Solving Snapping Scapula: Is resection of the superomedial your option?

Key Takeaway
Here are the crucial details you must know about Solving Snapping Scapula: Is resection of the superomedial your option?. Scapulothoracic crepitus, or snapping scapula syndrome, is painful scapular motion with crepitus due to incongruence or maltracking in the scapulothoracic articulation. This often involves irritation of bursae or osseous anomalies, especially near the superior or superomedial angle of the scapula. Treatment, when conservative measures fail, may involve surgical procedures like resection of the superomedial portion to alleviate impingement.
Introduction and Epidemiology
Scapulothoracic crepitus, initially described by Boinet in 1867, represents a complex clinical entity characterized by painful scapular motion and associated crepitus during scapulothoracic articulation. This condition manifests with or without a definitive history of acute trauma and is frequently encountered in overhead athletes, laborers, and active individuals subjected to repetitive upper extremity biomechanical stress.
Often referred to in the literature under various synonyms—including scapulothoracic bursitis, retroscapular creaking, superior scapular syndrome, retroscapular pain, washboard syndrome, and rattling of the shoulder blade—snapping scapula syndrome remains a diagnostic and therapeutic challenge. The hallmark of the syndrome is the tactile-acoustic phenomenon described by Milch and Burman. This crepitus is generated secondary to an abnormality in the scapulothoracic interval and is traditionally divided into three classes based on the volume and character of the sound produced.
Epidemiologically, snapping scapula syndrome is most prevalent in young, active patients, particularly those involved in sports requiring repetitive overhead motion, such as baseball, swimming, and gymnastics. The etiology is generally multifactorial, encompassing osseous abnormalities, soft tissue variations, and dynamic neuromuscular imbalances leading to scapular dyskinesis. While primary osseous lesions like osteochondromas or rib exostoses are classic causes, the vast majority of cases are secondary to chronic microtrauma, resulting in fibrotic changes within the periscapular bursae and subsequent impingement of the superomedial angle of the scapula against the posterior thoracic wall.
Surgical Anatomy and Biomechanics
A rigorous understanding of periscapular anatomy is mandatory for the surgical management of snapping scapula syndrome, particularly when considering resection of the superomedial angle. The scapulothoracic articulation is not a true diarthrodial joint; rather, it is a complex myofascial interface between the concave anterior aspect of the scapula and the convex posterior thoracic cage.
Osseous Morphology
The osseous anatomy of the scapula exhibits significant inter-individual variability. The mean superomedial angle of the scapula is estimated to range between 139 and 154 degrees, with the average thickness of the superior pole measuring 3.4 to 3.9 mm. A prominent superomedial angle, sometimes referred to as Luschka’s tubercle, significantly increases the risk of mechanical impingement against the underlying ribs during scapular protraction and retraction.
Muscular and Fascial Layers
The scapulothoracic articulation is cushioned by several critical muscle bellies. The subscapularis covers the anterior surface of the scapula, while the serratus anterior features a broad origin on the anterolateral chest wall and inserts along the ventral surface of the medial scapular border.
A distinct "bare area" devoid of muscular attachments exists between the origins of the subscapularis and serratus anterior. Averaging 22.3 × 10.8 mm, this region has been heavily implicated as a primary locus for pathologic scapulothoracic impingement and subsequent bursal hypertrophy.
Bursal Anatomy
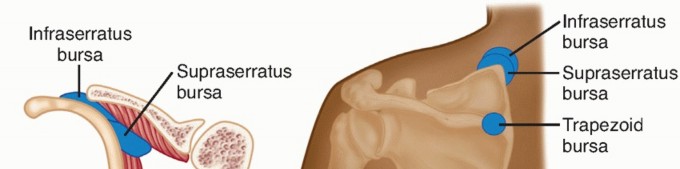
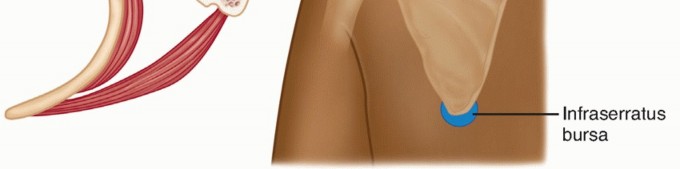
The smooth gliding of the scapula over the thorax is facilitated by a complex bursal network. Anatomical studies consistently identify two major and four minor bursae within this articulation.
The two major bursae are:
1. Infraserratus Bursa: Located between the serratus anterior muscle and the posterolateral chest wall.
2. Supraserratus Bursa: Situated between the serratus anterior and the subscapularis muscles.
The four minor bursae are distributed as follows:
* Two at the superomedial angle of the scapula.
* One at the inferior angle of the scapula.
* One at the medial base of the scapular spine, underlying the trapezius muscle.
Pathologic thickening, fibrotic scarring, or inflammation of these bursae—particularly the supraserratus and superomedial minor bursae—directly correlates with the symptomatic tactile-acoustic crepitus observed clinically.
Neurovascular Considerations
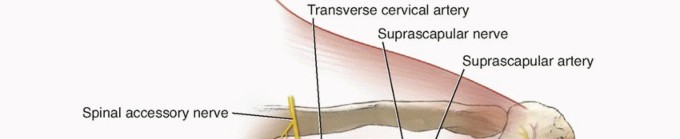
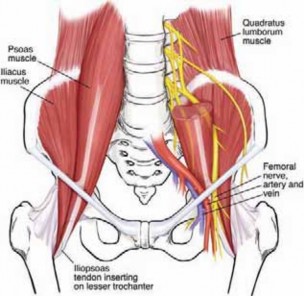
Surgical intervention in this region demands meticulous respect for the regional neurovascular structures. The spinal accessory nerve (Cranial Nerve XI) courses obliquely across the posterior triangle of the neck and descends deep to the trapezius, lateral to the medial border of the scapula. More critically for superomedial angle resection, the dorsal scapular nerve (DSN) and the descending branch of the transverse cervical artery course parallel and medial to the medial border of the scapula, deep to the rhomboids. Iatrogenic injury to the DSN results in rhomboid and levator scapulae paralysis, leading to profound lateral scapular winging.
Indications and Contraindications
The management of snapping scapula syndrome strictly follows a stepwise algorithm, prioritizing conservative modalities before considering surgical intervention. Operative management, specifically bursectomy with or without superomedial angle resection, is reserved for recalcitrant cases or those with distinct structural pathology.
| Clinical Scenario | Operative Indication | Non Operative Indication |
|---|---|---|
| Duration of Symptoms | Refractory to >6 months of targeted conservative therapy | Symptoms present for <6 months |
| Osseous Pathology | Symptomatic osteochondroma, rib exostosis, or malunion | Normal osseous morphology or asymptomatic incidentalomas |
| Response to Injections | Transient relief from diagnostic/therapeutic bursal injections | Sustained relief from corticosteroid injections |
| Neuromuscular Status | Intact periscapular innervation with structural impingement | Primary scapular winging due to long thoracic or DSN palsy |
| Patient Compliance | High adherence to preoperative physical therapy | Poor compliance with rehabilitation protocols |
Contraindications
Absolute contraindications to surgical resection include active local or systemic infection, primary neurogenic scapular winging (e.g., long thoracic nerve palsy), and cervical radiculopathy mimicking scapulothoracic pain. Relative contraindications include poorly controlled psychiatric comorbidities, chronic pain syndromes (e.g., fibromyalgia) without a clear structural etiology, and failure to engage in preoperative periscapular rehabilitation.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical to differentiating true structural snapping scapula from secondary scapular dyskinesis.
Clinical Evaluation and Diagnostic Injections
The physical examination must evaluate scapulohumeral rhythm, assessing for dyskinesis, pseudo-winging, or compensatory kinematics. Palpation of the medial border and superomedial angle during active and passive shoulder elevation often localizes the crepitus. A diagnostic local anesthetic injection (e.g., 10 mL of 1% lidocaine) directed into the supraserratus or infraserratus bursa under ultrasound guidance is highly predictive of surgical success. Complete, albeit temporary, resolution of pain confirms the scapulothoracic articulation as the primary pain generator.
Advanced Imaging Modalities
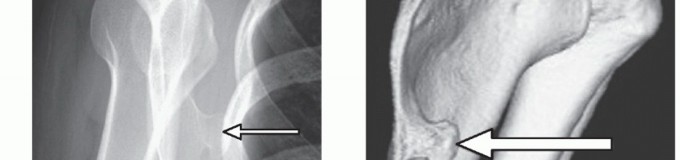
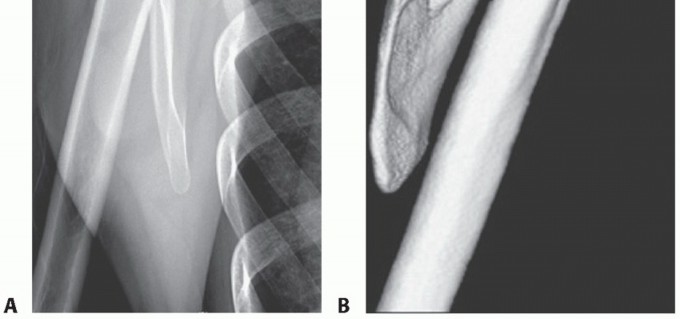
While standard anteroposterior and scapular Y radiographs can rule out gross abnormalities, advanced cross-sectional imaging is mandatory for surgical planning.

Computed Tomography (CT) with 3D volumetric reconstruction is the gold standard for evaluating the osseous morphology of the superomedial angle. It precisely delineates the anterior curvature of the scapula, identifies osteochondromas, and assesses thoracic cage congruency.

Magnetic Resonance Imaging (MRI), particularly T2-weighted and STIR sequences, is indispensable for evaluating soft tissue pathology. MRI effectively demonstrates bursal fluid, synovial hypertrophy, fibrotic masses, and soft tissue tumors (e.g., elastofibroma dorsi) that may be responsible for the mechanical snapping.
Patient Positioning
For both arthroscopic and open surgical approaches, the patient is typically placed in the prone position. General anesthesia is administered, and the patient is carefully padded to prevent pressure necrosis.
The operative arm is draped free and placed in the "chicken wing" position—internal rotation with the dorsum of the hand resting on the lumbar spine. This maneuver allows the scapula to lift away from the posterior thoracic wall, maximizing the scapulothoracic interval and facilitating access to the superomedial angle and underlying bursae. Alternatively, some surgeons prefer the lateral decubitus position, though prone positioning generally offers superior ergonomic access to the medial scapular border.
Detailed Surgical Approach and Technique
The surgical management of snapping scapula syndrome has evolved significantly. While the open approach remains a reliable workhorse, particularly for large osseous lesions, endoscopic (arthroscopic) scapulothoracic bursectomy and partial scapulectomy have become the standard of care due to decreased morbidity, minimized muscle detachment, and accelerated rehabilitation.
Endoscopic Scapulothoracic Approach
The endoscopic approach requires meticulous portal placement to avoid the dorsal scapular nerve and artery.
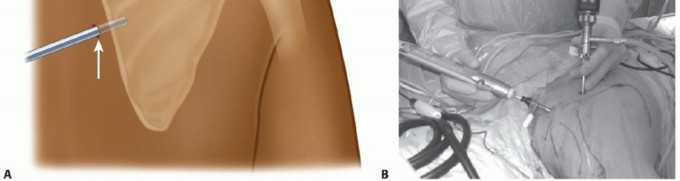
Portal Placement
Standard portals include a superior and an inferior medial portal. These are typically established 3 cm medial to the medial border of the scapula. The inferior portal is created first, positioned just proximal to the inferior angle. A trocar is introduced bluntly through the trapezius and rhomboid major muscles, entering the scapulothoracic space. The superior portal is then established under direct visualization, approximately 3 to 4 cm distal to the superomedial angle.

Diagnostic Endoscopy and Bursectomy
Upon entering the scapulothoracic interval, a thorough diagnostic endoscopy is performed. The space is often obscured by hypertrophic bursal tissue and fibrofatty connective tissue.

A radiofrequency ablation wand and an oscillating shaver are utilized to perform a radical bursectomy. The supraserratus and infraserratus bursae are systematically cleared. It is critical to maintain the shaver blades facing the ventral surface of the scapula to prevent iatrogenic injury to the thoracic cage, pleura, or intercostal neurovascular bundles.
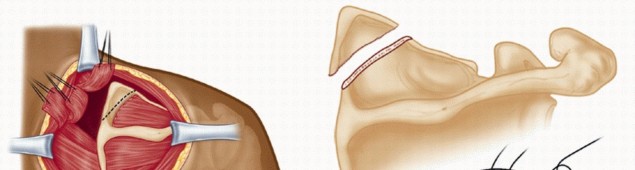
Superomedial Angle Resection
Once the ventral surface of the scapula is skeletonized and the superomedial angle is clearly identified, osseous resection commences.

An arthroscopic acromionizer or high-speed motorized burr is introduced. The resection targets the prominent superomedial angle, aiming to remove the bony impingement while preserving the structural integrity of the scapular spine.
Typically, a triangular wedge of bone measuring 2 to 3 cm at its base is resected. The levator scapulae insertion at the superomedial angle is partially detached during this process. The resection is carried down to bleeding cancellous bone, ensuring a smooth, contoured surface that will no longer abut the thoracic cage during scapular excursion. Fluoroscopy may be utilized intraoperatively to confirm the adequacy of the osseous resection.
Open Surgical Approach
The open approach is primarily indicated for massive osteochondromas, complex revision cases, or instances where endoscopic visualization is compromised by severe scarring.

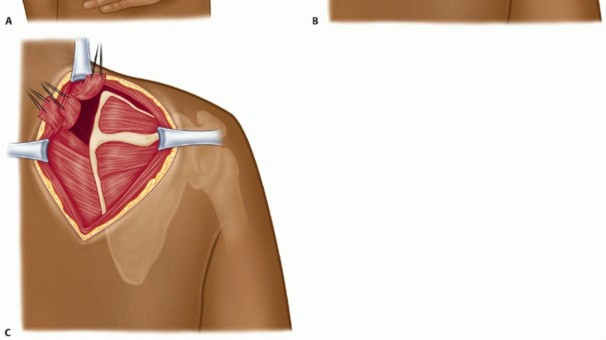
Incision and Dissection
A longitudinal incision is made parallel to the medial border of the scapula, centered over the superomedial angle. The subcutaneous tissues are divided to expose the trapezius fascia. The trapezius muscle fibers are either split longitudinally in line with their fibers or mobilized laterally depending on the extent of exposure required.

Deep to the trapezius, the insertions of the rhomboid minor and levator scapulae are identified. These muscles are carefully tagged and detached from the medial border of the scapula using electrocautery. Subperiosteal dissection is then performed along the ventral surface of the scapula to expose the supraserratus bursa and the superomedial angle.
Osseous Resection and Closure
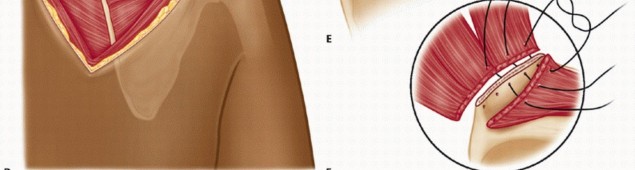
With the superomedial angle fully exposed, an oscillating saw or large rongeur is used to resect the prominent bone.

The resected edges are smoothed with a rasp or burr. The underlying bursal tissue is excised en bloc. Following copious irrigation and hemostasis, the detached levator scapulae and rhomboid minor muscles are securely reattached to the scapular border using transosseous suture equivalents or suture anchors. Meticulous layered closure is essential to prevent dead space and subsequent hematoma formation.
Complications and Management
Surgical intervention for snapping scapula syndrome, while generally successful, carries a distinct complication profile. The close proximity of critical neurovascular structures and the highly vascular nature of the periscapular musculature necessitate rigorous surgical technique.
| Complication | Estimated Incidence | Etiology and Mechanism | Prevention and Salvage Strategy |
|---|---|---|---|
| Hematoma / Seroma | 5% - 10% | Highly vascular muscle beds; inadequate hemostasis | Liberal use of electrocautery; closed suction drains in open cases; compressive dressings |
| Dorsal Scapular Nerve Injury | 1% - 3% | Errant portal placement; aggressive medial dissection | Keep portals >3 cm medial to the scapular border; avoid blind plunging with trocars |
| Incomplete Resection | 3% - 5% | Failure to adequately resect the superomedial angle | Intraoperative fluoroscopy; thorough 3D CT preoperative planning |
| Iatrogenic Scapular Winging | <2% | Failure of muscle reattachment (open) or nerve injury | Secure transosseous repair of rhomboids/levator; meticulous nerve protection |
| Pneumothorax | <1% | Violation of the pleural cavity during bursectomy | Direct shaver blades strictly toward the ventral scapula; avoid deep thoracic penetration |
Neurovascular and Soft Tissue Complications
Hematoma formation is the most frequently encountered postoperative complication, particularly in open procedures where extensive muscle detachment occurs.
If a large, symptomatic hematoma develops, it may require operative evacuation to prevent secondary infection or excessive fibrosis. Nerve injury, specifically to the dorsal scapular nerve, is a devastating complication.

Injury to this nerve results in denervation of the rhomboids and levator scapulae, leading to profound lateral scapular winging and significant functional deficit. Management of established nerve injuries is complex, often requiring prolonged conservative management, nerve exploration, or eventual dynamic muscle transfers (e.g., Eden-Lange procedure) if recovery does not occur.
Post Oper
Clinical & Radiographic Imaging



You Might Also Like