections. Aspiration: For larger, symptomatic collections. Surgical Drainage: For large, tense hematomas or if infection is suspected. |
| Cosmetic Issues | Variable | Individual healing characteristics, tension on wound. | Topical Scar Treatments: Silicone gel/sheets. Steroid Injections: For hypertrophic scars/keloids. Surgical Revision: For severe, symptomatic cosmetic deformities. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as crucial as the surgical technique itself for achieving optimal functional outcomes. Protocols vary based on the specific procedure performed, tear size, tissue quality, and surgeon preference. The general principle is a progressive, staged approach that balances protection of the repair with gradual restoration of motion and strength.
General Principles:
- Individualized: Tailored to patient's age, activity level, tissue quality, and goals.
- Progressive: Gradually increases stress on healing tissues.
- Pain-Controlled: Adequate pain management is essential for participation.
- Supervised: Guided by a physical therapist working closely with the surgeon.
Phase I: Protection & Passive Range of Motion (0-6 weeks)
- Goal: Protect the surgical repair, minimize pain and swelling, allow initial soft tissue healing.
-
Immobilization:
- Sling: Worn continuously, except for exercises and hygiene. Duration varies (e.g., 4-6 weeks for rotator cuff repair, 2-4 weeks for decompression/DCR).
- Sleeping: Recommended to sleep in the sling, often in a semi-recumbent position.
-
Exercises (Daily):
- Pendulum Exercises: Gentle, gravity-assisted swings of the arm to promote circulation and prevent stiffness without active muscle contraction.
-
Passive Range of Motion (PROM):
Performed by the therapist or with the contralateral hand.
- Forward Flexion: To 90-120 degrees, depending on repair security.
- External Rotation: Limited to 0-30 degrees, especially if subscapularis was repaired.
- Internal Rotation: Hand-to-back exercises.
- Scapular Mobilization: Gentle, non-painful movements to maintain scapulothoracic rhythm.
- Elbow, Wrist, Hand AROM: To prevent stiffness in unaffected joints.
-
Precautions:
- No active lifting, pushing, or pulling.
- No active shoulder movements.
- Avoid weight-bearing through the affected arm.
Phase II: Controlled Active-Assisted & Active Range of Motion (6-12 weeks)
- Goal: Gradually restore full, non-painful range of motion; initiate gentle strengthening.
- Sling Discontinuation: Usually weaned off during this phase, as tolerated.
-
Exercises:
- Active-Assisted Range of Motion (AAROM): Progress from PROM to AAROM using pulleys, sticks, or the unaffected arm.
- Active Range of Motion (AROM): Gradually initiate pain-free active shoulder movements.
- Gentle Isometric Strengthening: Submaximal contractions of the rotator cuff and deltoid, held for short durations.
- Scapular Stabilization Exercises: Focus on strengthening periscapular muscles (rhomboids, serratus anterior, trapezius).
-
Precautions:
- Avoid painful movements.
- No heavy lifting or sudden movements.
- Continue to avoid resisted internal/external rotation if specific repairs warrant.
Phase III: Progressive Strengthening & Endurance (12-24 weeks)
- Goal: Restore muscle strength, power, and endurance; prepare for functional activities.
-
Exercises:
-
Progressive Resistive Exercises (PREs):
Using elastic bands, light weights, or bodyweight.
- Rotator cuff strengthening (internal/external rotation, abduction).
- Deltoid strengthening.
- Advanced scapular stabilization.
- Core and Postural Strengthening: To support overall shoulder mechanics.
- Endurance Training: Repetitive low-resistance exercises.
-
Progressive Resistive Exercises (PREs):
Using elastic bands, light weights, or bodyweight.
- Functional Activities: Gradual return to light, non-strenuous daily activities.
-
Precautions:
- Avoid pain-producing activities.
- Progress weight and resistance cautiously.
Phase IV: Return to Activity / Sport (24+ weeks)
- Goal: Achieve full functional return, including sport-specific or work-related activities.
-
Exercises:
- Sport-Specific Training: Incorporate drills simulating sport movements (throwing, overhead activities).
- Plyometric Exercises: For dynamic strength and power, if appropriate for patient goals.
- Advanced Proprioception and Neuromuscular Control: To enhance stability and coordination.
- Return to Activity: Gradual and progressive return to full activities or sports, guided by functional testing and surgeon clearance. This phase can extend beyond 6 months, especially for overhead athletes or demanding occupations.
Summary of Key Literature / Guidelines
The anterolateral approach has been a cornerstone in shoulder surgery for decades, and its efficacy is well-supported in the literature, particularly for subacromial decompression and rotator cuff repair.
-
Subacromial Decompression (SAD):
- The role of SAD, particularly acromioplasty and coracoacromial ligament release, has been extensively studied. Early literature (Neer, 1972) established its effectiveness for chronic impingement. While arthroscopic SAD has largely superseded open SAD for isolated impingement, the principles of creating subacromial clearance remain.
- Recent randomized controlled trials (e.g., FINN-ISE, CSST) have questioned the added benefit of acromioplasty over bursectomy and debridement alone for some forms of impingement, particularly without a rotator cuff tear. However, for clear morphological impingement (Type II/III acromion, osteophytes), acromioplasty via an open or arthroscopic approach remains a standard.
-
Rotator Cuff Repair:
- Open rotator cuff repair using the anterolateral approach has demonstrated excellent long-term outcomes, particularly for small to medium-sized tears. Meta-analyses comparing open, mini-open (which often uses an anterolateral split), and arthroscopic techniques have generally shown comparable functional outcomes and re-tear rates, though arthroscopic techniques may offer less post-operative pain and improved cosmesis in the short term.
- Studies on the biomechanics of suture anchor fixation and various repair constructs (single-row, double-row, suture bridge) have informed modern repair strategies aimed at maximizing footprint coverage and initial strength.
-
AC Joint Pathology:
- Distal Clavicle Excision (Mumford Procedure): Both open (via anterolateral approach) and arthroscopic techniques have proven effective for symptomatic AC joint osteoarthritis or osteolysis. Literature supports both as viable options, with comparable pain relief and functional improvement.
- AC Joint Reconstruction: For chronic, unstable AC joint separations, various open techniques, often utilizing the anterolateral approach, have been described. These include autograft or allograft reconstruction of the coracoclavicular ligaments, augmented with internal fixation (e.g., hook plate, suture button constructs). Outcomes are generally favorable, though complications like hardware irritation or loss of reduction can occur.
-
Biceps Tenodesis:
- The anterolateral approach allows for easy access to the long head of the biceps for tenodesis (suprapectoral or subpectoral) or tenotomy. Literature indicates that tenodesis generally provides superior cosmetic results (less "Popeye" deformity) and potentially better endurance compared to tenotomy, particularly in younger, active patients.
-
Axillary Nerve Safety:
- Anatomical studies consistently emphasize the critical importance of limiting the deltoid split to 5 cm distally from the acromion to minimize the risk of axillary nerve injury. The nerve typically crosses the deep surface of the deltoid 5-7 cm from the lateral acromial edge. Electrophysiological monitoring can be considered in revision cases or when extensive distal exposure is anticipated.
In conclusion, the precision anterolateral approach remains a foundational technique in orthopedic shoulder surgery. Its well-defined anatomical landmarks, versatile exposure, and proven track record make it an invaluable tool for managing a wide array of subacromial and AC joint pathologies. While arthroscopic advancements continue to evolve, the open anterolateral approach ensures direct, robust, and reproducible surgical solutions when indicated.
Clinical & Radiographic Imaging
You Might Also Like