Achondroplasia Orthopedic MCQs - Arab Board Exam Prep

Achondroplasia Orthopedic MCQs - Arab Board Exam Prep
A couple with normal stature has a child diagnosed with achondroplasia. They are concerned about the genetics of this condition and ask about the likelihood of this occurring. Based on the epidemiology of achondroplasia, what is the most accurate genetic explanation?
Correct Answer: De novo mutation of a gene on chromosome 4
Achondroplasia is inherited in an autosomal dominant manner. However, over 80% of individuals with achondroplasia have parents with normal stature. In these cases, the condition is the result of a 'de novo' (new) mutation of a gene localized to the distal short arm of chromosome 4.
Review the AP and lateral radiographs of the lumbar spine in this patient with short-limb dwarfism. Which of the following is the characteristic radiographic finding shown?
Correct Answer: Interpediculate distance decreases from the upper to lower lumbar spine
The provided radiograph demonstrates the classic spinal findings in achondroplasia. The interpediculate distance abnormally decreases from the upper to the lower lumbar spine (AP view), and characteristic short pedicles are seen on the lateral view, which predisposes these patients to spinal stenosis.
A 4-year-old boy presents with delayed motor milestones and the facial features shown below. What is the most likely diagnosis?

Correct Answer: Achondroplasia
The clinical image shows a child with a head that is disproportionately large in relation to height, a prominent forehead (frontal bossing), and a broadened, depressed nasal bridge. These are the hallmark craniofacial features of achondroplasia, the most common human chondrodysplasia.
A patient with the most common human chondrodysplasia presents for orthopedic evaluation. Based on the clinical photograph provided, which combination of physical findings is most characteristic of this condition?
Correct Answer: Exaggerated lumbar lordosis, limitation of elbow extension, and genu varum
As seen in the clinical image and described in the text, patients with achondroplasia typically present with exaggerated lumbar lordosis, limitation of elbow extension and rotation, and genu varum. Hyperextension of the knees and most other joints is also common.
An infant is diagnosed with achondroplasia shortly after birth. The parents are counseled regarding potential life-threatening complications during infancy. Which of the following represents the greatest risk of mortality in this age group?
Correct Answer: Spinal cord compression and upper airway obstruction
In infancy, patients with achondroplasia are at an increased risk of death primarily due to compression of the spinal cord (often at the foramen magnum) and upper airway obstruction.
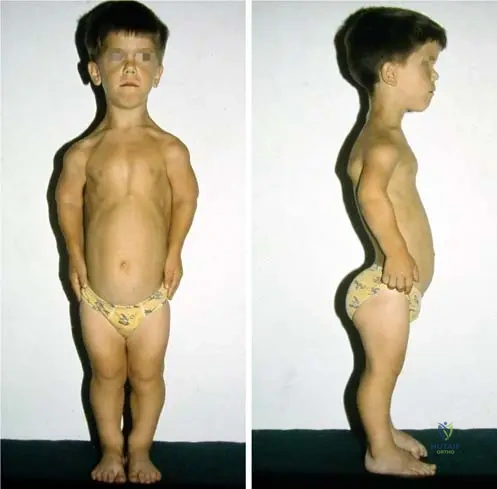
The image below compares a patient with a specific skeletal dysplasia to an age-matched individual of normal stature. Which of the following statements accurately describes the anthropometric differences seen in this condition?
Correct Answer: There is no difference in trunk height, but the chest and shoulders are narrower
Achondroplasia is a disproportionate short-limb dwarfism. As demonstrated in the comparative clinical image, there is no significant difference in the height of the trunk between an achondroplastic patient and a normal individual; however, the chest and shoulders are notably narrower.
A 12-month-old infant with achondroplasia is brought to the clinic. The parents are concerned because the child is not yet walking and seems 'floppy.' Which of the following is the most appropriate counseling regarding the child's development?
Correct Answer: Hypotonia and delayed motor milestones are typical, but intelligence is usually normal
In infancy, hypotonia is typical in achondroplasia, and the acquisition of developmental motor milestones is often delayed. However, intelligence and life span are usually normal, and parents should be reassured regarding cognitive development.
A 10-year-old girl with achondroplasia asks about her expected final adult height. According to established growth data for this condition, what is the mean adult height for females?
Correct Answer: 124 cm
According to the clinical data for achondroplasia, the mean adult height in males is 131 ± 5.6 cm, and in females, it is 124 ± 5.9 cm.
The clinical photograph below shows the hands of a patient with achondroplasia. Which of the following statements best describes the hand manifestations in this specific dysplasia compared to other short-limb dwarfisms?

Correct Answer: The fingers are not as short as in many other short-limb dwarfisms
As shown in the clinical image and noted in the text, the fingers in achondroplasia are not as short as in many other forms of short-limb dwarfism. They often present with a 'trident' appearance, though their relative length is better preserved than in other severe dysplasias.
Achondroplasia is caused by a mutation that affects endochondral ossification. The responsible gene is localized to which of the following chromosomal regions?
Correct Answer: Distal short arm of chromosome 4
Achondroplasia is the result of a mutation of a gene (FGFR3) localized to the distal short arm of chromosome 4. This mutation leads to a gain of function that inhibits chondrocyte proliferation, resulting in disproportionate short-limb dwarfism.
A 5-year-old boy with short stature presents for evaluation. An AP and lateral radiograph of the lumbar spine is shown below. What is the characteristic radiographic finding demonstrated in this condition?
Correct Answer: Decrease in interpediculate distance from upper to lower lumbar spine
In achondroplasia, a hallmark radiographic finding is the narrowing of the interpediculate distance from the upper to the lower lumbar spine, which is the opposite of the normal widening seen in unaffected individuals. Short pedicles are also characteristically seen on the lateral view.
A child presents with the facial features shown below. Which of the following genetic mutations is most likely responsible for this phenotype?
Correct Answer: Mutation on the distal short arm of chromosome 4
The clinical image demonstrates a disproportionately large head, prominent forehead, and a broadened, depressed nasal bridge typical of achondroplasia. This condition is caused by a mutation localized to the distal short arm of chromosome 4 (specifically the FGFR3 gene).
A patient with the condition shown below presents to the clinic. Which of the following joint findings is typically associated with this disorder?
Correct Answer: Limitation of elbow extension and rotation
Patients with achondroplasia typically exhibit exaggerated lumbar lordosis, genu varum, hyperextension of the knees and most other joints, but characteristically have a limitation of elbow extension and rotation.
A couple with normal stature has a child diagnosed with achondroplasia. They are concerned about the risk of having another child with the same condition. What percentage of achondroplasia cases are the result of a de novo mutation in parents with normal stature?
Correct Answer: Over 80%
Over 80% of individuals with achondroplasia have parents with normal stature. In these cases, the condition is the result of a spontaneous 'de novo' mutation.
An infant is diagnosed with achondroplasia. Which of the following is a typical finding during the first year of life in this patient population?
Correct Answer: Hypotonia and delayed motor milestones
In infancy, patients with achondroplasia typically present with hypotonia, and the acquisition of developmental motor milestones is often delayed. Intelligence and overall life span are usually normal.
While life span in achondroplasia is usually normal, there is an increased risk of death in infancy. Which of the following is a primary cause for this increased mortality risk?
Correct Answer: Upper airway obstruction and spinal cord compression
Compression of the spinal cord (often at the foramen magnum) and upper airway obstruction are critical complications in infants with achondroplasia that significantly increase the risk of death during infancy.
A 12-year-old boy with achondroplasia is compared to his unaffected peer. Based on the clinical appearance shown below, which of the following statements regarding his trunk and chest is accurate?

Correct Answer: The chest and shoulders are narrower compared to an unaffected peer.
In achondroplasia, there is no significant difference in the height of the trunk compared to unaffected individuals; however, the chest and shoulders are characteristically narrower.
A family asks about the expected adult height for their male child recently diagnosed with achondroplasia. According to standard growth data for this condition, what is the mean adult height for males?
Correct Answer: 131 +/- 5.6 cm
The mean adult height in males with achondroplasia is 131 +/- 5.6 cm, whereas in females it is 124 +/- 5.9 cm.
The hands of a patient with a skeletal dysplasia are shown below. In achondroplasia, how do the fingers typically present compared to many other short-limb dwarfisms?
Correct Answer: They are not as short as in many other short-limb dwarfisms.
While achondroplasia is a short-limb dwarfism, the fingers are characteristically not as short as those seen in many other forms of short-limb dwarfism.
A 25-year-old male with achondroplasia is planning to start a family with a female of normal stature. What is the inheritance pattern of his condition, and what is the risk of passing the mutation to his offspring?
Correct Answer: Autosomal dominant; 50% risk
Achondroplasia is inherited in an autosomal dominant manner. An affected individual has a 50% chance of passing the mutated gene to each offspring, regardless of the child's sex.
A 12-year-old boy with disproportionate short stature presents with back pain. The AP and lateral radiographs of the lumbar spine are shown below. Which of the following is the characteristic radiographic finding demonstrated in this condition?
Correct Answer: Decreasing interpediculate distance from L1 to L5
In achondroplasia, the interpediculate distance characteristically decreases from the upper to the lower lumbar spine, which is the opposite of the normal spine where it widens. This, combined with short pedicles seen on the lateral view, contributes to the high risk of spinal stenosis in these patients.
A couple with normal stature has a child diagnosed with achondroplasia. They are concerned about the risk of having another child with the same condition. What is the most likely genetic mechanism responsible for their child's condition?
Correct Answer: De novo mutation on the distal short arm of chromosome 4
Achondroplasia is inherited in an autosomal dominant manner. However, over 80% of individuals with achondroplasia have parents with normal stature, meaning the condition is the result of a 'de novo' (new) mutation. This gene is localized to the distal short arm of chromosome 4 (FGFR3 gene).
A 5-year-old child presents to the orthopedic clinic. Clinical photographs are shown below. Examination of the upper extremities in this patient is most likely to reveal which of the following findings?
Correct Answer: Limitation of elbow extension and rotation
The clinical images demonstrate a patient with achondroplasia, characterized by exaggerated lumbar lordosis and genu varum. A classic upper extremity finding in these patients is the limitation of elbow extension and rotation, despite hyperextension being common in most other joints like the knees.
An infant is diagnosed with the most common form of human chondrodysplasia. While life span is generally normal, there is an increased risk of death in infancy. Which of the following is the primary cause of this increased mortality risk?
Correct Answer: Compression of the spinal cord and upper airway obstruction
In achondroplasia, intelligence and life span are usually normal. However, compression of the spinal cord (often at the foramen magnum) and upper airway obstruction significantly increase the risk of death during infancy.
A 3-year-old boy is evaluated for delayed motor milestones. His clinical appearance is shown below. Which of the following best describes the craniofacial characteristics associated with this syndrome?
Correct Answer: Disproportionately large head, prominent forehead, and depressed nasal bridge
The image shows the classic facial features of achondroplasia. The head is disproportionately large in relation to height (macrocephaly), the forehead is prominent (frontal bossing), and the nasal bridge is broadened and depressed.
A pediatrician refers a 9-month-old infant with achondroplasia to the orthopedic clinic due to concerns about delayed motor milestones. The parents are highly anxious about the child's future cognitive development. What is the most appropriate counseling to provide regarding this child's developmental trajectory?
Correct Answer: Motor delays are typical due to hypotonia, but intelligence is usually normal.
In infancy, hypotonia is typical in achondroplasia, and the acquisition of developmental motor milestones is often delayed as a result. However, intelligence and overall life span are usually normal.
The hands of a patient with a disproportionate short-limb dwarfism are shown below. According to the specific characteristics of this condition, how do these digits typically compare to other forms of short-limb dwarfism?
Correct Answer: They are not as short as in many other short-limb dwarfisms.
While achondroplasia is a short-limb dwarfism and features a characteristic 'trident hand' deformity, the fingers themselves are actually not as short as those seen in many other forms of short-limb dwarfism.
A 10-year-old female with achondroplasia and her parents are inquiring about her expected final adult height. Based on epidemiological data for this condition, what is the mean adult height for females?
Correct Answer: 124 cm
In achondroplasia, the mean adult height in males is 131 +/- 5.6 cm, and in females, it is 124 +/- 5.9 cm.
A clinical comparison between a patient with achondroplasia and an age-matched individual of normal stature is shown below. Which of the following statements accurately describes the axial skeletal proportions in the affected individual?
Correct Answer: There is no difference in trunk height, but the chest and shoulders are narrower.
Achondroplasia is a disproportionate short-limb dwarfism. As demonstrated in the clinical comparison, there is no significant difference in the height of the trunk between an achondroplastic patient and a normal individual; however, the chest and shoulders are notably narrower in achondroplasia.
A 45-year-old male with achondroplasia presents with neurogenic claudication. Radiographic evaluation of his lumbar spine is performed. Which of the following anatomical abnormalities of the vertebrae is most responsible for his spinal stenosis?
Correct Answer: Characteristic short pedicles
Spinal stenosis is a hallmark complication of achondroplasia in adulthood. It is primarily driven by the characteristic short pedicles (seen on lateral radiographs) and the decreasing interpediculate distance in the lumbar spine, which severely narrows the spinal canal.
A 5-year-old boy with disproportionate short stature presents for evaluation. The AP and lateral radiographs of the lumbar spine are shown below. Which of the following best describes the classic radiographic finding seen in the AP view of this condition?
Correct Answer: The interpedicular distance decreases from L1 to L5.
In achondroplasia, a hallmark radiographic finding on the AP view of the spine is the narrowing of the interpedicular distance from the upper to the lower lumbar spine (L1 to L5). In a normal spine, this distance widens caudally. Anterior beaking is more characteristic of mucopolysaccharidoses (like Morquio or Hurler syndrome), and severe platyspondyly is seen in conditions like thanatophoric dysplasia or spondyloepiphyseal dysplasia.
A 3-year-old child presents with the facial features shown in the clinical photograph below. Which of the following genetic mechanisms is most likely responsible for this patient's condition?
Correct Answer: De novo mutation of a gene on the distal short arm of chromosome 4.
The clinical image shows a child with a disproportionately large head, prominent forehead (frontal bossing), and a broadened, depressed nasal bridge, which are classic facial features of achondroplasia. Achondroplasia is caused by a mutation in the FGFR3 gene, localized to the distal short arm of chromosome 4. Over 80% of cases are the result of a de novo (new) mutation in individuals with parents of normal stature.
In infants diagnosed with the most common human chondrodysplasia, which of the following complications poses the greatest risk of mortality during the first year of life?
Correct Answer: Cervicomedullary compression and upper airway obstruction.
Achondroplasia is the most common chondrodysplasia. In infancy, compression of the spinal cord (specifically cervicomedullary compression at the narrowed foramen magnum) and upper airway obstruction significantly increase the risk of sudden death. Atlantoaxial instability is more characteristic of Down syndrome or Morquio syndrome, while a bell-shaped thorax causing severe restrictive lung disease is classic for asphyxiating thoracic dystrophy (Jeune syndrome) or thanatophoric dysplasia.
A 7-year-old patient presents with the clinical posture and lower extremity alignment shown below. Upon physical examination of the upper extremities, which of the following findings is most commonly associated with this syndrome?
Correct Answer: Limitation of elbow extension and rotation.
The image demonstrates exaggerated lumbar lordosis, genu varum, and hyperextension of the knees, typical of achondroplasia. While many joints in achondroplasia exhibit hyperextensibility (like the knees), the elbow is a notable exception. Limitation of elbow extension and rotation is a very common and classic clinical finding in patients with achondroplasia.
A couple with normal stature brings their newborn child to the orthopedic clinic. The child has been diagnosed with achondroplasia. The parents are concerned about the risk of having another child with the same condition. What is the most accurate counseling regarding the etiology of their child's condition?
Correct Answer: It is the result of a de novo mutation in over 80% of cases, making the recurrence risk for this couple very low.
Achondroplasia is inherited in an autosomal dominant manner. However, over 80% of individuals with achondroplasia have parents with normal stature. In these cases, the condition is the result of a spontaneous 'de novo' mutation. Therefore, the recurrence risk for parents of normal stature who have one affected child is extremely low (though slightly higher than the general population due to the rare possibility of germline mosaicism).
The clinical photograph below demonstrates the hands of a patient with the most common disproportionate short-limb dwarfism. Which of the following statements regarding the hand anatomy in this condition is true?
Correct Answer: The fingers are not as short as in many other short-limb dwarfisms.
In achondroplasia, the hands often exhibit a 'trident' appearance due to the inability to approximate the tips of the middle and ring fingers. However, as noted in the clinical description, the fingers in achondroplasia are actually not as short as they are in many other forms of short-limb dwarfism. Syndactyly is characteristic of Apert syndrome, and triphalangeal thumbs are seen in conditions like Holt-Oram syndrome.
A 12-month-old infant with achondroplasia is brought to the clinic by his parents, who are concerned that he is not yet walking or pulling to stand. Which of the following is the most appropriate response regarding his development?
Correct Answer: This is likely due to typical infantile hypotonia, and motor milestones are often delayed, though intelligence is usually normal.
In infancy, patients with achondroplasia typically present with hypotonia. As a result, the acquisition of developmental motor milestones (such as sitting, standing, and walking) is often delayed. However, their intelligence and life span are usually normal. While spinal cord compression is a risk, delayed motor milestones alone in a 12-month-old are expected due to hypotonia and altered biomechanics, not necessarily an acute cord compression.
The clinical photograph compares a patient with achondroplasia (left) to an age-matched child with normal stature (right). Based on the typical anthropometric features of this condition, which of the following statements is correct regarding the patient's torso?
Correct Answer: The trunk height is similar to the normal child, but the chest and shoulders are narrower.
Achondroplasia is a disproportionate short-limb dwarfism. The shortening primarily affects the appendicular skeleton (rhizomelic shortening). As demonstrated in the clinical image, there is no significant difference in the height of the trunk between an achondroplastic patient and a normal-statured peer; however, the chest and shoulders are characteristically narrower in achondroplasia.
An 18-year-old male with achondroplasia presents for a final growth evaluation. According to standard growth curves for this specific skeletal dysplasia, what is the expected mean adult height for males?
Correct Answer: 131 cm
In achondroplasia, the mean adult height for males is approximately 131 +/- 5.6 cm. For females, the mean adult height is slightly lower, at approximately 124 +/- 5.9 cm.
Review the lateral lumbar spine radiograph of the patient shown below. The characteristic anatomical abnormality seen on this view directly predisposes the patient to which of the following clinical conditions in adulthood?
Correct Answer: Lumbar spinal stenosis.
The lateral radiograph demonstrates characteristically short pedicles. Combined with the decreased interpedicular distance seen on the AP view, these short pedicles result in a congenitally narrow spinal canal. In adulthood, even mild degenerative changes (such as disc bulging or facet hypertrophy) can precipitate severe symptomatic lumbar spinal stenosis, which is a hallmark complication of achondroplasia.
A 5-year-old boy with disproportionate short stature presents for evaluation. An anteroposterior and lateral radiograph of the lumbar spine is obtained, as shown below. Which of the following is the hallmark radiographic finding in the lumbar spine for this condition?
Correct Answer: Interpediculate distance decreases from upper to lower lumbar spine
In achondroplasia, a classic radiographic feature is that the interpediculate distance decreases from the upper to the lower lumbar spine, which is the opposite of the normal spine. Additionally, characteristic short pedicles are seen on the lateral view, contributing to spinal stenosis.
A couple with normal stature has a child diagnosed with achondroplasia. They are concerned about the risk in future pregnancies and ask how this occurred. What is the most accurate statement regarding the genetics of this condition in their child?
Correct Answer: It represents a de novo mutation in over 80% of such cases
Achondroplasia is inherited in an autosomal dominant manner. However, over 80% of individuals with achondroplasia have parents with normal stature, meaning the condition is the result of a 'de novo' (new) mutation.
A 3-year-old child presents to the orthopedic clinic. Based on the clinical photograph below, which of the following craniofacial features is characteristic of this patient's underlying skeletal dysplasia?
Correct Answer: Disproportionately large head with a prominent forehead and depressed nasal bridge
As seen in the provided clinical image and described in the text, patients with achondroplasia typically have a head that is disproportionately large in relation to their height, a prominent forehead (frontal bossing), and a broadened, depressed nasal bridge.
While evaluating an infant with achondroplasia, the orthopedic surgeon must be vigilant about potential life-threatening complications. Which of the following conditions significantly increases the risk of death during infancy in these patients?
Correct Answer: Upper airway obstruction and spinal cord compression
According to the clinical text, compression of the spinal cord (often at the foramen magnum) and upper airway obstruction are the primary factors that increase the risk of death in infancy for patients with achondroplasia.
A 12-year-old boy with achondroplasia presents for a routine follow-up. The clinical photograph below demonstrates his typical standing posture. Which combination of physical findings is most consistent with this condition?
Correct Answer: Exaggerated lumbar lordosis, limitation of elbow extension, and genu varum
The clinical image and text highlight that exaggerated lumbar lordosis, limitation of elbow extension and rotation, genu varum, and hyperextension of the knees and most other joints are common findings in achondroplasia.
Achondroplasia is the most common of the human chondrodysplasias. The genetic mutation responsible for this condition is localized to which of the following chromosomal regions?
Correct Answer: Distal short arm of chromosome 4
Achondroplasia is caused by a mutation in the FGFR3 gene, which is localized to the distal short arm of chromosome 4.
A pediatrician refers a 9-month-old infant with achondroplasia to the orthopedic clinic due to concerns about delayed walking and poor head control. What is the typical developmental and cognitive profile for a child with this condition?
Correct Answer: Hypotonia and delayed motor milestones with normal intelligence
In infancy, hypotonia is typical in achondroplasia, and the acquisition of developmental motor milestones is often delayed. However, intelligence and life span are usually normal.
A clinical photograph of the hands of a patient with a skeletal dysplasia is shown below. In the context of achondroplasia, how do the fingers typically present compared to many other short-limb dwarfisms?
Correct Answer: They are not as short as in many other short-limb dwarfisms
As noted in the text accompanying the clinical image, the fingers in achondroplasia are not as short as in many other forms of short-limb dwarfism, often presenting with a characteristic 'trident' appearance (though the relative length is the key distinguishing feature mentioned).
A 14-year-old male with achondroplasia asks about his expected final adult height. According to established growth data for this condition, what is the mean adult height for males?
Correct Answer: 131 +/- 5.6 cm
The mean adult height in males with achondroplasia is 131 +/- 5.6 cm, whereas in females it is 124 +/- 5.9 cm.
Two individuals are shown in the clinical photograph below. The patient on the right has achondroplasia. When comparing the trunk and shoulder dimensions of a patient with achondroplasia to an individual of normal stature, which of the following statements is most accurate?
Correct Answer: There is no difference in trunk height, but the chest and shoulders are narrower
Achondroplasia is a disproportionate short-limb dwarfism. As demonstrated in the clinical comparison image, there is no difference between the patients in the height of the trunk; however, the chest and shoulders are narrower in achondroplasia.
When evaluating an AP pelvis radiograph of a child with achondroplasia, which constellation of findings is most characteristic?
A patient with achondroplasia demonstrates a classic hand deformity. Which of the following describes the typical hand appearance in these patients?
What is the characteristic finding of the lumbar pedicles in achondroplasia?
What is the primary underlying mechanical cause of genu varum in patients with this condition?
None
