Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand

Anatomy and Surgical Approaches of the Forearm, Wrist, and Hand
Definition
Safe surgical dissection and exposure require an in-depth knowledge of anatomy. In no place is this more relevant than in the surgical approaches to the hand, wrist, and forearm. The critical aspect of successful surgical approaches in the forearm and wrist is the judicious use of internervous planes. These planes lie between muscles that are innervated by different nerves. Dissection through internervous planes allows extensive mobilization and exposure without risk of muscle denervation. Unique to the hand, wrist, and forearm is the complex relationship of not only the muscles overlying bone but also the close proximity and delicate balance of accessory anatomic structures, including tendons, vessels, and nerves. Consideration of postoperative function of the extremity should start with preoperative surgical planning. Elective incisions should not cross flexion creases (antecubital fossa, wrist, or digit creases) to avoid scar contracture. If necessary, a transverse limb or zigzag incision should be incorporated to avoid crossing flexion creases perpendicularly.
Introduction & Epidemiology
The upper extremity, particularly the forearm, wrist, and hand, represents a complex and highly specialized biomechanical unit essential for daily function and interaction with the environment. Surgical interventions in this region are diverse, ranging from trauma management (fractures, dislocations, tendon lacerations, nerve injuries) to degenerative conditions (osteoarthritis, tendinopathies, nerve entrapments) and congenital anomalies. Given the intricate nature of its anatomy, even minor surgical missteps can lead to significant functional impairment, chronic pain, or neurovascular compromise. A thorough understanding of the three-dimensional relationships of osseous, ligamentous, muscular, tendinous, neurovascular, and cutaneous structures is paramount for achieving optimal surgical outcomes and minimizing iatrogenic injury.
Epidemiologically, injuries to the forearm, wrist, and hand are common across all age groups. Distal radius fractures are among the most frequently encountered fractures, often occurring due to falls on an outstretched hand, particularly in osteoporotic individuals. Scaphoid fractures are also prevalent, especially in young active adults, and carry a high risk of nonunion and avascular necrosis due to their peculiar blood supply. Lacerations involving tendons and nerves are common in industrial and domestic settings, demanding precise anatomical repair. Chronic conditions such as carpal tunnel syndrome, cubital tunnel syndrome, and various forms of tendinitis (e.g., De Quervain's tenosynovitis, trigger finger) necessitate surgical intervention when conservative measures fail. The high incidence of these conditions underscores the critical need for a detailed and updated understanding of surgical approaches and their underlying anatomical principles.
Surgical Anatomy & Biomechanics
The anatomy of the hand, wrist, and forearm is characterized by a dense packing of functionally diverse structures within confined spaces. Surgical success is predicated upon a comprehensive understanding of these relationships.
Forearm Anatomy
The forearm extends from the elbow to the wrist and contains two bones, the radius and ulna, connected by the interosseous membrane. This arrangement allows for pronation and supination, movements critical for hand function.
Bones and Joints
- Radius: The lateral bone, articulating with the capitellum of the humerus proximally and the carpal bones (scaphoid and lunate) distally. Its shape changes significantly from a cylindrical shaft to a broader, triangular distal metaphysis.
- Ulna: The medial bone, articulating with the trochlea of the humerus proximally and primarily forming the elbow joint. Distally, it forms the ulnar head and styloid, articulating with the triangular fibrocartilage complex (TFCC) rather than directly with carpal bones.
- Proximal Radioulnar Joint (PRUJ): Allows pronation and supination through rotation of the radial head within the annular ligament.
- Distal Radioulnar Joint (DRUJ): Crucial for forearm rotation. The radius pivots around the fixed ulna. Stabilized by the TFCC.
Muscles and Tendons
The forearm muscles are divided into anterior (flexor-pronator) and posterior (extensor-supinator) compartments.
Anterior Compartment (Flexor-Pronator Group)
Superficial layer (all originate from medial epicondyle):
*
Pronator Teres:
Pronates and flexes forearm.
*
Flexor Carpi Radialis (FCR):
Flexes and radially deviates wrist.
*
Palmaris Longus:
Weak wrist flexor (absent in ~15%).
*
Flexor Carpi Ulnaris (FCU):
Flexes and ulnarly deviates wrist.
Intermediate layer:
*
Flexor Digitorum Superficialis (FDS):
Flexes proximal interphalangeal (PIP) joints and wrist.

Deep layer:
*
Flexor Digitorum Profundus (FDP):
Flexes distal interphalangeal (DIP) joints and wrist. The medial half (digits 4, 5) is supplied by the ulnar nerve, and the lateral half (digits 2, 3) by the anterior interosseous nerve (AIN), a branch of the median nerve. This forms a critical internervous plane.
*
Flexor Pollicis Longus (FPL):
Flexes thumb IP joint. Supplied by AIN.
*
Pronator Quadratus:
Primary pronator of the forearm. Supplied by AIN.
Posterior Compartment (Extensor-Supinator Group)
Superficial layer (all supplied by radial nerve or its deep branch):
*
Brachioradialis:
Flexes elbow.
*
Extensor Carpi Radialis Longus (ECRL):
Extends and radially deviates wrist.
*
Extensor Carpi Radialis Brevis (ECRB):
Extends and radially deviates wrist.
*
Extensor Digitorum (ED):
Extends MCP and IP joints of digits 2-5.
*
Extensor Digiti Minimi (EDM):
Extends little finger.
*
Extensor Carpi Ulnaris (ECU):
Extends and ulnarly deviates wrist.
Deep layer (all supplied by posterior interosseous nerve (PIN), a branch of the deep radial nerve):
*
Supinator:
Supinates forearm. The deep branch of the radial nerve pierces it.
*
Abductor Pollicis Longus (APL):
Abducts thumb and wrist.
*
Extensor Pollicis Brevis (EPB):
Extends thumb MCP joint.
*
Extensor Pollicis Longus (EPL):
Extends thumb IP joint, loops around Lister's tubercle.
*
Extensor Indicis (EI):
Extends index finger.
Neurovascular Structures
- Median Nerve: Travels through the anterior compartment, initially between pronator teres heads, then between FDS and FDP. Gives off the AIN.
- Ulnar Nerve: Enters the forearm after passing posterior to the medial epicondyle (cubital tunnel), travels deep to FCU.
- Radial Nerve: Divides into superficial (sensory) and deep (motor) branches at the level of the elbow. The deep branch becomes the PIN after piercing the supinator.
-
Brachial Artery:
Divides into radial and ulnar arteries at the cubital fossa.
- Radial Artery: Courses distally with the superficial radial nerve, lies between brachioradialis and FCR tendons at the wrist.
- Ulnar Artery: Courses distally with the ulnar nerve, deep to FCU. Gives off the common interosseous artery, which divides into anterior and posterior interosseous arteries.
Wrist Anatomy
The wrist is a complex bicondylar joint system connecting the forearm to the hand, allowing for a wide range of motion.
Bones and Joints
- Distal Radius: Articular surface for scaphoid and lunate.
- Distal Ulna: Head and styloid, separated from carpus by TFCC.
-
Carpal Bones (8):
Arranged in two rows.
- Proximal row: Scaphoid, Lunate, Triquetrum, Pisiform. The scaphoid is critical as it bridges both rows.
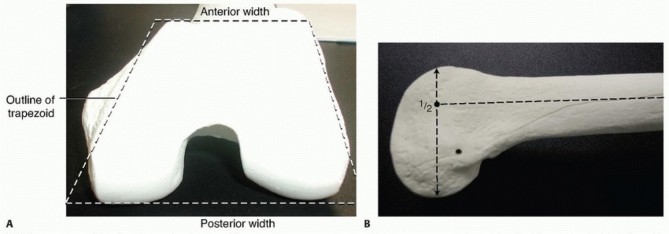
-
Distal row:
Trapezium, Trapezoid, Capitate, Hamate. These articulate with the metacarpals.
Ligaments
Numerous intrinsic and extrinsic ligaments provide stability. Key ligaments include the scapholunate (SL) and lunotriquetral (LT) interosseous ligaments, and the strong extrinsic volar radiocarpal ligaments (radioscaphocapitate, long and short radiolunate). The TFCC stabilizes the DRUJ and acts as a primary ulnocarpal load bearer.
Extensor Compartments
The dorsal wrist contains six extensor compartments, defined by fibrous retinacular septa, which guide and protect the extensor tendons.
1.
APL, EPB
(De Quervain's tunnel)
2.
ECRL, ECRB
3.
EPL
(hooks around Lister's tubercle)
4.
ED, EI
5.
EDM
6.
ECU
(subsheath stabilization)

Carpal Tunnel and Guyon's Canal
- Carpal Tunnel: Formed by the carpal bones dorsally and the transverse carpal ligament (flexor retinaculum) volarly. Contains the median nerve and nine flexor tendons (4 FDS, 4 FDP, 1 FPL).
- Guyon's Canal (Ulnar Canal): Formed by the pisiform, hook of hamate, and overlying palmar carpal ligament. Transmits the ulnar nerve and artery.
Hand Anatomy
The hand is a marvel of evolutionary engineering, enabling precision grip, power grasp, and tactile discrimination.
Bones and Joints
- Metacarpals (5): Articulate with carpal bones proximally and phalanges distally.
- Phalanges (14): Proximal, middle (absent in thumb), and distal.
- Joints: Carpometacarpal (CMC), Metacarpophalangeal (MCP), Proximal Interphalangeal (PIP), Distal Interphalangeal (DIP).
Muscles and Tendons
- Extrinsic Muscles: Forearm muscles whose tendons insert into the hand.
-
Intrinsic Muscles:
Originate and insert within the hand.
- Thenar Muscles: Abductor Pollicis Brevis (APB), Flexor Pollicis Brevis (FPB), Opponens Pollicis (OP). Primarily median nerve innervation (recurrent motor branch).
- Hypothenar Muscles: Abductor Digiti Minimi (ADM), Flexor Digiti Minimi Brevis (FDMB), Opponens Digiti Minimi (ODM). Ulnar nerve innervation.
- Lumbricals (4): Flex MCPs, extend PIP/DIPs. Lateral two (index, middle) supplied by median nerve; medial two (ring, little) by ulnar nerve.
-
Interossei (7):
- Palmar Interossei (3): Adduct fingers (PAD). Ulnar nerve.
-
Dorsal Interossei (4):
Abduct fingers (DAB). Ulnar nerve.
Neurovascular Structures
- Median Nerve: Terminal branches include the recurrent motor branch to the thenar muscles and common/proper digital nerves.
- Ulnar Nerve: Divides into superficial (sensory) and deep (motor) branches. The deep motor branch innervates most intrinsic muscles.
- Radial Nerve (Superficial branch): Primarily sensory innervation to the dorsal aspect of the thumb, index, middle, and radial half of the ring finger.
-
Arteries:
Superficial and deep palmar arches, formed by anastomoses of radial and ulnar arteries, give rise to common and proper digital arteries.
Pulley System
The flexor tendons within the digits are held close to the bone by a retinacular pulley system (A1-A5 annular pulleys, C1-C3 cruciate pulleys). Damage to these pulleys can lead to bowstringing and loss of mechanical efficiency. The A1 pulley is often implicated in trigger finger.
Biomechanics
Forearm rotation (pronation/supination) relies on synchronized movement at the PRUJ and DRUJ. Wrist flexion/extension and radial/ulnar deviation are complex motions involving both radiocarpal and midcarpal joints. The hand's ability to perform fine motor tasks and strong grasping depends on the balance between extrinsic and intrinsic muscle groups, an intact pulley system, and sensory feedback. Pathologies disrupting these intricate balances often necessitate surgical intervention.
Indications & Contraindications
Surgical intervention in the forearm, wrist, and hand is indicated for a myriad of conditions where non-operative management has failed or is unlikely to achieve satisfactory functional outcomes. Contraindications are generally relative, often pertaining to the patient's overall health status or local tissue conditions.
Indications
-
Traumatic Injuries:
- Displaced or unstable fractures (e.g., distal radius, scaphoid, metacarpal, phalangeal).
- Joint dislocations (e.g., lunate, perilunate, MCP/PIP/DIP dislocations failing closed reduction).
- Tendon lacerations (flexor/extensor) or avulsions.
- Nerve lacerations or severe compression injuries (e.g., compartment syndrome).
- Vascular injuries requiring repair.
- Ligamentous ruptures causing instability (e.g., scapholunate dissociation).
- Severe soft tissue injuries, including degloving injuries, requiring reconstruction.
-
Degenerative Conditions:
- Advanced osteoarthritis (e.g., CMC joint of the thumb, distal radioulnar joint, wrist arthrosis) refractory to conservative care.
- Chronic tendinopathies with structural damage (e.g., De Quervain's tenosynovitis, trigger finger, epicondylitis).
- Nerve entrapment syndromes (e.g., carpal tunnel syndrome, cubital tunnel syndrome) with progressive neurological deficit or failed non-operative treatment.
-
Tumors:
- Excision of symptomatic benign tumors (e.g., ganglion cysts, enchondromas).
- Biopsy or excision of suspected malignant tumors.
-
Infections:
- Severe hand infections (e.g., necrotizing fasciitis, deep space infections, osteomyelitis) requiring debridement and drainage.
-
Congenital Deformities:
- Correction of syndactyly, polydactyly, radial club hand, etc., to improve function.
-
Reconstructive Procedures:
- Tendon transfers for irreparable nerve injury or muscle paralysis.
- Vascularized bone grafting for nonunion (e.g., scaphoid).
Contraindications
-
Absolute Contraindications:
- Unstable medical comorbidities precluding safe anesthesia and surgery.
- Active infection at the surgical site (except when surgery is for infection management).
- Patient refusal or inability to comply with postoperative rehabilitation protocols.
-
Relative Contraindications:
- Severe soft tissue compromise (e.g., severe swelling, blistering, extensive devitalization) necessitating delayed definitive fixation.
- Poor nutritional status or other systemic factors that may impair wound healing.
- Uncontrolled diabetes, peripheral vascular disease, or immunosuppression (increased risk of infection/poor healing).
- Smoking (increased risk of nonunion, poor healing, infection).
- Significant psychological comorbidities affecting compliance.
| Condition | Operative Indication | Non-Operative Indication / Consideration |
|---|---|---|
| Fractures | Displaced, unstable, intra-articular, open fractures. Nonunion. | Minimally displaced, stable, closed fractures. High surgical risk. |
| Dislocations | Failed closed reduction, irreducible, chronic instability. | Acute, reducible, stable dislocations. |
| Tendon Lacerations | Complete lacerations, significant partial lacerations. | Minor partial lacerations (rarely). |
| Nerve Lacerations/Compression | Complete transection, progressive neurological deficit, severe compression. | Mild compression, early symptoms, no motor deficit. |
| Osteoarthritis | Severe pain, functional limitation, failed conservative therapy. | Mild to moderate pain, initial presentation, amenable to bracing, NSAIDs, injections. |
| Tenosynovitis/Tendinopathy | Chronic symptoms, failed conservative care, mechanical locking. | Acute onset, mild symptoms, amenable to rest, splinting, NSAIDs, injections. |
| Tumors | Symptomatic, growing, suspicious for malignancy. | Asymptomatic, stable, confirmed benign and non-problematic. |
| Infections | Deep space infection, abscess, necrotizing fasciitis, osteomyelitis. | Superficial cellulitis responding to antibiotics. |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is crucial to anticipate potential challenges, optimize exposure, and mitigate risks.
Pre-Operative Planning
- Clinical Assessment: Detailed history and physical examination, including neurovascular status, range of motion, and assessment of skin integrity.
-
Imaging:
- Radiographs: Standard AP, lateral, and oblique views are essential for bony pathology. Specialized views (e.g., scaphoid views, pronated/supinated views for DRUJ) may be required.
- CT Scan: Indicated for complex intra-articular fractures, carpal kinematics, or to assess nonunion/malunion. Essential for 3D reconstruction in complex trauma.
- MRI: Best for soft tissue assessment (ligaments, tendons, cartilage, nerves, masses).
- Ultrasound: Useful for dynamic assessment of tendons, nerve integrity, and evaluation of superficial masses.
- Tourniquet Time Planning: Estimate procedure duration to manage tourniquet inflation time (generally <90-120 minutes, with reinflation considerations after a 15-20 minute reperfusion period).
- Implant Selection: Pre-contouring plates or selecting appropriate screw sizes based on anatomy and pathology.
- Patient Education: Discuss the procedure, expected outcomes, and potential complications, ensuring informed consent.
Patient Positioning
For most forearm, wrist, and hand procedures, the patient is positioned
supine
on the operating table.
*
Arm Board:
The affected arm is typically placed on a specialized hand table or arm board, ensuring full access and stability. The arm board should be securely positioned and padded to prevent nerve compression (e.g., ulnar nerve at the elbow).
*
Tourniquet:
A pneumatic tourniquet is applied to the upper arm. The skin underneath should be protected with appropriate padding to prevent pressure necrosis.
*
Anesthesia:
Regional anesthesia (e.g., interscalene or supraclavicular block) combined with general anesthesia is often preferred for prolonged procedures or those requiring significant postoperative analgesia.
*
Sterile Field:
The extremity is prepared and draped to allow ample sterile working space, often including the entire hand, wrist, and forearm, up to the elbow or higher. For forearm fractures requiring plating, the elbow joint must remain free to allow manipulation and assessment of rotation.
*
Image Intensifier (Fluoroscopy):
Essential for intraoperative assessment of reduction and fixation in bony procedures. Ensure the C-arm can be positioned without contamination of the sterile field.
Detailed Surgical Approach / Technique
Successful surgical exposure in the forearm, wrist, and hand requires meticulous attention to anatomical landmarks, judicious dissection through internervous planes, and careful handling of delicate neurovascular structures.
Forearm Approaches
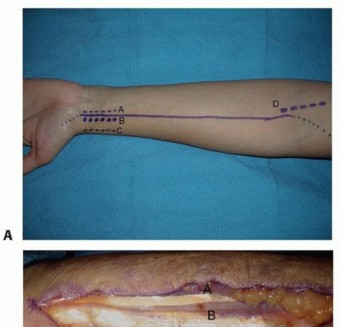
Volar (Henry) Approach to the Radius
*
Indication:
Fractures of the radial shaft, distal radius, osteotomies, tumor excisions.
*
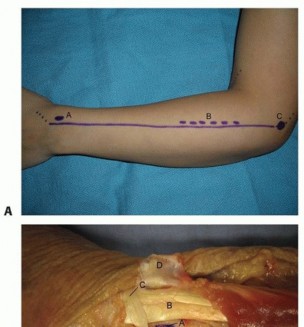
Incision:
Longitudinal incision on the volar aspect of the forearm, centered over the radius, extending from the elbow crease to the wrist crease, avoiding crossing flexion creases perpendicularly. For distal radius, may be centered more distally.
*
Dissection:
1. Incise skin and superficial fascia. Identify and protect the
lateral antebrachial cutaneous nerve
(LACN) and potentially the
superficial radial nerve
branches if extending distally.
2. Identify the
brachioradialis
muscle laterally and the
flexor carpi radialis (FCR)
tendon medially (distally).
3. The
internervous plane
for the Henry approach lies between the brachioradialis (radial nerve) and the pronator teres/FCR (median nerve).
4. Proximally, identify the
pronator teres
. Retract the brachioradialis laterally and the pronator teres medially. Deep to the pronator teres, the
radial artery
and
median nerve
will be identified. Protect them.
5. Continue dissecting between the brachioradialis laterally and the FCR/FDS medially. The
flexor pollicis longus (FPL)
muscle belly will become visible, originating from the volar aspect of the radius and interosseous membrane.
6. Retract the FPL, FDS, and median nerve medially. The
anterior interosseous artery and nerve
run along the interosseous membrane and must be protected.
7. The radius is now exposed. Its volar surface is covered by the
pronator quadratus
distally, and more proximally by the FPL origin.

*
Closure:
Layered closure, ensuring muscle reapproximation, followed by subcutaneous tissue and skin.
Dorsal (Thompson) Approach to the Radius
- Indication: Fractures of the radial shaft, especially those requiring access to the posterior surface. Less commonly used than Henry.
- Incision: Longitudinal incision on the dorsal aspect of the forearm, centered over the radius, from the lateral epicondyle to the Lister's tubercle.
-
Dissection:
- Incise skin and superficial fascia. Identify and protect sensory branches of the superficial radial nerve and posterior antebrachial cutaneous nerve .
- The internervous plane lies between the ECRB/ECRL (radial nerve) and the extensor digitorum communis/extensor indicis (PIN).
- Proximally, identify the brachioradialis and extensor carpi radialis longus/brevis laterally. Medially, identify the extensor digitorum communis .
- Retract the ECRB/ECRL laterally and the extensor digitorum communis medially.
-
Deep to the extensor mass, the
supinator
muscle becomes visible. The
posterior interosseous nerve (PIN)
, a motor branch of the deep radial nerve, penetrates the supinator. Careful dissection is required to protect the PIN, especially when reflecting the supinator. The PIN enters the supinator through the Arcade of Frohse.
- Closure: Layered closure.
Ulnar Approach to the Ulna
- Indication: Fractures of the ulnar shaft (e.g., Monteggia fractures), osteotomies, tumor excision.
- Incision: Direct longitudinal incision over the subcutaneous border of the ulna.
-
Dissection:
- Incise skin and subcutaneous tissue directly over the palpable ulnar shaft.
- Identify and protect branches of the medial antebrachial cutaneous nerve .
- The ulna is largely subcutaneous along its medial border, making direct access straightforward.
- The flexor carpi ulnaris (FCU) and flexor digitorum profundus (FDP) attach to the medial and volar aspects of the ulna. The extensor carpi ulnaris (ECU) attaches dorsally.
- The ulnar nerve and ulnar artery run deep to the FCU proximally and become more superficial distally, radial to the FCU tendon. Exercise extreme caution.
- Closure: Layered closure.
Wrist Approaches
Volar Approach to the Wrist (Distal Radius / Carpal Tunnel)
- Indication: Distal radius fractures, carpal tunnel release, carpal bone pathology (e.g., scaphoid nonunion), tendon repairs.
-
Incision:
- Distal Radius: A longitudinal incision, 5-8 cm in length, placed just ulnar to the FCR tendon, extending from the wrist crease proximally. Can be extended proximally in line with the Henry approach or distally in line with the thenar crease.
-
Carpal Tunnel Release:
A longitudinal incision over the transverse carpal ligament, starting at the distal wrist crease and extending into the palm, often utilizing a zigzag or slightly curvilinear trajectory to avoid scar contracture. For endoscopic release, smaller portals are used.

-
Dissection (Distal Radius):
- Incise skin and superficial fascia. Identify the palmar cutaneous branch of the median nerve and branches of the lateral antebrachial cutaneous nerve (if incision extends radially).
- Identify the FCR tendon sheath . The incision should be between the FCR and the radial artery (radial to FCR).
- The radial artery must be protected. It lies radial to the FCR tendon.
- Deep to the FCR tendon, expose the flexor pollicis longus (FPL) and the flexor digitorum profundus (FDP) .
- The pronator quadratus muscle covers the volar aspect of the distal radius. This muscle can be sharply elevated from its radial origin to expose the bone, taking care to protect the anterior interosseous nerve which lies on the interosseous membrane.
- The median nerve and flexor tendons are deep and ulnar, protected by the pronator quadratus and then the transverse carpal ligament.
-
Dissection (Carpal Tunnel Release - Open):
- Incise skin and subcutaneous tissue. Identify and protect the palmar cutaneous branch of the median nerve (often radial to the incision).
- Identify the transverse carpal ligament (flexor retinaculum).
- Carefully incise the transverse carpal ligament longitudinally, starting distally and proceeding proximally, ensuring the median nerve and its motor branch are not injured. The motor branch typically arises from the radial side of the median nerve and loops volarly.
- Inspect for any remaining constricting fibers.
-
Confirm full decompression of the median nerve.
- Closure: Subcutaneous closure and skin closure.
Dorsal Approach to the Wrist
- Indication: Dorsal wrist ganglion excision, wrist arthrodesis, scaphoid fracture fixation (for some patterns), ligament repair, synovectomy, dorsal plating of distal radius fractures.
- Incision: Longitudinal or transverse incision centered over the wrist joint. A transverse incision at the wrist crease offers better cosmesis but limits extensile exposure. A longitudinal incision between the 3rd and 4th extensor compartments provides excellent exposure for general wrist surgery.
-
Dissection:
- Incise skin and subcutaneous tissue. Identify and protect sensory branches of the superficial radial nerve and dorsal cutaneous branch of the ulnar nerve .
- Identify the extensor retinaculum . For direct access to the carpus, make a longitudinal incision in the retinaculum, typically between the 3rd (EPL) and 4th (ED, EI) compartments, then reflect the retinaculum proximally and distally, or radially and ulnarly.
- Carefully retract the extensor tendons. The posterior interosseous nerve (PIN) , a purely sensory nerve at this level, lies deep to the 4th compartment and can be identified and resected if necessary for wrist denervation procedures.
- Expose the underlying carpal bones and ligaments.
- Closure: Repair the extensor retinaculum if possible or leave it open if excessive pressure is anticipated. Layered closure.
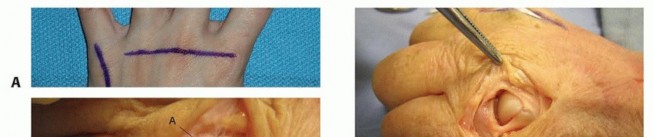
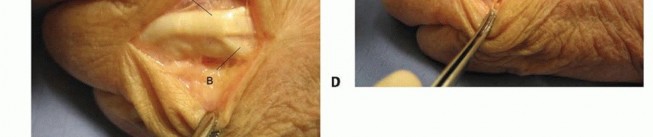
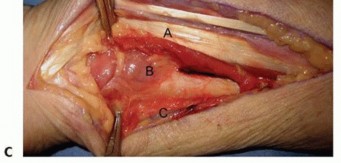
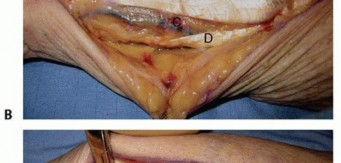
Radial Approach to the Scaphoid
- Indication: Scaphoid fracture fixation, nonunion repair.
- Incision: A curvilinear incision on the radial aspect of the wrist, extending from the dorsal wrist crease distally towards the base of the first metacarpal, paralleling the radial border of the snuffbox.
-
Dissection:
- Incise skin and subcutaneous tissue. Meticulously identify and protect branches of the superficial radial nerve .
- Identify the tendons of the first extensor compartment (APL, EPB) and the second extensor compartment (ECRL, ECRB) .
- The approach typically proceeds between the first and second extensor compartments, or between the radial artery and the FCR tendon volarly.
- Retract the radial artery radially. Identify the FCR tendon and retract it ulnarly.
- Deep to the FCR tendon, visualize the flexor carpi radialis brevis (not a distinct muscle, but a deep part of FCR tendon attachment) and the underlying trapezium .
-
The
scaphoid tuberosity
can be palpated. Further dissection carefully exposes the scaphoid. Take care to preserve the periscaphoid vascular supply.
- Closure: Layered closure, ensuring nerve protection.
Hand Approaches
Carpal Tunnel Release (See above)
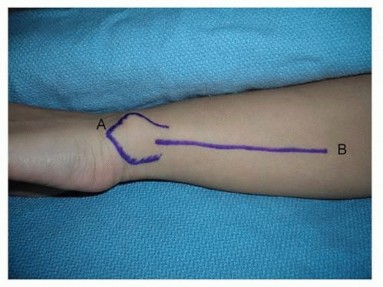
De Quervain's Tenosynovitis Release
- Indication: Pain and tenderness at the radial styloid, positive Finkelstein's test, unresponsive to conservative treatment.
- Incision: Transverse or longitudinal incision over the first dorsal extensor compartment at the radial styloid. A transverse incision is often preferred for cosmetic reasons.
-
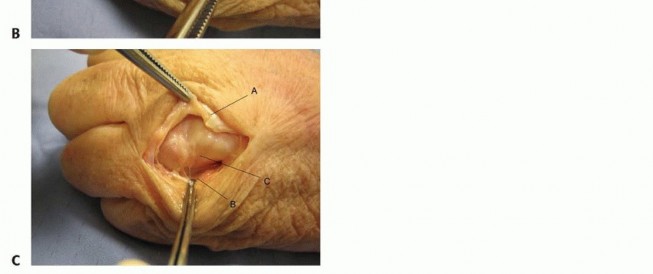
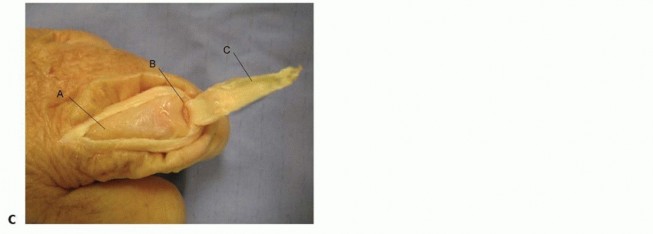
Dissection:
- Incise skin and subcutaneous tissue. Identify and protect all branches of the superficial radial nerve , which are highly variable and at risk.
- Expose the first dorsal extensor compartment , containing APL and EPB tendons. The compartment roof is often thickened.
- Carefully incise the retinaculum longitudinally along its dorsal aspect. Inspect for accessory compartments or septa that may entrap the tendons.
- Ensure complete release of both APL and EPB tendons.
-
Closure:
Skin closure.
Trigger Finger Release
- Indication: Painful locking or catching of a digit due to thickening of the A1 pulley.
- Incision: Small transverse or longitudinal incision over the A1 pulley at the metacarpophalangeal (MCP) joint crease (distal palmar crease).
-
Dissection:
- Incise skin and subcutaneous tissue. Identify and protect the digital nerves and arteries .
- The A1 pulley is a distinct fibrous band overlying the flexor tendons.
-
Carefully incise the A1 pulley longitudinally from distal to proximal, ensuring complete release. Verify free gliding of the flexor tendons. Take care not to injure the underlying FDS and FDP tendons.

- Closure: Skin closure.
Digital Nerve & Vessel Exposure
- Indication: Nerve laceration, neuroma excision, vessel repair.
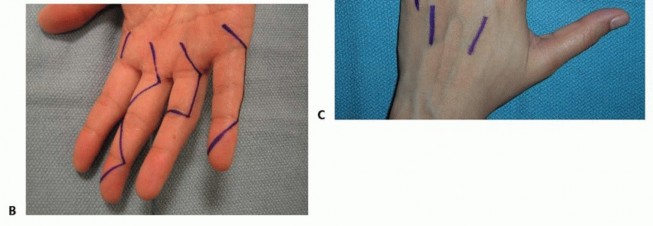
- Incision: Midaxial incision along the side of the digit, extending from the distal palmar crease to the distal interphalangeal joint. Avoid straight incisions across flexion creases. Alternatively, Brunner's zigzag incisions are commonly used in the palm and digits.
-
Dissection:
- Incise skin and subcutaneous tissue.
- The proper digital nerve and artery run together in the neurovascular bundle, volar to the midaxial line and dorsal to the flexor tendon sheath.
-
Carefully separate the neurovascular bundle from the surrounding soft tissues.

- Closure: Layered closure.
Metacarpal and Phalangeal Fracture Fixation
- Indication: Displaced or unstable fractures requiring open reduction and internal fixation (ORIF).
-
Incision:
- Metacarpals: Dorsal longitudinal incision between the metacarpals, or directly over the metacarpal shaft if superficial. For the first metacarpal, a dorsal incision centered over the bone is typical.
- Phalanges: Dorsal longitudinal incision or midaxial incision, depending on the fracture location and required exposure. Brunner's incisions are often employed for volar access.
-
Dissection:
- Dorsal Metacarpals/Phalanges: Incise skin and subcutaneous tissue. Retract extensor tendons. Access bone directly. Take care to preserve the thin overlying soft tissues and perforating vessels.
-
Volar Phalanges:
Utilize Brunner's zigzag incision. Carefully incise skin and subcutaneous tissue. Retract the neurovascular bundles laterally. The flexor tendon sheath and underlying tendons are then accessed.
-
Reduction & Fixation:
Achieve anatomical reduction and stabilize with appropriate implants (K-wires, screws, plates).


- Closure: Layered closure.
Palmar Fasciectomy (for Dupuytren's Contracture)
- Indication: Significant Dupuytren's contracture leading to functional impairment.
- Incision: Transverse or longitudinal incision, often multiple, or zigzag (Brunner) incisions, planned carefully to allow exposure of the diseased fascia while preserving neurovascular structures.
-
Dissection:
- Incise skin and subcutaneous tissue. Elevate skin flaps.
- Carefully identify and isolate the digital neurovascular bundles , which can be intimately involved with the diseased cords.
-
Excise the diseased palmar fascia, tracing the cords to their origins and insertions. Preserve healthy tissue.
- Closure: Skin closure, sometimes requiring skin grafts or local flaps for larger defects.
Complications & Management
Complications following forearm, wrist, and hand surgery, though infrequent with meticulous technique, can significantly impact patient outcomes. Prevention through careful planning and execution is paramount, and early recognition and appropriate management are crucial for salvage.
| Complication | Incidence (General) | Salvage Strategies / Management |
|---|---|---|
| Nerve Injury | 1-5% (sensory branches higher) | Careful dissection, intraoperative nerve monitoring. Repair if transected. Neurolysis for compression. Secondary nerve grafting/transfers. |
| Vascular Injury | <1% (rarely severe) | Direct repair, vein grafting. If unrecognized, can lead to compartment syndrome or tissue loss. |
| Infection | 1-5% (higher in open injuries) | Prophylactic antibiotics, meticulous asepsis. Debridement, irrigation, antibiotics. Culture-directed therapy. |
| Nonunion / Malunion | Variable (e.g., scaphoid 5-30%) | Revision surgery with bone grafting, stable fixation. Corrective osteotomy for symptomatic malunion. |
| Stiffness / Contracture | Common, variable degrees | Early supervised rehabilitation, splinting. Tenolysis, capsulotomy, arthrolysis if severe. |
| Scar Contracture | 5-10% (more with poor incision) | Appropriate incision planning (zigzag). Scar massage, silicone sheeting. Z-plasty, skin grafting for severe cases. |
| Complex Regional Pain Syndrome (CRPS) | 1-5% | Early recognition. Multimodal pain management, physical therapy, sympathetic blocks, psychological support. |
| Hardware Irritation | 5-15% (depending on implant) | Hardware removal after bone healing (typically >6-12 months post-op). |
| Tendon Adhesions/Rupture | 2-10% (flexor tendons higher) | Early mobilization protocols. Tenolysis. Tendon grafting/transfer for rupture. |
| Compartment Syndrome | Rare (acute injury/tight closure) | Immediate fasciotomy. |
Specific Considerations:
- Iatrogenic Nerve Injury: The most common nerve injuries involve sensory branches (e.g., superficial radial nerve, dorsal cutaneous branch of the ulnar nerve, palmar cutaneous branch of the median nerve), often during superficial dissection. Meticulous identification and protection are key.
- Hematoma Formation: Can lead to increased pressure, pain, and potentially compartment syndrome or compromise of neurovascular structures. Careful hemostasis and judicious use of drains are important.
- Wound Dehiscence/Necrosis: Risk increased with tension, poor vascularity, or infection. Requires careful wound management, sometimes secondary closure or skin grafting.
- Post-Traumatic Arthritis: A common long-term complication, especially after intra-articular fractures. Management ranges from conservative measures to arthrodesis or arthroplasty.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral component of the overall surgical management, aiming to restore function, minimize stiffness, and prevent complications. Protocols are highly specific to the surgical procedure, patient factors, and surgeon preference.
General Principles:
- Early Mobilization (when safe): Crucial to prevent stiffness and adhesion formation, especially for tendon repairs.
- Protection: Adequate immobilization (splints, casts) is necessary to protect healing structures (fractures, repairs).
- Pain Management: Effective analgesia facilitates participation in therapy.
- Edema Control: Elevation, compression, and gentle active range of motion help reduce swelling.
- Patient Education: Empowering the patient to understand and adhere to the protocol is vital.
Phases of Rehabilitation:
Phase I: Immobilization and Protection (0-4 weeks post-op)
- Goals: Protect surgical repair/fixation, control pain and edema, maintain motion in uninvolved joints.
-
Interventions:
- Immobilization: Custom splinting or casting in a position that offloads tension from repaired structures (e.g., wrist in slight extension for extensor tendon repair, wrist in slight flexion for flexor tendon repair, thumb in abduction for CMC arthroplasty).
- Edema Control: Elevation, gentle compression.
- Uninvolved Joints: Active and passive range of motion (ROM) for shoulder, elbow, and non-involved digits.
- Sensory Re-education: For nerve repairs, begin early protective sensation training.
Phase II: Controlled Mobilization (4-8 weeks post-op)
- Goals: Gradually increase ROM, improve tendon gliding, initiate gentle strengthening, continue edema and pain control.
-
Interventions:
- Gradual Weaning from Immobilization: Transition from static to dynamic splints or remove splints for specific exercise sessions.
- Active Range of Motion (AROM): Begin gentle, progressive AROM exercises, respecting tissue healing timelines.
- Passive Range of Motion (PROM): May be introduced cautiously, particularly for joint stiffness, under therapist supervision.
- Tendon Gliding Exercises: Specific exercises to promote differential gliding of flexor and extensor tendons.
- Light Strengthening: Isometric exercises or very light resistance can be introduced as appropriate.
- Scar Management: Massage, silicone products to minimize scar hypertrophy and adhesion.
Phase III: Progressive Strengthening and Functional Restoration (8-12+ weeks post-op)
- Goals: Maximize strength, endurance, dexterity, and return to functional activities.
-
Interventions:
- Progressive Resistance Exercises: Increase resistance and complexity of strengthening exercises.
- Advanced ROM: Continue stretching and mobilization to regain full motion.
- Fine Motor Dexterity: Practice tasks requiring precision and coordination.
- Work/Sport-Specific Training: Tailored exercises to prepare for return to vocational or recreational activities.
- Desensitization: For nerve injuries, progressive desensitization techniques.
- Functional Bracing/Splinting: May be used for protection during strenuous activities.
Specific Considerations for Common Procedures:
- Flexor Tendon Repair: Early protected passive motion (Duran protocol) or active motion (Kleinerts, Nottingham protocols) within specific ranges to prevent adhesion while protecting the repair. High compliance and skilled therapy are essential.
- Distal Radius Fractures (ORIF): Early AROM of digits, elbow, and shoulder. Wrist ROM begins around 2-4 weeks post-op, with progressive strengthening.
- Scaphoid Fracture Fixation: Immobilization is usually shorter than non-operative. Early digital ROM. Wrist ROM and strengthening generally begin 6-12 weeks post-op, once radiographic evidence of healing is present.
- Nerve Repair: Immobilization for 3 weeks to protect repair. Gradual AROM. Sensory re-education and desensitization are critical.
Summary of Key Literature / Guidelines
The body of literature guiding surgical approaches to the forearm, wrist, and hand is extensive, evolving, and often procedure-specific. However, several foundational principles and areas of ongoing research remain central.
- Anatomical Texts & Atlases: Standard surgical textbooks and anatomical atlases (e.g., Netter, Gray's Anatomy, Hoppenfeld's Surgical Exposures in Orthopaedics) are indispensable for understanding the precise relationships of structures and defining safe dissection planes. The concept of internervous planes , championed by Hoppenfeld, remains a cornerstone of orthopedic surgical technique to minimize iatrogenic injury.
- AO Principles: The AO Foundation's principles of fracture management (anatomical reduction, stable fixation, preservation of blood supply, early mobilization) are universally applied to osseous injuries of the forearm, wrist, and hand. Evidence supports these principles for optimizing outcomes in fractures like distal radius and scaphoid.
- Median Nerve Decompression (Carpal Tunnel Syndrome): The efficacy of open and endoscopic carpal tunnel release for medically refractory CTS is well-established. Long-term studies consistently demonstrate superior outcomes for surgery compared to conservative management in moderate-to-severe cases. Debates continue regarding the optimal incision type and the utility of endoscopic versus open techniques, though outcomes are generally comparable.
- Tendon Repair Protocols: Evidence-based rehabilitation protocols are critical for flexor tendon repairs, balancing the need for repair protection with early motion to prevent adhesions. Recent trends favor earlier controlled active motion protocols over purely passive approaches, demonstrating improved outcomes in appropriate patient populations with strict adherence to therapy.
- Scaphoid Nonunion: Management of scaphoid nonunion often involves open reduction and internal fixation with bone grafting. Studies highlight the importance of vascularized bone grafts, especially for proximal pole nonunions or those with avascular changes, to improve union rates.
- Dupuytren's Contracture: Surgical fasciectomy remains the gold standard for functionally limiting Dupuytren's contracture. The literature increasingly explores less invasive alternatives like needle aponeurotomy and collagenase injection, demonstrating comparable short-term efficacy for specific contracture types, though recurrence rates may differ.
- Ligamentous Instability: Advances in understanding carpal kinematics and ligamentous anatomy have refined approaches to wrist instability, particularly scapholunate dissociation. Direct repair, reconstruction with local tissues, and capsulodesis procedures are employed, with ongoing research comparing long-term outcomes of various techniques.
- Functional Outcomes Measures: The use of standardized patient-reported outcome measures (PROMs) such as the Disabilities of the Arm, Shoulder and Hand (DASH) score or Michigan Hand Outcomes Questionnaire (MHQ) is increasingly advocated to objectively assess the effectiveness of surgical interventions and guide clinical decision-making and research.
Clinical & Radiographic Imaging

You Might Also Like