Considering METHA Short Stem? Discover Bone-Preserving THA

Key Takeaway
Discover the latest medical recommendations for Considering METHA Short Stem? Discover Bone-Preserving THA. The **metha short stem** is a modular, metaphyseal anchoring, and proximally loading implant for total hip arthroplasty. Based on the Mayo hip, it offers a bone and soft tissue preserving option for young, active patients with disabling hip arthritis. This physiological design reduces thigh pain and is easily revisable, serving as a bridge between resurfacing and standard cementless stems.
Introduction and Epidemiology
Short stem designs offer a conservative, bone- and soft-tissue-preserving option for total hip arthroplasty (THA), specifically indicated for young and active patients presenting with disabling hip arthritis. The demographic profile of patients undergoing THA has shifted significantly over the past two decades, with a marked increase in procedures performed on patients under the age of 60. This epidemiological shift necessitates implants that not only provide excellent survivorship and functional outcomes but also preserve proximal femoral bone stock to facilitate inevitable future revision arthroplasties.
The conceptual framework of neck-preserving total hip arthroplasty is largely credited to Michael Freeman. Similar tissue-sparing concepts were proposed by Leo Whiteside and Townley, who advocated for neck preservation utilizing conventional stems. Whiteside et al., in a landmark cadaveric study, demonstrated that the preservation of a minimum of 50% of the femoral neck significantly enhances the resistance to torsional forces in proximally fixed stems.

Furthermore, Jasty et al., through a canine in vivo study evaluating proximal fitting stems with polished distal segments, revealed that while the diaphyseal component provides essential initial mechanical stability, it is largely redundant for long-term implant stability once proximal osteointegration is achieved. This biomechanical revelation catalyzed the development and refinement of short metaphyseal anchoring stems.

Short, neck-preserving stems have demonstrated clinical efficacy since 1985, with the Mayo conservative hip (pioneered by Bernard F. Morrey) establishing an excellent long-term track record. However, the taxonomy of short stems is heterogeneous. Current classifications encompass five distinct design philosophies: stems inspired by the Mayo hip (e.g., METHA, ESKA, NANOS); short, bulky, non-neck-preserving stems (e.g., Proxima); neck-preserving curved stems (e.g., CFP by Pipino); shortened tapered stems (e.g., Taperlock Microplasty, Trilock); and epiphyseal "neck pods" (e.g., BMHR and Silent hip).

The clinical utility of short stems in THA has historically been scrutinized, primarily through comparisons with hip resurfacing arthroplasty (HRA) and modern cementless tapered femoral stems that utilize proximal load transfer. While HRA is inherently bone-preserving on the femoral side, it requires extensive soft tissue dissection, negating the principles of soft-tissue preservation. Furthermore, HRA is inextricably linked to metal-on-metal (MoM) articulations, precipitating complications such as hypersensitivity, aseptic lymphocyte-dominated vasculitis-associated lesions (ALVAL), and systemic elevation of serum metal ions.

Conversely, while modern tapered stems with metaphyseal loading have documented success, short metaphyseal-fixing implants offer superior preservation of the femoral diaphysis, facilitate minimally invasive surgical (MIS) approaches, and accommodate a diverse array of tribological couplings. By providing proximal loading that mitigates stress shielding and minimizes the incidence of thigh pain, short metaphyseal loading implants act as an optimal bridge between HRA and standard cementless stems. The METHA stem, a modular short stem predicated on the Mayo hip philosophy, epitomizes this evolution by combining modular construction, metaphyseal anchoring, proximal load transfer, minimal stem volume, and circumferential osteoconductive coating.

Surgical Anatomy and Biomechanics
Proximal Femoral Osteology and Metaphyseal Architecture
A profound understanding of proximal femoral anatomy is paramount for the successful implantation of short-stem prostheses. The proximal femur is characterized by a complex trabecular network designed to transmit multi-planar forces from the hip joint to the femoral diaphysis. The primary compressive trabeculae extend from the superior femoral head to the medial calcar, while the secondary tensile trabeculae arc from the fovea to the lateral cortex below the greater trochanter. Short stems like the METHA are engineered to engage this metaphyseal cancellous bone, relying on the structural integrity of the calcar femorale and the lateral cortical wall for primary stability.

The Dorr classification of proximal femoral morphology plays a critical role in patient selection for short stems. Dorr Type A (champagne flute) and Type B (normal) femurs exhibit robust metaphyseal cancellous bone and thick cortical bone, providing an ideal biomechanical envelope for metaphyseal-engaging implants. Conversely, Dorr Type C (stovepipe) femurs, characterized by cortical thinning and metaphyseal cancellous depletion, compromise the initial press-fit stability required for short stems, increasing the risk of early subsidence.

Biomechanics of Proximal Load Transfer
Conventional diaphyseal-engaging cementless stems often bypass the metaphyseal bone, transferring loads distally. According to Wolff’s Law, this distal load transfer results in proximal stress shielding, leading to progressive calcar resorption and loss of proximal bone stock over time. The biomechanical rationale of the METHA short stem is to restore physiological load transmission. By anchoring exclusively within the metaphysis and preserving the femoral neck, the stem facilitates direct compressive loading onto the calcar and lateral cortex.

The preservation of the femoral neck ring is biomechanically advantageous. It acts as a closed structural loop that resists torsional forces, which are particularly high during activities of daily living such as stair climbing and rising from a seated position. The METHA stem utilizes a rounded, tapered geometry that engages the preserved cortical ring of the femoral neck, converting shear forces into compressive forces, thereby enhancing initial stability and promoting robust secondary osteointegration.

Implant Metallurgy and Modularity
The METHA stem is manufactured from a high-strength titanium alloy (Ti6Al4V), which possesses a modulus of elasticity closer to that of cortical bone compared to cobalt-chromium alloys, further mitigating stress shielding. The surface is typically treated with a circumferential microporous titanium plasma spray, often augmented with a calcium phosphate or hydroxyapatite coating to accelerate bone ongrowth and ingrowth.

A defining feature of the METHA system is its modular neck adapters. This modularity allows the surgeon to independently adjust femoral offset, leg length, and version without altering the fixation of the stem within the metaphysis. By decoupling stem fixation from joint kinematics, the surgeon can accurately restore the patient's native center of rotation, optimizing abductor mechanics and reducing the risk of impingement and dislocation.

Indications and Contraindications
The selection criteria for short-stem THA must be rigorous to ensure optimal outcomes. The ideal candidate is a young, active patient with good bone quality who requires arthroplasty for end-stage joint disease. Careful assessment of preoperative radiographs and bone morphology is mandatory.

Table of Indications and Contraindications
| Parameter | Favorable Indications for Short Stem (METHA) | Contraindications (Consider Standard THA) |
|---|---|---|
| Patient Age and Activity | Age < 65 years, high functional demand | Elderly, low demand, institutionalized |
| Bone Morphology | Dorr Type A or Type B | Dorr Type C (Stovepipe), severe osteopenia |
| Pathology | Primary Osteoarthritis, AVN (Ficat I-III) | AVN with massive metaphyseal cysts, active infection |
| Anatomy | Normal anatomy, mild dysplasia (Crowe I) | Severe dysplasia (Crowe III/IV), severe coxa vara/valga |
| Previous Surgery | No prior proximal femoral hardware | Retained hardware, prior intertrochanteric osteotomy |
| Femoral Neck | Intact, sufficient length for osteotomy | Resorbed neck, basicervical fracture |

Nuances in Patient Selection
Avascular necrosis (AVN) presents a specific challenge. While short stems are indicated for early-stage AVN, the surgeon must carefully evaluate the extent of the necrotic lesion on preoperative MRI or CT. If the cystic changes or necrotic bone extend distally into the metaphysis, the primary stability of a short stem will be compromised, necessitating the use of a standard diaphyseal-engaging stem.

Similarly, in cases of developmental dysplasia of the hip (DDH), short stems can be highly effective in Crowe Type I and occasionally Type II dysplastic hips, provided the metaphyseal envelope can accommodate the implant. However, in severe dysplasia with extreme anteversion or an excessively narrow medullary canal, the modularity of the METHA stem may not be sufficient to overcome the anatomical distortion, and a custom or modular standard stem may be required.

Pre Operative Planning and Patient Positioning
Radiographic Assessment and Templating
Meticulous preoperative planning is the cornerstone of successful short-stem arthroplasty. Standard weight-bearing anteroposterior (AP) pelvic radiographs and cross-table lateral views of the affected hip are required. Digital templating software, calibrated with a radiographic marker, should be utilized to assess leg length discrepancy, femoral offset, and the center of rotation.

Templating for a METHA stem differs significantly from standard stems. The primary objective is to determine the optimal level and angle of the femoral neck osteotomy. The osteotomy is typically planned higher than in conventional THA, often preserving the base of the femoral neck to provide a cortical ring for the implant to rest against. The template should demonstrate the stem filling the metaphyseal region, with the lateral flare of the implant abutting the lateral endosteal cortex and the medial curve resting congruently against the calcar.
Restoring Biomechanics
The surgeon must evaluate the native femoral offset and neck-shaft angle. Because the METHA stem relies on modular neck adapters, the templating phase involves selecting the appropriate stem size for metaphyseal fill and subsequently superimposing various modular neck options to reconstruct the native center of rotation. Anticipating the required neck adapter (e.g., standard, high offset, varus, or valgus) ensures that the surgeon is prepared to restore soft tissue tension intraoperatively.

Patient Positioning and Surgical Approach Compatibility
The METHA stem is highly compatible with minimally invasive surgical (MIS) approaches due to its reduced length and curved trajectory, which does not require extensive clearance into the femoral diaphysis.

For the Direct Anterior Approach (DAA), the patient is positioned supine on a standard or specialized traction table. The DAA utilizes the internervous plane between the tensor fasciae latae (superior gluteal nerve) and the sartorius (femoral nerve). The short stem is particularly advantageous in the DAA, as it minimizes the need for extreme femoral elevation and soft tissue releases typically required to broach and insert a standard straight stem.

If utilizing a Minimally Invasive Posterior Approach, the patient is placed in the lateral decubitus position. The approach involves splitting the gluteus maximus and detaching the short external rotators. The short stem facilitates easier insertion without impinging on the abductor musculature or requiring excessive anterior capsular release.

Detailed Surgical Approach and Technique
Exposure and Capsulotomy
Following the selected surgical approach, meticulous hemostasis and careful soft tissue handling are maintained. A comprehensive capsulotomy or capsulectomy is performed to expose the femoral head and neck. In tissue-sparing approaches, a capsular release must be sufficient to allow adequate mobilization of the proximal femur without applying excessive traction, which could result in intraoperative fractures.

The Femoral Neck Osteotomy
The femoral neck osteotomy is the most critical step in short-stem THA. Unlike standard stems where the cut is often made at the base of the neck, the METHA stem requires a higher, more horizontal resection. The osteotomy is typically initiated 1.0 to 1.5 cm proximal to the lesser trochanter, angling towards the superior aspect of the base of the femoral neck.

Preserving the lateral aspect of the femoral neck and the greater trochanteric bed is vital, as the stem relies on three-point fixation within the metaphysis: the medial calcar, the lateral cortex, and the anterior/posterior cortices of the preserved neck. An oscillating saw is used to make the precise cut, and the femoral head is subsequently removed using a corkscrew.

Acetabular Preparation
Acetabular preparation follows standard arthroplasty principles. The labrum is excised, and the acetabulum is reamed to hemispherical bleeding subchondral bone. A press-fit cementless acetabular component is impacted into place, targeting 40 degrees of inclination and 15-20 degrees of anteversion. The appropriate bearing surface (highly cross-linked polyethylene or ceramic) is seated.
Femoral Preparation and Broaching
The proximal femur is mobilized to allow direct access to the medullary canal. A box osteotome or a specialized curved awl is used to open the femoral canal laterally, ensuring the trajectory aligns with the lateral cortex to prevent varus malalignment.

Broaching is performed using specialized compaction broaches that preserve metaphyseal cancellous bone. The broaches are sequentially impacted, following the natural curve of the medial calcar. The surgeon must pay strict attention to rotational alignment during broaching, allowing the broach to seek its natural anteversion dictated by the preserved femoral neck anatomy. Broaching is complete when axial and rotational stability are achieved, and the broach sits flush with the osteotomy level.

Trialing and Modularity Assessment
With the final broach in situ, the modular trial neck is attached. The METHA system provides various neck adapters differing in CCD angle (e.g., 130°, 135°, 140°) and offset. A trial femoral head is placed, and the hip is reduced.

The surgeon assesses leg length, tissue tension, and stability through a full range of motion. The shuck test and impingement checks (in flexion/internal rotation and extension/external rotation) are performed. The modularity of the neck allows for fine-tuning of the biomechanics without requiring the extraction of the broach or altering the metaphyseal fit.

Final Implantation
Once the optimal neck and head configuration is determined, the hip is dislocated, and the trial components are removed. The definitive METHA stem is introduced into the canal. Due to the compaction broaching technique, the definitive stem (which is slightly oversized compared to the broach to ensure a press-fit) is impacted until it achieves absolute rotational and axial stability.

The selected modular neck adapter is then engaged into the stem's morse taper. The taper must be clean and dry before impaction to prevent micromotion or cold welding failure. The definitive femoral head is applied, and the hip is finally reduced. A final check of stability and leg length is conducted before meticulous layered closure of the soft tissues.
Complications and Management
While short-stem THA offers numerous biomechanical advantages, it is associated with specific intraoperative and postoperative complications that require astute surgical management. The learning curve for short stems is primarily centered around the high neck osteotomy and the avoidance of varus malalignment.
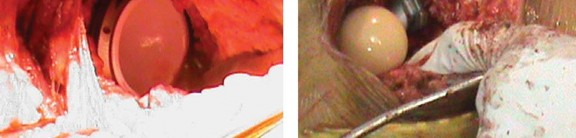
Table of Complications and Salvage Strategies
| Complication | Incidence / Risk Factors | Prevention and Management Strategy |
|---|---|---|
| Intraoperative Calcar Fracture | 1-3%. Associated with undersized osteotomy, aggressive broaching, or Dorr A bone. | Prevention: Careful lateralization of the starting point. Management: Prophylactic or therapeutic cerclage wiring around the lesser trochanter; bypass with standard stem if unstable. |
| Early Subsidence | 2-5%. Risk higher in Dorr C bone, osteopenia, or undersized stems. | Prevention: Strict patient selection; ensure rigid press-fit intraoperatively. Management: If progressive >5mm or symptomatic, revise to standard diaphyseal stem. |
| Varus Malalignment | 3-6%. Caused by medial starting point or failure to clear lateral neck. | Prevention: Aggressive lateral preparation with box chisel. Management: Accept if stable and asymptomatic; revise if associated with loosening or impingement. |
| Thigh Pain | <1% (Significantly lower than standard cementless stems). | Prevention: Avoid distal point loading by ensuring excellent metaphyseal fit. Management: Conservative management; rule out aseptic loosening or infection. |
| Aseptic Loosening | Rare (<2% at 10 years). Failure of osteointegration. | Prevention: Avoid thermal necrosis during bone prep; ensure initial mechanical stability. Management: Revision arthroplasty with standard or revision stem. |

Managing Intraoperative Challenges
The most critical intraoperative complication is a fracture of the calcar femorale during broaching or stem impaction. Because short stems rely heavily on the proximal cortical ring, a calcar crack compromises primary stability. If a non-displaced crack is identified, a cerclage wire should be passed immediately below the lesser trochanter to stabilize the hoop stresses. If the fracture propagates distally or destabilizes the stem, the surgeon must abandon the short
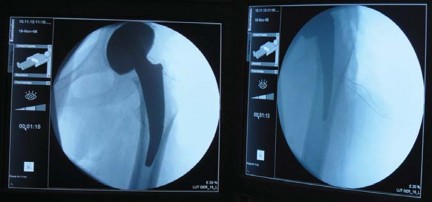
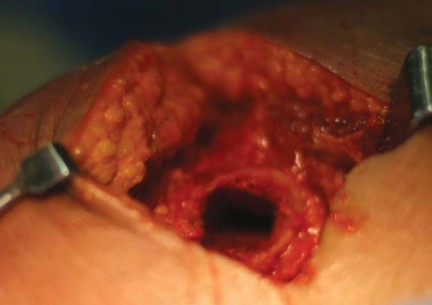
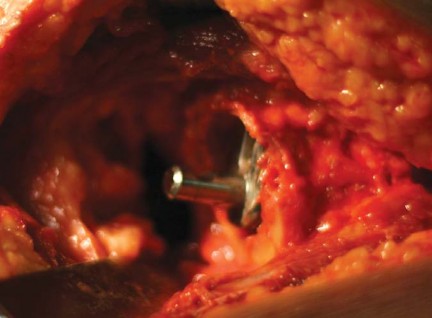
Clinical & Radiographic Imaging














You Might Also Like


