Enhance Anterior Shoulder Surgery: Crucial Joint Applied Surgical Anatomy

Key Takeaway
This topic focuses on Enhance Anterior Shoulder Surgery: Crucial Joint Applied Surgical Anatomy, Joint applied surgical anatomy of the anterior shoulder approach focuses on the deltoid (outer sleeve) and rotator cuff (inner sleeve: supraspinatus, infraspinatus, teres minor, subscapularis). Access involves reflecting the deltoid laterally and incising the subscapularis. Muscles attached to the coracoid process, a key landmark, require medial retraction for exposure.
Comprehensive Introduction and Patho-Epidemiology
The anterior approach to the shoulder, classically recognized in the orthopedic literature as the deltopectoral approach, remains the fundamental workhorse incision in reconstructive and traumatological shoulder surgery. First popularized in the mid-20th century by pioneers such as Charles Neer, this approach provides highly extensile, unparalleled access to the glenohumeral joint, the proximal humerus, and the anterior articular structures. Crucially, it achieves this comprehensive exposure without denervating the primary muscular stabilizers of the shoulder girdle, a biomechanical imperative for postoperative recovery. Its clinical utility spans a vast spectrum of orthopedic pathology, including complex proximal humerus fracture fixation, anatomic total shoulder arthroplasty (aTSA), reverse total shoulder arthroplasty (rTSA), and anterior stabilization procedures such as the Latarjet coracoid transfer.

Epidemiologically, the demand for surgical interventions utilizing the anterior approach has surged at an unprecedented rate over the past two decades. Proximal humerus fractures now account for approximately 5% to 6% of all adult fractures, presenting with an exponentially increasing incidence in the aging, osteoporotic demographic. This fragility fracture burden necessitates surgical strategies that can navigate compromised bone stock while preserving the delicate vascular supply to the humeral head. Furthermore, the volume of shoulder arthroplasty has grown significantly, outpacing the growth rates of both hip and knee arthroplasty in several international joint registries. Recent epidemiological data indicates a massive paradigm shift toward rTSA, particularly for patients presenting with rotator cuff tear arthropathy, massive irreparable cuff tears, and severe glenohumeral osteoarthritis with concurrent posterior subluxation (Walch B2/B3 and C glenoids).
Understanding the applied surgical anatomy of this region is not merely an academic exercise but a critical prerequisite for executing these complex reconstructions safely. The transition from historically constrained prosthetic designs to modern modular, convertible, and reverse geometry systems relies heavily on the structural integrity of the deltoid and the remaining rotator cuff musculature. Consequently, the surgical approach must prioritize the absolute preservation of these dynamic stabilizers. The deltopectoral interval, functioning as a true internervous plane, allows for profound exposure while completely mitigating the risk of iatrogenic denervation, cementing its status as the gold standard approach for the vast majority of reconstructive shoulder procedures.

The evolution of shoulder arthroplasty and fracture management has necessitated a significantly more nuanced understanding of the anterior shoulder's soft tissue envelope. Surgeons must now account for the three-dimensional interplay between the osseous architecture and the capsuloligamentous constraints. Failure to respect these anatomical boundaries during the anterior approach invariably leads to suboptimal component positioning, neurovascular morbidity, and catastrophic biomechanical failure. Therefore, a meticulous, layer-by-layer comprehension of the anterior shoulder—from the superficial dermal landmarks down to the glenoid vault—is mandatory for any surgeon undertaking these procedures.
Detailed Surgical Anatomy and Biomechanics
Mastery of the anterior shoulder approach requires a profound, three-dimensional understanding of the musculotendinous sleeves, the internervous planes, and the intimate relationship between the osseous landmarks and critical neurovascular structures. The surgeon must visualize the shoulder not as isolated components, but as a complex, dynamic organ system where every fascial release and muscular retraction alters the global biomechanical environment.
Superficial Landmarks and The Outer Muscular Sleeve
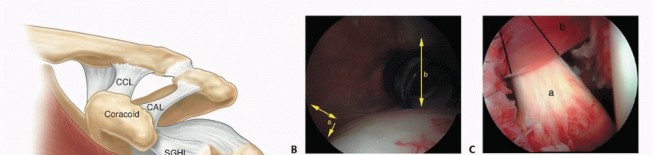
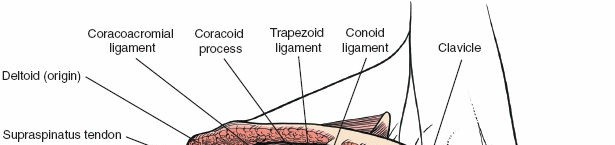
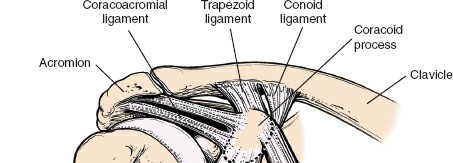
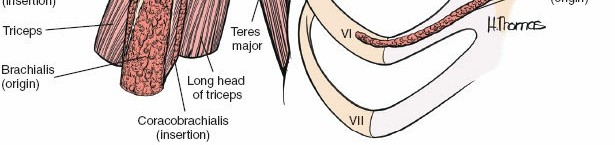
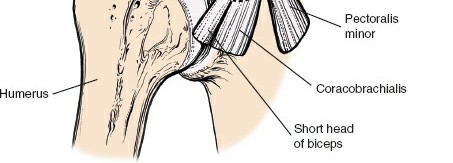
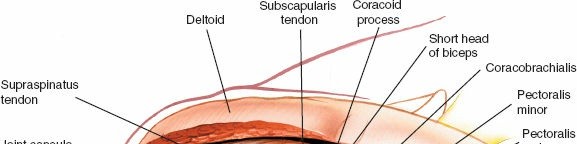
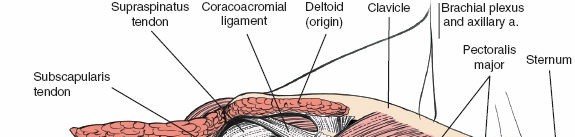
The surgical landmarks dictate the trajectory of the approach and serve as the initial orienting beacons for the surgeon. The coracoid process of the scapula is undeniably the most critical palpable bony protuberance in the anterior shoulder. Located at the superior aspect of the deltopectoral groove, it serves as the "lighthouse of the shoulder." The tip of the coracoid projects anteriorly, laterally, and inferiorly, providing a reliable guide to the underlying glenohumeral joint. It serves as the origin for the conjoint tendon (comprising the short head of the biceps brachii and the coracobrachialis) and the insertion site for the pectoralis minor, making it a critical hub of musculotendinous convergence.
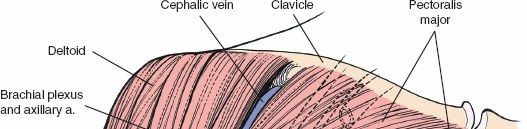
The outer muscular sleeve consists of the deltoid and the pectoralis major muscles, which together form the superficial boundaries of the surgical field. The deltoid muscle, a massive multipennate structure, originates from the lateral third of the clavicle, the acromion, and the scapular spine, converging to insert onto the deltoid tuberosity of the lateral humerus. It is exclusively innervated by the axillary nerve, making its preservation paramount for postoperative arm elevation. The pectoralis major, comprising distinct clavicular and sternal heads, inserts onto the lateral lip of the bicipital groove and is innervated by the medial and lateral pectoral nerves.
The deltopectoral approach brilliantly exploits the internervous plane between these two massive muscles. Because the deltoid is supplied by the axillary nerve (arising from the posterior cord of the brachial plexus) and the pectoralis major by the pectoral nerves (arising from the medial and lateral cords), separating these muscles longitudinally does not denervate either structure. The cephalic vein consistently marks this interval, running within the deltopectoral groove and draining superiorly into the clavipectoral triangle before piercing the clavipectoral fascia to join the axillary vein. Management of the cephalic vein—whether retracted laterally with the deltoid to preserve its major tributaries or medially with the pectoralis—is a critical early step in the approach.
The Inner Muscular Sleeve and Dynamic Stabilizers
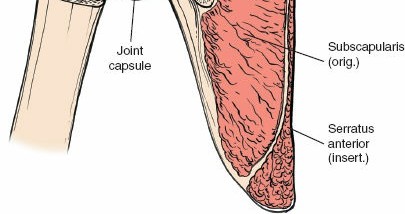
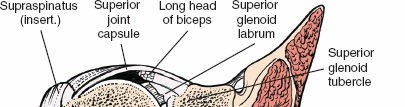
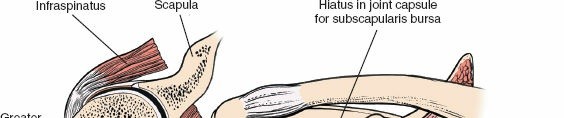
Deep to the deltopectoral interval lies the inner muscular sleeve, primarily composed of the rotator cuff and the underlying capsuloligamentous complex. The rotator cuff consists of four distinct muscles: the supraspinatus, infraspinatus, teres minor, and subscapularis. In the context of the anterior approach, the subscapularis is the most critical structure, acting as the primary anterior barrier to the glenohumeral joint.
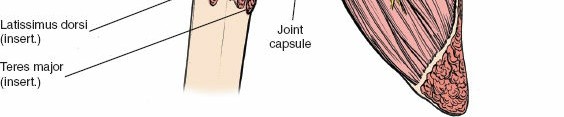
Originating from the expansive subscapular fossa of the anterior scapula, the subscapularis inserts broadly onto the lesser tuberosity of the humerus and blends intimately with the anterior joint capsule. It is innervated by the upper and lower subscapular nerves (branches of the posterior cord). The superior border of the subscapularis is demarcated by the rotator interval, a triangular capsular region bordered superiorly by the anterior margin of the supraspinatus, inferiorly by the superior margin of the subscapularis, and medially by the base of the coracoid process.


The rotator interval is a complex anatomical space containing the long head of the biceps tendon (LHBT), the coracohumeral ligament (CHL), and the superior glenohumeral ligament (SGHL). Dissection through the rotator interval is often the key to unlocking the anterior shoulder, allowing for mobilization of the subscapularis and identification of the intra-articular biceps tendon. Pathological contracture of the structures within the rotator interval, particularly the CHL, is a hallmark of adhesive capsulitis and requires meticulous surgical release to restore external rotation.
Neurovascular Structures in the Anterior Approach
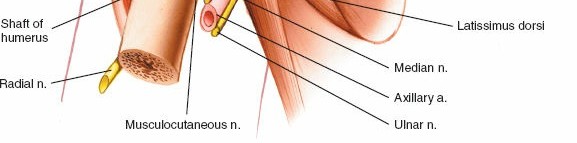
Surgical navigation of the anterior shoulder mandates precise identification, respect, and protection of several critical neurovascular structures that traverse the operative field. The musculocutaneous nerve typically enters the medial aspect of the coracobrachialis approximately 3 to 8 centimeters distal to the tip of the coracoid process. However, profound anatomical variants exist where the nerve penetrates the muscle much more proximally, sometimes within 1 centimeter of the coracoid. This places the nerve at significant risk of traction neurapraxia or direct transection during aggressive medial retraction of the conjoint tendon, particularly during procedures like the Latarjet or revision arthroplasty.
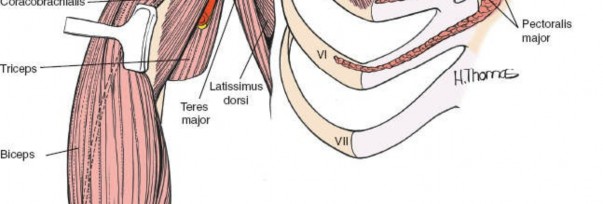
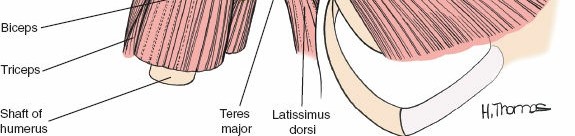
The axillary nerve is another structure of paramount concern, representing the most frequently injured nerve in anterior shoulder surgery. After branching from the posterior cord, it traverses anterior to the inferior border of the subscapularis before diving posteriorly through the quadrangular space. This space is bounded by the teres minor superiorly, the teres major inferiorly, the long head of the triceps medially, and the surgical neck of the humerus laterally. During inferior capsular release—a mandatory step for mobilizing the humerus in arthroplasty—the axillary nerve is highly vulnerable as it courses intimately close to the inferior capsule, often lying within millimeters of the inferior glenoid rim.


The anterior circumflex humeral artery (ACHA) and its accompanying paired veins (classically referred to by surgeons as the "three sisters") run horizontally across the inferior border of the subscapularis muscle. These vessels mark the inferior extent of the subscapularis and the superior border of the latissimus dorsi tendon. Ligation or meticulous electrocauterization of these vessels is a standard procedural step to prevent obscuring hemorrhage during deep dissection, capsular release, and subscapularis mobilization. Failure to secure these vessels can lead to significant postoperative hematoma formation and subsequent complications.
Biomechanics of the Anterior Shoulder
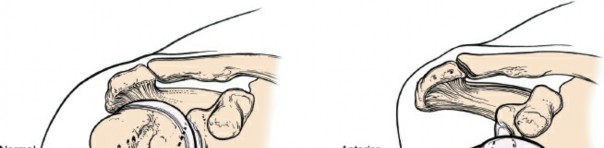
The glenohumeral joint is characterized biomechanically by a profound mismatch in articular surface area between the large, spherical humeral head and the shallow, pear-shaped glenoid fossa. This evolutionary design prioritizes global mobility and spatial positioning of the hand over intrinsic osseous stability. Static stability is conferred by the glenoid labrum, a fibrocartilaginous ring that deepens the glenoid socket by approximately 50%, and the complex arrangement of the glenohumeral ligaments (superior, middle, and inferior) which act as check-reins at the extremes of motion.
Dynamic stability, however, is primarily governed by the "concavity compression" mechanism orchestrated by the rotator cuff force couples. In the transverse plane, the anteriorly situated subscapularis balances the posteriorly situated infraspinatus and teres minor. These muscles simultaneously contract to compress the humeral head directly into the center of the glenoid concavity throughout the arc of motion. Disruption of the subscapularis during the anterior approach fundamentally alters this force couple.


Therefore, meticulous repair and postoperative protection of the subscapularis are absolutely critical to preventing anterior humeral subluxation and optimizing the kinematics of the reconstructed joint. In the setting of reverse shoulder arthroplasty, the biomechanical paradigm is shifted entirely; the center of rotation is medialized and distalized, tensioning the deltoid to act as the primary elevator while relying less on the native rotator cuff force couples. Nevertheless, preserving the anterior structures when possible continues to play a role in rotational stability and the prevention of prosthetic dislocation.
Exhaustive Indications and Contraindications
The deltopectoral approach is highly versatile, providing exceptional, extensile access for a wide array of glenohumeral and proximal humeral pathologies. The decision to utilize this approach versus alternative exposures (such as the anterolateral deltoid-splitting approach, the superior approach, or the posterior approach) depends heavily on the specific pathology, the required visualization of the glenoid face, and the absolute necessity of preserving the deltoid origin to maintain postoperative elevation.
Primary indications for the deltopectoral approach encompass almost the entirety of reconstructive shoulder surgery. It is the approach of choice for anatomic total shoulder arthroplasty (aTSA) and reverse total shoulder arthroplasty (rTSA), allowing for direct, orthogonal preparation of the glenoid vault. It is equally essential for hemiarthroplasty and the open reduction and internal fixation (ORIF) of complex proximal humerus fractures, particularly 3- and 4-part fractures where visualization of the medial calcar and the tuberosities is required. Furthermore, open anterior stabilization procedures, including the Latarjet procedure and open Bankart repairs, rely exclusively on this anatomic window.

Contraindications are generally relative but require careful preoperative consideration. Isolated posterior glenoid pathology, such as a posterior bony Bankart lesion or isolated posterior glenoid wear without anterior subluxation, is exceedingly difficult to address from the front and is better served by a posterior approach. Isolated greater tuberosity fractures, particularly those displaced superiorly and posteriorly, are often better addressed via a direct lateral deltoid-splitting approach, which provides direct access to the fracture bed without the need for extensive anterior soft tissue dissection.
Furthermore, in cases of severe proximal humerus malunions where the greater tuberosity has migrated significantly posterior and consolidated, the anterior approach may struggle to provide adequate orthogonal access for mobilization and reduction. In certain complex revision arthroplasty scenarios where extensive posterior capsular release or posterior osseous reconstruction is mandated, an extensile posterior approach or a combined approach may be warranted to safely extract components and reconstruct the joint line.
Comprehensive Summary of Indications and Pathways
| Pathology Category | Operative Indications via Anterior Approach | Non-Operative or Alternative Approach Indications |
|---|---|---|
| Glenohumeral Osteoarthritis | Intact rotator cuff (aTSA); eccentric wear with retroversion >15 degrees requiring structural grafting or augmented baseplates. | Mild/moderate OA manageable with injections/PT; severe posterior wear requiring posterior approach (rare). |
| Rotator Cuff Tear Arthropathy | Pseudoparalysis, severe superior migration of humeral head (rTSA); massive irreparable anterior/superior tears. | Medically unfit patients; isolated massive posterior tears without arthritis (may require superior capsular reconstruction or tendon transfer). |
| Proximal Humerus Fractures | 3- and 4-part fractures; head-splitting fractures; fracture-dislocations; valgus impacted fractures requiring elevation. | Non-displaced fractures; isolated greater tuberosity fractures (anterolateral approach preferred). |
| Anterior Instability | Recurrent instability with significant glenoid bone loss >15-20% (Latarjet); failed arthroscopic stabilization; HAGL lesions. | First-time dislocators without structural bone loss; engaging Hill-Sachs lesions (arthroscopic remplissage). |
| Infection / Revision | Two-stage exchange arthroplasty; component extraction; periprosthetic fractures requiring stem bypass. | Suppressive antibiotic therapy in non-surgical candidates; isolated posterior component failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough, exhaustive preoperative planning is paramount to executing the anterior approach effectively, anticipating intraoperative challenges, and ensuring precise execution of the surgical objective. The tolerance for error in modern shoulder arthroplasty and complex fracture fixation is exceedingly low, mandating a rigorous preoperative protocol that integrates advanced imaging, three-dimensional templating, and optimal patient positioning.


Advanced Imaging and Three-Dimensional Templating
Standard radiographic evaluation must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. The axillary view is absolutely non-negotiable, as it provides critical, foundational information regarding glenohumeral subluxation, static glenoid version, and the presence of anterior or posterior bone loss. Without a high-quality axillary radiograph, the surgeon is operating blind regarding the spatial relationship of the humeral head to the glenoid face.
For arthroplasty and complex fracture management, a fine-cut, non-contrast Computed Tomography (CT) scan is the definitive standard of care. Advanced 3D templating software allows the surgeon to assess glenoid morphology accurately, utilizing the modified Walch classification to categorize wear patterns. The surgeon can measure precise vault depth, calculate native version and inclination, and template baseplate positioning. This digital rehearsal allows for the optimization of screw trajectories to maximize purchase in the best available native bone stock, often targeting the base of the coracoid and the scapular spine.
Magnetic Resonance Imaging (MRI) is utilized selectively, primarily to evaluate the integrity of the rotator cuff musculature and assess for fatty infiltration using the Goutallier classification system. In cases of advanced osteoarthritis, an intact subscapularis and supraspinatus (Goutallier stage 0-2) generally support the use of an anatomic prosthesis, whereas advanced fatty degeneration (Goutallier stage 3-4) mandates a reverse geometry implant to bypass the dysfunctional cuff force couples.


Patient Positioning and Operating Room Setup
Proper patient positioning is critical for maximizing exposure and minimizing intraoperative frustration. The patient is typically placed in a modified beach-chair position, with the backrest elevated to approximately 30 to 45 degrees. The patient must be translated laterally on the operative table so that the entire medial border of the scapula is free and unsupported by the table mattress. This allows for unrestricted extension and external rotation of the arm, which is mechanically necessary to deliver the humeral head out of the anterior wound.
The head must be securely immobilized in a neutral position using a specialized headrest, ensuring that the cervical spine is not subjected to excessive lateral flexion or rotation, which could precipitate a brachial plexus traction injury. All bony prominences must be meticulously padded. The operative arm is draped free to allow for a full, unencumbered range of motion during the procedure.
Many surgeons utilize an articulated arm positioner (e.g., Spider arm or Trimano) to maintain static positioning during critical steps of the procedure, such as glenoid preparation. Alternatively, a dedicated surgical assistant manages the arm, applying precise, dynamic traction and rotation as directed by the primary surgeon. A Mayo stand is often positioned across the patient's lap to support the arm during periods of rest and to provide a stable platform for instrument exchange.
Step-by-Step Surgical Approach and Fixation Technique
Execution of the deltopectoral approach requires a methodical, layered dissection. The surgeon must respect the fascial planes, maintain meticulous hemostasis, and sequentially address the anatomical barriers to achieve adequate exposure of the deep articular structures.



Superficial Dissection and Interval Development
The skin incision begins just lateral to the tip of the coracoid process and extends distally and slightly laterally for approximately 10 to 15 centimeters, following the natural contour of the deltopectoral groove toward the deltoid insertion. Subcutaneous tissue is divided sharply down to the deltopectoral fascia. The cephalic vein is identified visually by its blue hue through the fascia or palpated within the fat of the groove.
The interval is developed sharply. The decision to take the cephalic vein laterally with the deltoid or medially with the pectoralis major is a matter of surgeon preference; however, retracting it laterally generally preserves its major deltoid tributaries and minimizes the risk of avulsion. The clavipectoral fascia, which envelops the conjoint tendon and forms a distinct layer deep to the pectoralis major, is incised longitudinally. This critical maneuver allows the surgeon to sweep the conjoint tendon medially and the deltoid laterally, deploying self-retaining retractors (such as a Kolbel or Richardson retractor) to maintain the superficial exposure.
At this stage, the coracoacromial (CA) ligament is identified, running from the coracoid to the acromion. While partial release may be necessary for exposure, complete resection should be avoided in fracture cases or when rotator cuff deficiency is present, as it serves as a secondary restraint to superior humeral head translation. The subdeltoid and subacromial spaces are bluntly developed with a sweeping finger or a blunt Cobb elevator to free any bursal adhesions, greatly enhancing the mobility of the proximal humerus.
Deep Dissection and Subscapularis Management
With the superficial structures retracted, the inner muscular sleeve comes into full view. The anterior circumflex humeral vessels ("three sisters") are identified at the inferior border of the subscapularis, meticulously ligated, and divided. The management of the subscapularis tendon is the most debated and critical step in the anterior approach. Options include a subscapularis peel off the lesser tuberosity, a formal tendinous tenotomy 1 centimeter medial to the insertion, or a lesser tuberosity osteotomy (LTO).

The lesser tuberosity osteotomy involves taking a wafer of bone with the attached subscapularis tendon, allowing for bone-to-bone healing during closure, which biomechanically provides the strongest and most reliable repair. If a tenotomy or peel is chosen, heavy non-absorbable traction sutures are placed through the tendon edge to control it and prevent medial retraction. Once the subscapularis is mobilized, the underlying anterior joint capsule is sharply incised, often elevating it as a continuous sleeve with the subscapularis tendon.
The arm is then progressively externally rotated and extended. This maneuver mechanically delivers the humeral head out of the anterior wound. An inferior capsular release is performed meticulously, keeping the electrocautery directly on the humeral neck to avoid thermal or direct injury to the axillary nerve, which lies dangerously close to the inferior capsule at the 6 o'clock position.
Glenohumeral Exposure and Osseous Preparation
Once the humeral head is dislocated anteriorly, the surgeon has complete access to the proximal humerus. In the setting of arthroplasty, the anatomical neck is identified, and the humeral head is resected using an oscillating saw along the planned version and inclination angles, protecting the rotator cuff insertions on the greater tuberosity with a Darrach or Hohmann retractor.
To expose the glenoid, the proximal humerus must be translated posteriorly and inferiorly. This is achieved through sequential capsular releases (anterior, inferior, and posterior as needed) and the strategic placement of retractors. A Fukuda or specialized ring retractor is placed posterior to the glenoid rim to lever the humerus out of the way. A pointed Hohmann or Bankart retractor is placed anteriorly over the anterior glenoid neck, and a superior retractor is placed at the base of the coracoid.



With circumferential visualization of the glenoid face, the labrum is excised, and the articular cartilage is removed. The glenoid is then reamed to correct version and establish a bleeding bone bed for component implantation. The precision of this step dictates the long-term survivorship of the glenoid component, as eccentric reaming or failure to correct retroversion will lead to catastrophic early loosening.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, the anterior approach to the shoulder carries inherent risks. Complications can be broadly categorized into intraoperative neurovascular injuries, periprosthetic fractures, and postoperative soft tissue failures or infections. A profound understanding of these risks allows the surgeon to employ preventative strategies and execute immediate salvage protocols when necessary.
Intraoperative nerve injury is a devastating complication. The axillary nerve is the most frequently injured, with transient neur
Clinical & Radiographic Imaging Archive



You Might Also Like