Shoulder Arthroscopy: Advanced Portal Placement, Regional Anatomy, and Surgical Techniques
Key Takeaway
Establishing precise arthroscopic portals is the foundation of successful shoulder surgery. This comprehensive guide details the retrograde method for anterior portal placement, the suprascapular nerve portal, and lateral subacromial access. By mastering the regional anatomy, including the rotator cuff interval and neurovascular safe zones, orthopedic surgeons can optimize instrument trajectory, minimize iatrogenic injury, and effectively address complex glenohumeral and subacromial pathology.
Introduction to Shoulder Arthroscopy Portals
The foundation of any successful arthroscopic shoulder procedure lies in the precise establishment of surgical portals. A poorly placed portal not only compromises visualization and instrument maneuverability but also exponentially increases the risk of iatrogenic injury to the complex neurovascular network surrounding the shoulder girdle. As arthroscopic techniques have evolved to address increasingly complex pathology—ranging from massive, retracted rotator cuff tears to multidirectional instability and superior labral anterior-posterior (SLAP) lesions—the necessity for exact, reproducible portal placement has become paramount.
This comprehensive academic review details the advanced techniques for establishing anterior, lateral, and specialized suprascapular portals. It provides an exhaustive analysis of the regional anatomy, biomechanical rationale for portal trajectories, and strict evidence-based protocols for avoiding catastrophic neurovascular complications.
The Retrograde Method for Anterior Portal Placement
The anterior portal is the primary working portal for glenohumeral joint procedures, including Bankart repairs, capsular plications, and biceps tenodesis. While an "outside-in" technique utilizing a spinal needle is common, the retrograde method (or "inside-out" technique) remains a highly reliable alternative, particularly in larger, more muscular patients where external palpation of landmarks is obscured.
Step-by-Step Surgical Technique
The retrograde method ensures that the anterior portal perfectly traverses the rotator cuff interval without damaging the surrounding tendinous structures. The procedure is executed as follows:
- Initial Glenohumeral Evaluation: Establish the standard posterior viewing portal (typically 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion). Perform a diagnostic sweep of the glenohumeral joint.
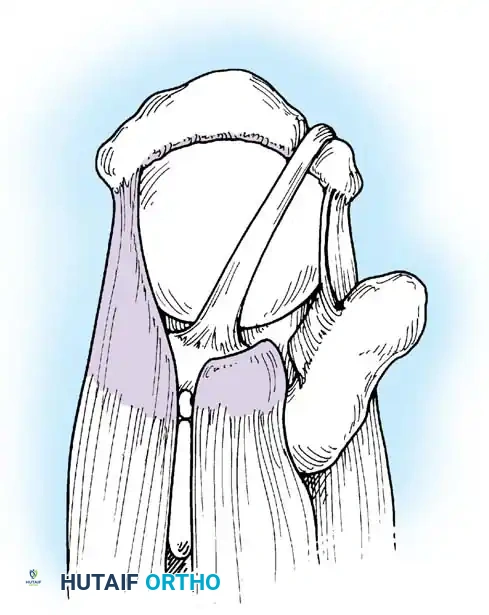
- Targeting the Soft Spot: "Drive" the arthroscope, still housed within its protective sheath, directly across the joint space toward the anterior "soft spot." This soft spot represents the rotator cuff interval, a triangular anatomical space bounded superiorly by the anterior margin of the supraspinatus, inferiorly by the superior border of the subscapularis, and medially by the base of the coracoid process.
- Sheath Positioning: Once the tip of the arthroscope is firmly pressed against the anterior capsule within the interval, carefully remove the arthroscope optic from its sheath. Maintain strict, unyielding pressure on the sheath to keep it firmly docked against the anterior capsular structures.
- Advancing the Wissinger Rod: Pass a Wissinger rod (or a large, blunted Steinmann pin) through the posterior cannula. Advance it smoothly through the anterior capsule, traversing the deltopectoral interval, until the anterior skin is visibly tented.
- Establishing the Portal: Make a precise, controlled skin incision (typically using a #11 blade) directly over the tented tip of the rod. Advance the rod completely past the skin.
- Cannula Insertion: Pass a clear, threaded working cannula over the protruding anterior aspect of the Wissinger rod. Advance the cannula retrograde (from outside to inside) along the rod until it enters the glenohumeral joint. Finally, remove the Wissinger rod, leaving the anterior working portal established.
🔪 Surgical Pearl: The Retrograde Trade-off
While the retrograde method guarantees intra-articular entry through the rotator interval and is technically easier in obese or heavily muscled patients, it affords less flexibility in final portal positioning compared to the outside-in spinal needle technique. If a specific trajectory is required for inferior anchor placement (e.g., at the 5:30 position on the glenoid face), the outside-in method may be preferable.
Anatomical Considerations and Neurovascular Safe Zones
The anterior portal traverses the clavicular portion of the deltoid muscle and enters the rotator cuff interval of the anterior capsule. Mastery of the surrounding anatomy is non-negotiable, as several critical structures are at risk during this maneuver.
- The Cephalic Vein: Located laterally within the deltopectoral groove. Medial deviation during rod advancement can lacerate this vessel, leading to significant hematoma and obscured visualization.
- The Musculocutaneous Nerve (MCN): The MCN typically enters the coracobrachialis muscle 3 to 5 cm inferior to the tip of the coracoid process. However, significant anatomical variations exist. Plunging instruments too far inferiorly or medially places this nerve at extreme risk.
- The Brachial Plexus and Axillary Vessels: These structures lie anteromedially to the coracoid process.
⚠️ Surgical Warning: The Coracoid Safe Zone
To avoid catastrophic injury to the brachial plexus and axillary vascular bundle, the surgeon must adhere strictly to two anatomical rules: (1) Always stay lateral to the coracoid process, and (2) Always remain superior to the leading edge of the subscapularis tendon. Violating the medial or inferior boundaries of the rotator interval invites severe neurovascular compromise.
Specialized Portals: The Suprascapular Nerve Portal
As arthroscopic techniques have advanced, the ability to perform nerve decompressions entirely endoscopically has revolutionized the management of suprascapular neuropathy. The suprascapular nerve portal, popularized by Lafosse, provides direct, inline access to the suprascapular notch.
Indications for the Suprascapular Portal
- Arthroscopic release of the superior transverse scapular ligament for suprascapular nerve entrapment.
- Excision of spinoglenoid or suprascapular notch paralabral cysts.
- Mobilization of massive, chronically retracted posterosuperior rotator cuff tears where the nerve is tethered.
Landmarks and Surgical Technique (Lafosse Method)
The suprascapular nerve portal is established to provide a parallel trajectory to the suprascapular nerve as it traverses the notch.
- Positioning: The portal is positioned in the superior fossa, between the posterior clavicle and the scapular spine.
- Measurements: It is located approximately 7 cm medial to the lateral border of the acromion. This places it approximately 2 cm medial to the standard Neviaser portal (which is typically located in the soft spot bounded by the clavicle, acromion, and scapular spine).
- Execution: Under direct intra-articular or subacromial visualization, a spinal needle is introduced vertically. The trajectory must be carefully monitored to avoid plunging into the supraspinatus muscle belly. Once the correct angle is confirmed, a #11 blade is used to incise the skin, and a blunt trocar is used to spread the trapezius muscle fibers, granting access to the suprascapular notch.
Anatomical Risks at the Suprascapular Notch
The suprascapular nerve passes under the superior transverse scapular ligament, while the suprascapular artery and vein pass over it (remembered by the mnemonic: "Army goes over the bridge, Navy goes under"). When releasing the ligament, the surgeon must use arthroscopic scissors or a specialized tissue elevator, keeping the inferior blade directly against the ligament to avoid lacerating the underlying nerve or the overlying artery.
Subacromial Space Access: Lateral, Posterolateral, and Anterolateral Portals
Accessing the subacromial space is mandatory for procedures such as subacromial decompression, acromioclavicular (AC) joint resection, and rotator cuff repair. The lateral portal serves as the primary operative and viewing portal for this anatomical region.
The Lateral Portal: Anatomy and Establishment
The lateral portal is the workhorse of subacromial surgery. It provides an unparalleled orthogonal view of the rotator cuff footprint and the undersurface of the acromion.
- Location: The portal is located exactly 3 cm lateral to the lateral border of the acromion, typically in line with the posterior aspect of the clavicle.
- Trajectory: The portal passes directly through the deltoid muscle. When advancing the cannula or arthroscope, the instrument must be directed downward (inferiorly) and medially toward the greater tuberosity. This trajectory allows the instrument to slip smoothly beneath the acromion and enter the lateral extent of the subacromial bursa.
- Impingement Avoidance: A common pitfall for junior surgeons is directing the trocar too horizontally, causing the cannula to impinge on the lateral acromial edge. This not only damages the acromion but severely restricts instrument mobility.
⚠️ Surgical Warning: The Axillary Nerve Danger Zone
The axillary nerve courses circumferentially around the surgical neck of the humerus, lying approximately 5 cm (50 mm) distal to the lateral border of the acromion. To prevent iatrogenic denervation of the deltoid, lateral portal incisions must never extend beyond 3 to 4 cm distal to the acromion. Furthermore, deltoid-splitting incisions should be made longitudinally, parallel to the muscle fibers, rather than transversely.
Transitioning from Glenohumeral to Subacromial Space
Arthroscopy of the subacromial space can usually be accomplished by repurposing the initial posterior and central anterior portals used for the glenohumeral joint.
- Redirection: After completing the intra-articular work, the arthroscope and anterior cannula are withdrawn just outside the glenohumeral capsule but kept deep to the deltoid and subcutaneous tissues.
- Entering the Bursa: The cannulas are then redirected superiorly into the subacromial bursa from the exact same skin incisions.
- Anterior Portal Palpation: When passing the anterior cannula into the subacromial space, gentle, tactile palpation with the blunt trocar tip can reveal the firm, unyielding extent of the coracoacromial (CA) ligament. Recognizing this landmark allows the surgeon to redirect the cannula just lateral to the ligament, avoiding inadvertent damage to the CA arch before a formal decompression is planned.
Managing the Muscular Patient
In very muscular individuals, or if the initial posterior portal was placed too far inferiorly for optimal glenohumeral viewing, redirecting the posterior portal into the subacromial space may result in a poor trajectory that fights the soft tissue envelope. In such cases, forcing the trajectory will lead to fluid extravasation and instrument bending.
- Solution: Do not hesitate to establish a new, dedicated posterior subacromial portal. This is typically placed 1.5 cm inferior and slightly lateral to the posterior corner of the acromion, providing a direct, unhindered view of the subacromial space.
Accessory Portals: Burkhart’s SLAP Portals
For advanced pathology, such as Type II SLAP lesions, standard anterior and posterior portals often fail to provide the correct angle of approach for anchor insertion. Stephen Burkhart, MD, described the necessity of specialized lateral portals to achieve the "deadman's angle" (an insertion angle of 45 degrees or less to the articular surface) for superior labral repair.
- The Portals of Wilmington: Depending on the exact site of the superior labral disruption (anterior to the biceps anchor vs. posterior to the biceps anchor), accessory anterolateral or posterolateral portals are established just off the anterolateral or posterolateral corners of the acromion.
- Biomechanical Advantage: These portals allow a percutaneous trans-cuff approach (passing a spinal needle directly through the muscular portion of the supraspinatus or the rotator interval) to achieve a perfect 45-degree angle to the superior glenoid rim, ensuring maximum anchor pull-out strength and anatomical labral reduction.
Postoperative Protocols and Complication Management
Managing Portal-Related Complications
Even with meticulous technique, portal-related complications can occur. The most common is fluid extravasation.
- Pathophysiology: Prolonged surgical times or high pump pressures can force irrigation fluid into the deltoid, pectoral, and fascial planes of the neck.
- Prevention and Management: Utilize the lowest effective pump pressure (typically 30-40 mmHg, increasing only temporarily for bleeding control). Ensure cannulas are fully seated and not backing out of the capsule. If massive extravasation occurs, the procedure must be expedited or aborted to prevent airway compromise or compartment syndrome of the arm.
Rehabilitation Implications
Portal placement rarely dictates the postoperative rehabilitation protocol, which is primarily driven by the underlying pathology repaired (e.g., rotator cuff vs. labrum). However, patients should be educated on portal site care.
* Sutures are typically removed at 10 to 14 days.
* Patients may experience localized tenderness at the lateral portal site due to the deltoid split; this is self-limiting and resolves with standard cryotherapy and early passive range of motion as dictated by the primary repair protocol.
Conclusion
The mastery of shoulder arthroscopy is inextricably linked to the mastery of portal placement. Whether utilizing the retrograde method for precise anterior access, navigating the complex anatomy of the suprascapular notch, or establishing orthogonal lateral portals for subacromial work, the surgeon must possess a profound understanding of three-dimensional regional anatomy. By adhering to established safe zones—such as remaining lateral to the coracoid and respecting the 5 cm axillary nerve boundary—orthopedic surgeons can consistently achieve optimal visualization, superior biomechanical angles for repair, and the highest standards of patient safety.
You Might Also Like