Sacroiliac Joint Anterior Approach: Comprehensive Review of Anatomy, Biomechanics & Surgical Rationale
Key Takeaway
The anterior approach to the sacroiliac (SI) joint offers superior access and control, particularly for specific pelvic ring injuries. It provides direct visualization for precise anatomical reduction and plate application, crucial for unstable fracture patterns like APC Type II/III, LC Type II/III, or vertical shear injuries. This enhances stability and improves patient outcomes.
Sacroiliac Joint Anterior Approach: Superior Access & Control
Introduction & Epidemiology
The sacroiliac (SI) joint represents a critical component of the pelvic ring, facilitating load transfer between the axial skeleton and the lower extremities. Its inherent stability is derived from the complex interplay of its articular surfaces and a robust ligamentous complex. Dysfunction or injury to the SI joint can significantly compromise pelvic stability and profoundly impact patient mobility and quality of life.
Epidemiologically, SI joint pathology ranges from insidious degenerative changes to acute traumatic disruptions. Traumatic injuries, particularly high-energy pelvic ring fractures, frequently involve the SI joint, representing a significant challenge in orthopedic trauma. These injuries can manifest as pure ligamentous disruptions, sacral fractures extending into the joint, or iliac wing fractures that violate the joint line. The integrity of the posterior pelvic ring, often maintained by the SI joint, is paramount for overall pelvic stability, and its disruption necessitates accurate anatomical reduction and stable fixation to prevent long-term sequelae such as chronic pain, gait disturbance, and functional impairment.
While posterior approaches have traditionally been favored for addressing SI joint pathology due to the joint's posterior anatomical location, the anterior approach has emerged as a compelling alternative, and in many instances, a superior option for specific indications. This approach offers direct visualization of the anterior joint capsule and the inner wall of the ilium, providing distinct advantages for certain fracture patterns and facilitating precise plate application, thereby offering enhanced access and control over reduction and fixation.
Surgical Anatomy & Biomechanics
Surgical Anatomy
The sacroiliac joint is a diarthrodial joint anteriorly and a syndesmosis posteriorly. Its articular surfaces, located on the ilium and sacrum, are auricle-shaped and lined with hyaline cartilage on the sacral side and fibrocartilage on the iliac side. These surfaces exhibit significant congruence variability among individuals.
Key anatomical considerations for the anterior approach include:
*
Ligamentous Structures:
*
Anterior Sacroiliac Ligaments:
Relatively thin and weak, contributing minimally to overall joint stability compared to their posterior counterparts. These ligaments are typically incised or elevated during the anterior approach.
*
Interosseous Sacroiliac Ligaments:
The strongest ligaments of the SI joint, situated immediately superior and posterior to the articular surfaces. These are not directly exposed via the anterior approach but contribute significantly to the biomechanical stability that fixation must restore.
*
Posterior Sacroiliac Ligaments:
Comprise the short and long posterior SI ligaments, forming a formidable posterior tension band. These are also not directly accessed anteriorly.
*
Bony Anatomy:
The flat, anterior aspect of the SI joint directly beneath the iliac fossa allows for straightforward access. In contrast, the posterior aspect is deeply situated and overhung by the posterior iliac crest and robust musculature. The inner wall of the ilium (iliac ala) is critical, as it allows for placement of fixation constructs that can buttress or compress associated iliac fractures extending into the SI joint. The sacral ala and body are the target for screw purchase.
*
Neurovascular Structures:
*
Iliac Vessels:
The common and external iliac arteries and veins lie medially to the iliac fossa and must be carefully identified, mobilized, and protected throughout the exposure. The ureter typically crosses anterior to the common iliac artery.
*
Lumbar Plexus & Nerves:
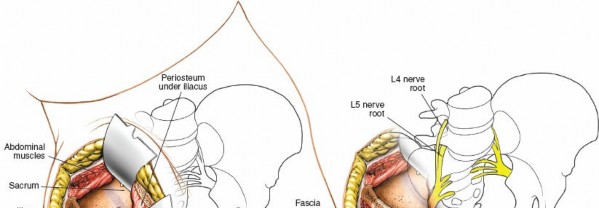
The femoral nerve (L2-L4) lies deep to the iliacus muscle. The lateral femoral cutaneous nerve emerges from the lateral border of the psoas muscle and crosses the iliacus muscle obliquely towards the ASIS, requiring protection during the initial incision and muscle dissection. The L5 nerve root (lumbosacral trunk) passes anterior to the sacral ala and can be vulnerable, particularly during sacral screw placement. Careful dissection and anatomical awareness are paramount.
*
Muscles:
The iliacus muscle lines the iliac fossa. Medial retraction of the abdominal contents (peritoneum, bowel) and careful subperiosteal elevation of the iliacus muscle exposes the inner table of the ilium and the anterior aspect of the SI joint.
Biomechanics
The SI joint is a unique structure designed for both stability and limited shock absorption. Its primary biomechanical function is to transfer loads between the spine and the lower limbs while maintaining the integrity of the pelvic ring.
*
Form Closure:
Refers to the stability provided by the anatomical configuration of the joint, including its undulating surfaces, the wedge shape of the sacrum, and the friction coefficient between the articular cartilages.
*
Force Closure:
Relates to the dynamic stability provided by the muscles and ligaments acting across the joint, generating compressive forces that enhance its resistance to displacement. The anterior sacroiliac ligaments provide minimal force closure compared to the robust posterior ligamentous complex.
*
Injury Patterns:
In traumatic pelvic ring disruptions, the anterior approach is particularly valuable for unstable injuries classified as anteroposterior compression (APC) Type II or III (Young-Burgess classification), lateral compression (LC) Type II or III, or vertical shear (VS). These injuries often involve significant anterior SI joint capsule disruption or anterior sacral fracture components, which are directly accessible for reduction and stabilization via this approach.
Indications & Contraindications
The anterior approach to the sacroiliac joint offers specific advantages for certain pathologies. The decision to utilize this approach is predicated on a thorough understanding of the injury pattern, patient physiology, and potential complications.
Indications
The primary indications for the anterior approach to the SI joint are predominantly traumatic pelvic ring disruptions requiring direct visualization and robust fixation of the anterior SI joint or associated iliac fractures.
-
Traumatic Pelvic Ring Disruptions:
- Anteroposterior Compression (APC) Type II and III Injuries: In these unstable patterns, significant anterior SI joint capsular disruption or avulsion of the anterior sacroiliac ligaments occurs. The anterior approach allows direct repair or plating.
- Lateral Compression (LC) Type II and III Injuries with Anterior SI Joint Disruption: While LC injuries typically involve posterior instability, severe rotational components can lead to anterior disruption, justifying an anterior approach.
- Vertical Shear (VS) Injuries: Often involve complete disruption of both anterior and posterior ligamentous complexes. Anterior plating can be a crucial component of bimodal fixation.
- Sacral Fractures: Especially those with an oblique or transverse component through the sacral ala that require direct compression or buttressing anteriorly.
- Iliac Wing Fractures (Ala Fractures) extending into the SI Joint: The anterior approach provides unparalleled access to the inner wall of the ilium, allowing for direct reduction and fixation of these associated fractures, which is difficult or impossible via posterior approaches.
- Sacroiliac Fracture-Dislocations: Where the iliac fracture line runs through the SI joint.
- Chronic Sacroiliac Joint Instability (for Arthrodesis): In select cases of chronic, severe SI joint pain and instability refractory to non-operative treatment, an anterior approach can be used for arthrodesis. This typically involves joint denudation and bone graft placement, followed by plate fixation.
- Tumor Resection or Biopsy: When the anterior aspect of the sacrum or ilium requires access.
Contraindications
Absolute and relative contraindications must be carefully considered:
-
Absolute Contraindications:
- Active Local Infection: Presence of osteomyelitis or soft tissue infection in the surgical field.
- Critical Medical Comorbidities: Patients unstable for prolonged general anesthesia or with severe cardiovascular/pulmonary compromise.
- Unstable Hemodynamics: Requiring immediate damage control laparotomy, which might preclude a concurrent or immediate elective pelvic fixation.
-
Relative Contraindications:
- Severe Obesity: Can make exposure and retraction extremely challenging, increasing operative time and complication risk.
- Previous Abdominal Surgeries: Particularly those resulting in significant adhesions, which increase the risk of bowel injury.
- Lack of Anterior Instability: If the primary instability is purely posterior (e.g., APC I, LC I, or isolated posterior ligamentous injury), a posterior approach may be more appropriate and less invasive.
- Severe Osteoporosis: May compromise hardware purchase, particularly in the sacrum, leading to fixation failure.
- Extensive Soft Tissue Injury/Degloving: In the region of the anterior incision (e.g., Morel-Lavallée lesion), increasing wound complication risk.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management (Anterior Approach) | Non-Operative Management |
|---|---|---|
| Pelvic Ring Injury | - APC Type II (significant gapping) | - APC Type I (stable, symphyseal widening < 2.5 cm) |
| - APC Type III (complete disruption, open book) | - LC Type I (stable, impaction, minimal displacement) | |
| - LC Type II/III (with anterior SI disruption) | - Isolated avulsion fractures of iliac spine | |
| - Vertical Shear (anterior fixation component) | ||
| Sacral/Iliac Fracture | - Displaced sacral ala fractures involving SI joint | - Non-displaced sacral ala fractures |
| - Displaced iliac ala fractures extending to SI joint | - Stable iliac wing fractures without SI involvement | |
| Chronic SI Joint Pain | - Refractory instability (for fusion, after failed conservative care) | - All initial presentations of SI joint pain |
| - SI joint dysfunction (subluxation, inflammation, sprain) | ||
| Other | - Tumor resection/biopsy requiring anterior access | - Minor ligamentous sprains, muscle strains |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are critical for a safe and effective anterior approach to the SI joint.
Pre-Operative Planning
-
Imaging Review:
- Computed Tomography (CT) Scan: Essential. Obtain fine-cut axial, coronal, and sagittal reconstructions. 3D reconstructions are invaluable for understanding complex fracture morphology, displacement, and joint violation. Identify the exact nature of the SI joint disruption (ligamentous, fracture through sacrum/ilium).
- Radiographs: Standard AP, inlet, and outlet views of the pelvis. These provide initial assessment and dynamic information, but CT is required for definitive characterization.
- Magnetic Resonance Imaging (MRI): May be considered for assessing soft tissue injury, nerve involvement, or chronic SI joint pathology if not already evident on CT.
- Patient Assessment: Evaluate comorbidities, obtain thorough medical clearance, and optimize nutritional status. Assess for potential contraindications.
-
Implants & Equipment:
- Plate Systems: Reconstruction plates (e.g., 3.5mm), specialized pelvic fixation plates, or SI joint specific plates. Ensure adequate length and number of screw holes.
- Screws: Cortical screws of appropriate diameter and length.
- Reduction Instruments: Various pointed reduction clamps, pelvic reduction clamps, Hohmann retractors, broad malleable retractors.
- Fluoroscopy: C-arm with high-quality imaging capabilities is indispensable for intraoperative confirmation of reduction and hardware placement.
- Vascular Instruments: In case of major vessel injury.
- Team Briefing: Discuss the surgical plan, potential challenges, and contingency plans with the entire surgical team (anesthesia, nursing, residents, fellows).
Patient Positioning
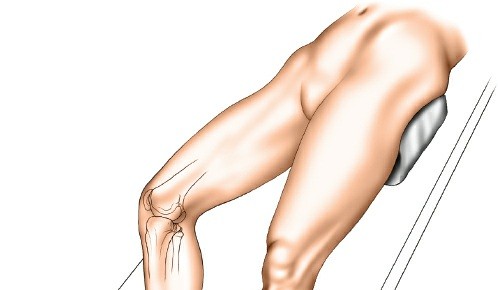
The patient is positioned supine on a radiolucent operating table.
*
Supine Position:
Allows for easy access to the anterior abdomen and pelvis.
*
Ipsilateral Buttock Support:
A large sandbag or bump is placed under the ipsilateral buttock (the side to be operated on). This maneuver effectively elevates the ipsilateral iliac crest and rotates the hemipelvis slightly, bringing the anterior aspect of the SI joint into a more accessible plane for the surgeon.
*
Contralateral Support:
The contralateral iliac wing is supported with a dedicated support attached to the operating table. This helps stabilize the pelvis during table manipulation.
*
Table Tilt:
The operating table is then tilted approximately 20 degrees away from the surgeon (towards the contralateral side). This gravity-assists in retracting the mobile contents of the pelvis (bowel, peritoneum) away from the surgical field, minimizing the need for aggressive manual retraction and reducing the risk of iatrogenic injury.
*
Fluoroscopy Access:
Ensure the C-arm can obtain unobstructed AP, inlet, and outlet views of the pelvis throughout the procedure. This often requires placing the C-arm from the contralateral side.
*
Foley Catheter:
Insertion of a Foley catheter is mandatory to decompress the bladder and protect it from injury during dissection and retraction.
*
Prep and Drape:
The surgical field is prepped widely, typically from the costal margin to the mid-thigh, including bilateral iliac crests, to allow for potential extension of the incision or bone graft harvest if needed. The entire abdomen should be prepped to allow for extension to a laparotomy incision if major vascular injury or bowel injury occurs.
Detailed Surgical Approach / Technique
The anterior approach to the sacroiliac joint offers safe, reliable access to that structure and allows anterior plates to be positioned accurately across the joint. It also permits the exposure of the inner wall of the ala of the ilium, allowing fixation of associated iliac fractures. Paradoxically, although the sacroiliac joint is one of the most posterior structures in the entire pelvic ring, the anterior approach allows greater exposure and control than does the seemingly more logical posterior approach, because of the shape of the joint. Anteriorly, the joint is flat and directly available, whereas posteriorly it is overhung by the posterior iliac crest.
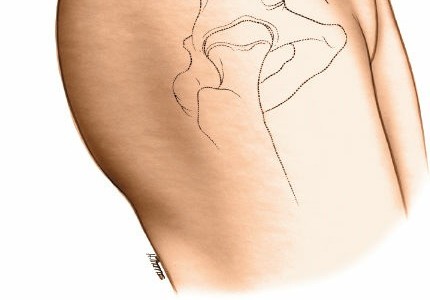
Landmarks and Incision
Landmarks
The anterior superior iliac spine (ASIS) and the anterior third of the iliac crest are subcutaneous and easy to palpate.

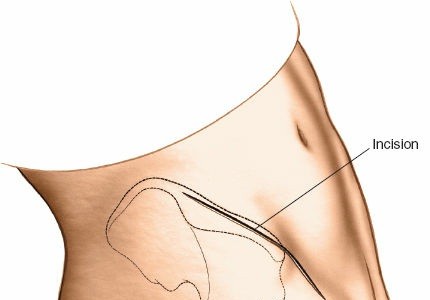
Incision
Make a long, curved incision over the iliac crest, beginning approximately 2 cm posterior to the ASIS and extending posteriorly along the crest for about 8-10 cm. The incision should be deep enough to reach the subcutaneous fat layer.
Dissection & Internervous Plane
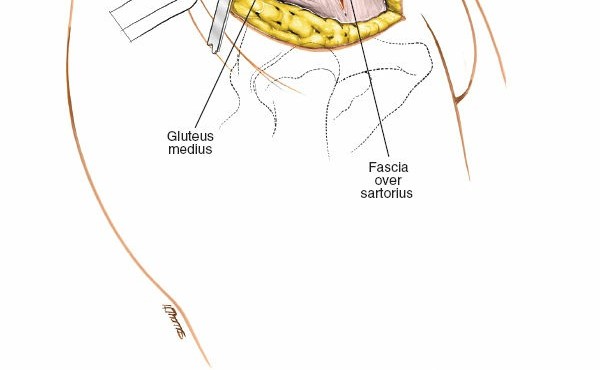
- Subcutaneous Dissection: Elevate skin flaps superiorly and inferiorly to expose the fascial attachments along the iliac crest. Care must be taken to protect the lateral femoral cutaneous nerve, which typically crosses the iliac crest approximately 2-3 cm posterior to the ASIS.
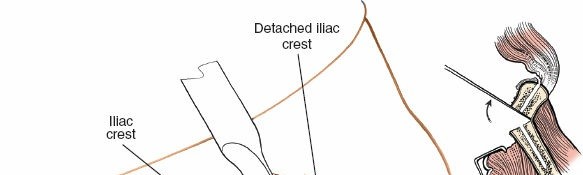
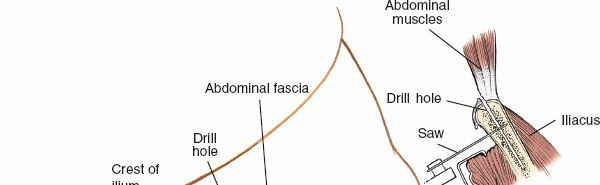
- External Oblique Fascia: Incise the external oblique fascia along the iliac crest, beginning posteriorly and extending anteriorly towards the ASIS. This incision should be slightly superior to the iliac crest to leave a cuff of fascia for later repair.
-
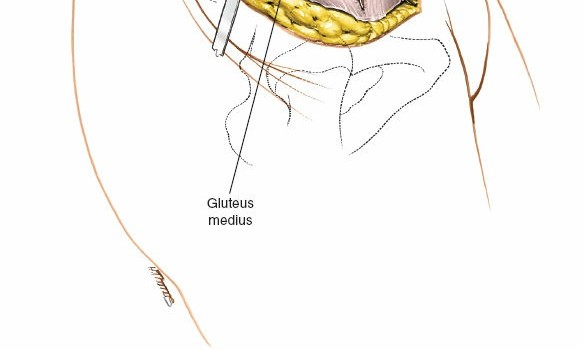
Elevation of Abdominal Wall Muscles: Subperiosteally elevate the internal oblique and transversus abdominis muscles from the inner lip of the iliac crest. This elevation creates a space between the abdominal wall muscles and the underlying iliacus muscle. The internervous plane here is between the internal oblique/transversus abdominis and the iliacus.
The muscles are carefully elevated from the iliac fossa.
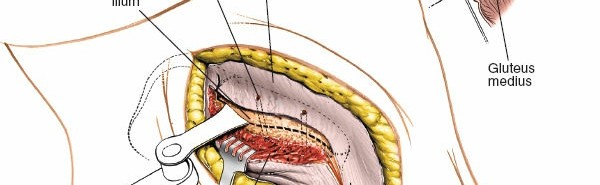
-
Retraction of Abdominal Contents: Using broad malleable retractors (e.g., Davidson retractors), gently retract the mobilized abdominal wall muscles, peritoneum, and contents (bowel, ureter) medially. The prior table tilt aids significantly in this step. The goal is to expose the entire iliac fossa and its contents.
The iliacus muscle is now visible, lining the iliac fossa.
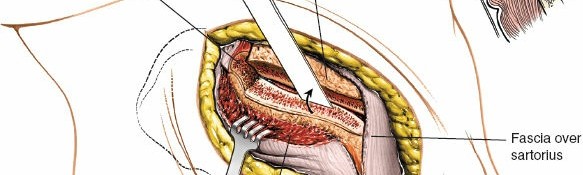
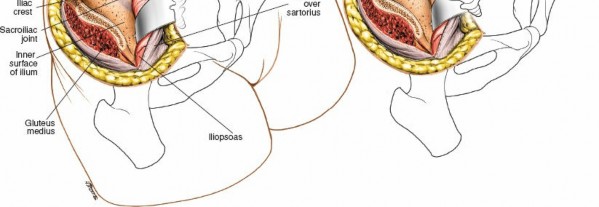
Exposure of the Sacroiliac Joint and Vascular Structures
- Iliacus Muscle Elevation: Incise the fascia overlying the iliacus muscle longitudinally, approximately 1-2 cm medial to the iliac crest. Subperiosteally elevate the iliacus muscle from the inner wall of the ilium. This maneuver exposes the inner table of the ilium.
-
Identification of Iliac Vessels: As the iliacus muscle is elevated and retracted, the major iliac vessels (common iliac artery and vein, external iliac artery and vein) will become visible lying on the medial aspect of the iliac fossa. These vessels must be meticulously identified, carefully mobilized, and continuously protected with broad malleable retractors throughout the remainder of the procedure. The ureter will typically be found crossing anterior to the common iliac artery.
The iliac vessels are critical anatomical structures in the surgical field. -
Direct Visualization of the SI Joint: Continue the subperiosteal dissection posteriorly along the inner iliac wall until the anterior capsule of the sacroiliac joint is clearly visualized. This appears as a dense fibrous structure marking the articulation between the ilium and the sacrum. The flat anterior surface of the joint is now directly accessible.
The anterior SI joint and sacral ala are now exposed, ready for reduction and fixation.
Reduction
With direct visualization, anatomical reduction of the SI joint disruption or associated fracture is achieved.
1.
Assessment of Displacement:
Visually inspect the joint for gapping, vertical displacement, or rotational deformity. Palpate the posterior aspect of the ilium through the incision to assess for rotational instability.
2.
Reduction Maneuvers:
*
Traction and Counter-Traction:
May be necessary for vertical shear components.
*
Direct Manipulation:
Using a Schanz pin placed in the iliac wing, reduction clamps (e.g., pointed reduction forceps, Faraboeuf clamps) applied directly to the ilium and sacrum, or specialized pelvic reduction clamps, the fractured/dislocated fragments can be anatomically realigned.
*
Buttress or Compression:
For iliac ala fractures, a Hohmann retractor can be used to buttress the outer wall while direct compression is applied.
3.
Confirmation of Reduction:
Intraoperative fluoroscopy (AP, inlet, and outlet views) is essential to confirm anatomical reduction in all planes. Direct visual inspection of the anterior joint line is also critical.
Direct visualization of the reduced SI joint.
Fixation
Once anatomical reduction is achieved and maintained, rigid fixation is performed.
1.
Plate Selection:
A contoured reconstruction plate (e.g., 3.5mm or 4.5mm) or a dedicated pelvic SI plate is typically used. The plate should be long enough to span the joint effectively, allowing for secure purchase in both the ilium and the sacrum.
2.
Plate Contouring:
The plate is contoured to fit the curvature of the anterior iliac fossa and cross the SI joint without impinging on neurovascular structures.
3.
Plate Application:
The plate is positioned to bridge the SI joint. For sacroiliac dislocations or fracture-dislocations, it is placed directly across the joint capsule onto the anterior sacral ala and iliac ala. For associated iliac fractures, the plate can be used to buttress the inner wall of the ilium and provide compression.
Anterior plating across the sacroiliac joint.
-
Screw Insertion:
- Iliac Screws: Screws are placed into the ilium first, ensuring adequate purchase in the cortical bone.
- Sacral Screws: Screws are then placed into the sacral ala. Careful consideration of sacral anatomy is paramount to avoid neurovascular injury. Fluoroscopic guidance (inlet, outlet, and lateral views) is mandatory to ensure appropriate screw trajectory and length, avoiding the sacral foramina (which contain nerve roots) and the central sacral canal. Aim for the dense bone of the sacral body or sacral ala.
- Compression: If a compression force is desired across the SI joint, eccentric drilling or lag screw technique can be employed.
- Final Confirmation: Final AP, inlet, and outlet fluoroscopic views are obtained to confirm plate and screw position, ensuring no intrapelvic penetration, adequate reduction, and stable fixation.
Closure
- Hemostasis: Ensure meticulous hemostasis.
- Drain Placement: A suction drain may be placed in the retroperitoneal space, deep to the abdominal wall muscles, especially if significant dissection or bleeding occurred.
- Muscle and Fascia Repair: The abdominal wall muscles (internal oblique and transversus abdominis) are reapproximated to the iliac crest through the fascial cuff left earlier. The external oblique fascia is then repaired.
- Subcutaneous and Skin Closure: Standard layered closure of the subcutaneous tissue and skin.
Complications & Management
While the anterior approach offers distinct advantages, it is not without potential complications. A thorough understanding of these risks and their management is crucial for all surgeons utilizing this approach.
Intraoperative Complications
-
Hemorrhage:
- Incidence: Varies, but can be significant due to proximity to major iliac vessels. Pelvic trauma itself often presents with substantial blood loss.
- Management: Meticulous dissection, careful retraction, and prompt recognition are key. Direct pressure, packing, vascular repair (by general or vascular surgeon), or embolization may be required.
-
Nerve Injury:
- Incidence: Lateral femoral cutaneous nerve (LFCN) neuropraxia is most common due to direct trauma or retraction. L5 nerve root (lumbosacral trunk) and sacral plexus injury are less common but more devastating, often due to errant screw placement.
- Management: Prophylactic protection of the LFCN during incision and retraction. For L5/sacral plexus, careful screw trajectory and length confirmation with fluoroscopy. If suspected intraoperatively, immediate removal of offending hardware. Postoperatively, conservative management for neuropraxia; surgical exploration for persistent deficits from retained hardware.
-
Ureteral Injury:
- Incidence: Rare, but possible during medial retraction of abdominal contents.
- Management: Identification with a Foley catheter and careful retraction. If injured, urology consultation for primary repair or stenting.
-
Bowel Injury:
- Incidence: Rare, typically from direct trauma during dissection or aggressive retraction.
- Management: Meticulous dissection. If suspected, general surgery consultation for repair.
-
Fixation Failure (Acute):
- Incidence: Low with appropriate technique, but can occur if bone quality is poor or reduction is unstable.
- Management: Revision with stronger hardware, supplementary fixation (e.g., iliosacral screws if appropriate), or conversion to a different approach.
Postoperative Complications
-
Infection:
- Incidence: SSI rates for pelvic trauma vary from 1-10%.
- Management: Strict aseptic technique, prophylactic antibiotics. Superficial infections: wound care, oral antibiotics. Deep infections: surgical debridement, IV antibiotics, possible hardware removal (after bone healing).
-
Wound Dehiscence/Hematoma/Seroma:
- Incidence: Common in pelvic trauma, especially with extensive soft tissue dissection.
- Management: Careful hemostasis, drain placement, meticulous layered closure. Hematoma/seroma: aspiration or surgical evacuation. Dehiscence: debridement, secondary closure, or wound VAC.
-
DVT/PE:
- Incidence: High in pelvic trauma patients.
- Management: Aggressive prophylaxis (mechanical, pharmacological with LMWH or DOACs) and early mobilization.
-
Hardware Failure:
- Incidence: Can occur with nonunion, poor bone quality, or excessive stress (e.g., early weight-bearing).
- Management: Revision surgery, often with bone grafting and stronger constructs.
-
Nonunion/Malunion:
- Incidence: Higher in complex, highly unstable injuries or with inadequate fixation.
- Management: Nonunion often requires revision surgery with bone grafting. Malunion may require osteotomy or arthrodesis for symptomatic correction.
-
Chronic Pain:
- Incidence: Multifactorial, can be due to residual instability, nerve irritation, or arthritis.
- Management: Multimodal pain management, physical therapy, SI joint injections, nerve blocks, or potential fusion in severe cases.
-
Heterotopic Ossification (HO):
- Incidence: Can occur around the SI joint or within the surgical dissection planes.
- Management: Prophylaxis (NSAIDs, radiation therapy) in high-risk patients. If symptomatic, surgical excision after maturation.
Complications & Management Table
| Complication | Incidence | Salvage Strategy |
|---|---|---|
| Intraoperative Hemorrhage | Moderate (variable by injury) | Direct pressure, packing, vascular repair, embolization |
| Lateral Femoral Cutaneous Neuropraxia | Common (transient) | Conservative management, reassurance |
| L5 Nerve Root/Sacral Plexus Injury | Rare (due to errant screw) | Immediate hardware removal, neurological consultation |
| Ureteral/Bowel Injury | Rare | Immediate surgical repair (urology/general surgery consult) |
| Acute Fixation Failure | Low (with proper technique) | Revision with stronger construct, supplementary fixation |
| Surgical Site Infection (SSI) | 1-10% | Debridement, IV antibiotics, potential hardware removal |
| Wound Dehiscence/Hematoma | Moderate | Drainage, debridement, secondary closure, wound VAC |
| DVT/Pulmonary Embolism (PE) | High (in pelvic trauma patients) | Aggressive prophylaxis, anticoagulation |
| Hardware Failure (Post-op) | Low to Moderate | Revision surgery, bone grafting, alternative fixation |
| Nonunion/Malunion | Low to Moderate | Revision surgery, bone grafting, osteotomy for malunion |
| Chronic Pain | Moderate to High (multifactorial) | Multimodal pain management, PT, injections, possible fusion |
| Heterotopic Ossification | Low to Moderate | Prophylaxis (NSAIDs/XRT), surgical excision (if symptomatic) |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following an anterior approach to the SI joint is crucial for optimizing outcomes, restoring function, and preventing complications. The protocol must be individualized based on the patient's age, bone quality, severity of injury, stability of fixation, and overall medical status.
Phase 1: Immediate Post-Operative (Weeks 0-6)
- Goals: Pain control, wound healing, DVT prophylaxis, gentle mobilization, protection of fixation.
-
Weight-Bearing:
- Typically non-weight bearing (NWB) or touch-down weight-bearing (TDWB) on the operated side to protect the healing joint and fixation. This is maintained until radiographic evidence of initial healing and clinical stability is confirmed (usually around 6-8 weeks).
- Ambulation with assistive devices (walker, crutches).
- Pain Management: Multimodal approach including opioids, NSAIDs (if not contraindicated by fusion or renal issues), acetaminophen, and nerve blocks.
- DVT Prophylaxis: Pharmacological (e.g., LMWH) and mechanical (e.g., SCDs) as per institutional guidelines, initiated immediately post-op.
-
Early Mobilization:
- Bed mobility training, transfers (bed to chair).
- Gentle active and passive range of motion (ROM) for hips and knees within pain limits.
- Avoidance of hip flexion beyond 90 degrees or significant rotation, which can put stress on the SI joint.
- Static core activation (gentle abdominal bracing) if tolerated.
- Wound Care: Daily inspection for signs of infection or dehiscence.
Phase 2: Intermediate Healing (Weeks 6-12)
- Goals: Gradual increase in weight-bearing, restoration of joint mobility, initiation of muscle strengthening.
-
Weight-Bearing:
- Progression to partial weight-bearing (PWB) with assistive devices, typically after radiographic evidence of early union and clinical assessment of stability.
- Gradual increase in load as tolerated, moving towards full weight-bearing (FWB) by week 10-12, contingent on healing.
-
Therapeutic Exercises:
- Range of Motion: Continued hip and lumbar spine ROM exercises.
- Strengthening: Initiation of isometric strengthening for hip abductors, adductors, extensors, and gentle core stabilizers (transversus abdominis, multifidus). Avoid deep twisting or rotational movements of the trunk initially.
- Gait Training: Progression from assistive devices to independent ambulation as strength and balance improve. Focus on normalized gait pattern.
- Pain Management: Transition from opioid to non-opioid analgesics.
Phase 3: Advanced Strengthening & Functional Return (Weeks 12-24+)
- Goals: Full weight-bearing, advanced strengthening, proprioception, return to functional activities.
- Weight-Bearing: Typically FWB by this stage.
-
Therapeutic Exercises:
- Advanced Strengthening: Progressive resistive exercises for hip and core musculature. Focus on functional strength and endurance.
- Proprioceptive Training: Balance exercises, single-leg stance.
- Endurance Training: Low-impact activities such as cycling or swimming.
- Sport-Specific Training: For athletes, gradual introduction of sport-specific movements and drills, under guidance.
- Activity Progression: Gradual return to activities of daily living. Return to work may be phased, depending on physical demands. High-impact sports or heavy lifting typically deferred until 6 months or later, and only after complete radiographic healing and full restoration of strength and function.
- Hardware Removal: Rarely indicated unless symptomatic (e.g., bursitis over the plate). Typically considered after 12-18 months, if at all.
Throughout all phases, patient education regarding activity restrictions, body mechanics, and warning signs of complications is paramount. Regular clinical and radiographic follow-up is necessary to monitor healing and guide rehabilitation progression.
Summary of Key Literature / Guidelines
The management of sacroiliac joint pathology, particularly in the context of pelvic ring injuries, has evolved significantly, with the anterior approach gaining increasing recognition for its distinct advantages. Key literature and guidelines underscore its utility in specific scenarios.
Historical reviews and foundational texts in orthopedic trauma, such as the AO Principles of Fracture Management, have long described various approaches to the pelvic ring, including anterior routes. Early proponents highlighted the benefits of direct visualization of the anterior SI joint and the ability to address associated iliac fractures directly.
Advantages of the Anterior Approach (as supported by literature):
*
Direct Visualization:
Unlike posterior approaches, the anterior approach provides direct, unobstructed visualization of the anterior SI joint capsule and the inner wall of the ilium. This facilitates anatomical reduction, especially for gapping or rotational deformities, and allows precise placement of fixation hardware.
*
Addressing Iliac Fractures:
The literature consistently emphasizes the superiority of the anterior approach for managing iliac ala fractures that propagate into the SI joint. Plates can be applied to buttress or compress these fractures effectively.
*
Minimizing Nerve Injury:
While proximity to major vessels requires vigilance, the anterior approach can potentially minimize the risk of injury to the superior gluteal neurovascular bundle, which is a concern with posterior trans-iliac-sacral screw placement, especially in the setting of pelvic deformity.
*
Biomechanical Stability:
Studies evaluating the biomechanical stability of anterior SI plating have demonstrated its efficacy in restoring stability, particularly in APC-type injuries. While some complex VS injuries may benefit from a combined anterior-posterior fixation, anterior plating alone or in conjunction with pubic symphyseal plating can provide sufficient stability for many anterior pelvic ring disruptions.
Comparative Studies:
* Numerous studies have compared anterior and posterior fixation methods for SI joint disruptions. While no single approach is universally superior for all pelvic ring injuries, the anterior approach is often favored for highly unstable APC injuries with significant anterior gapping.
* For pure sacral fractures, iliosacral screw fixation via a posterior approach often remains the gold standard, but the anterior approach offers a valuable alternative or adjunct for complex anterior sacral components.
* Clinical outcomes, including pain reduction, functional recovery, and complication rates, are often comparable between well-selected anterior and posterior approaches when performed by experienced surgeons. However, specific injury patterns may dictate the optimal approach.
Current Guidelines:
* Current trauma guidelines, such as those from the Orthopaedic Trauma Association (OTA) and AO Trauma, advocate for individualized treatment strategies based on the specific injury pattern (e.g., Young-Burgess or Tile classification), patient comorbidities, and surgeon expertise.
* The anterior approach is explicitly recognized as a viable and often preferred option for specific patterns of pelvic ring instability involving the anterior SI joint or adjacent iliac fractures.
* Emphasis is consistently placed on achieving anatomical reduction and rigid fixation to optimize long-term outcomes and prevent chronic pain and disability.
In conclusion, the anterior approach to the sacroiliac joint stands as a valuable and often indispensable technique in the armamentarium of the orthopedic trauma surgeon. Its capacity to provide direct visualization, facilitate anatomical reduction, and allow robust fixation of the anterior SI joint and associated iliac fractures positions it as a superior option for appropriately selected patients, as supported by established surgical principles and clinical literature.
Clinical & Radiographic Imaging
You Might Also Like