Shoulder Arthroscopy Portals: Surgical Technique & Anatomy
Key Takeaway
Establishing precise portals is the foundational step in shoulder arthroscopy. The standard posterior portal serves as the primary viewing corridor, while anterior portals established through the rotator interval facilitate instrumentation. Mastery of anatomical landmarks, such as the coracoid process and acromion, is critical to optimize surgical trajectories and prevent iatrogenic neurovascular injury to the suprascapular and axillary nerves during complex glenohumeral reconstructions.
INTRODUCTION TO SHOULDER ARTHROSCOPY PORTALS
The foundation of any successful shoulder arthroscopy lies in the precise and safe establishment of surgical portals. Accurate portal placement dictates the surgeon’s ability to visualize intraarticular pathology, achieve proper instrument triangulation, and execute complex reconstructive procedures without iatrogenic injury to the surrounding neurovascular structures.
Shoulder arthroscopy demands a profound three-dimensional understanding of the glenohumeral joint, the subacromial space, and the extraarticular neurovascular anatomy. Portals must be strategically placed to allow parallel or convergent access to the glenoid articular surface, the labrum, and the rotator cuff footprint. This comprehensive guide details the indications, anatomical landmarks, biomechanical considerations, and step-by-step surgical techniques for establishing standard and accessory shoulder arthroscopy portals.
ESTABLISHING THE STANDARD POSTERIOR PORTAL
The standard posterior portal is universally recognized as the primary viewing portal for diagnostic shoulder arthroscopy. It provides a panoramic view of the glenohumeral joint, including the anterior labrum, the rotator interval, the biceps anchor, and the humeral head.
Anatomical Landmarks and Positioning
Accurate identification of osseous landmarks is paramount. The surgeon must palpate and mark the following structures prior to insufflation:
* The posterolateral corner of the acromion.
* The lateral and posterior borders of the acromion.
* The coracoid process anteriorly.
* The spine of the scapula.
The classic "posterior soft spot" is located approximately 1.5 to 2.0 cm inferior and 1.5 to 2.0 cm medial to the posterolateral corner of the acromion. This interval lies between the infraspinatus and teres minor muscles.
Step-by-Step Surgical Technique
- Joint Localization: Establish the posterior portal by inserting an 18-gauge spinal needle through the posterior soft spot, directing it into the glenohumeral joint.
- Tactile Navigation: Place the index or long finger of the free hand on the tip of the coracoid process anteriorly. Direct the spinal needle anteromedially toward the palpated coracoid.
- Entering the Joint: The needle should meet minimal resistance as it traverses the posterior capsule and enters the joint space.
- Troubleshooting: If the needle abuts the humeral head, redirect it slightly superiorly over the humeral head to allow deeper penetration and ensure an intraarticular location.
- Troubleshooting: If the needle is placed too far medially and abuts the posterior glenoid rim, it can be gently "walked up" the posterior glenoid surface laterally until it slips into the joint space.
- Joint Insufflation: Once the capsule is breached and intraarticular placement is confirmed, inject 30 to 40 mL of sterile saline into the joint.
- Clinical Note: In patients with significant adhesive capsulitis, the joint volume is drastically reduced, and far less fluid (often 10-15 mL) will be accepted. Backflow or high resistance indicates either a contracted capsule or extraarticular needle placement.
- Incision and Trocar Insertion: Remove the needle and make a standard stab incision through the dermis. Insert the arthroscopic cannula with a blunt trocar along the exact trajectory established by the spinal needle.
🔪 Surgical Warning: Neurovascular Risks of the Posterior Portal
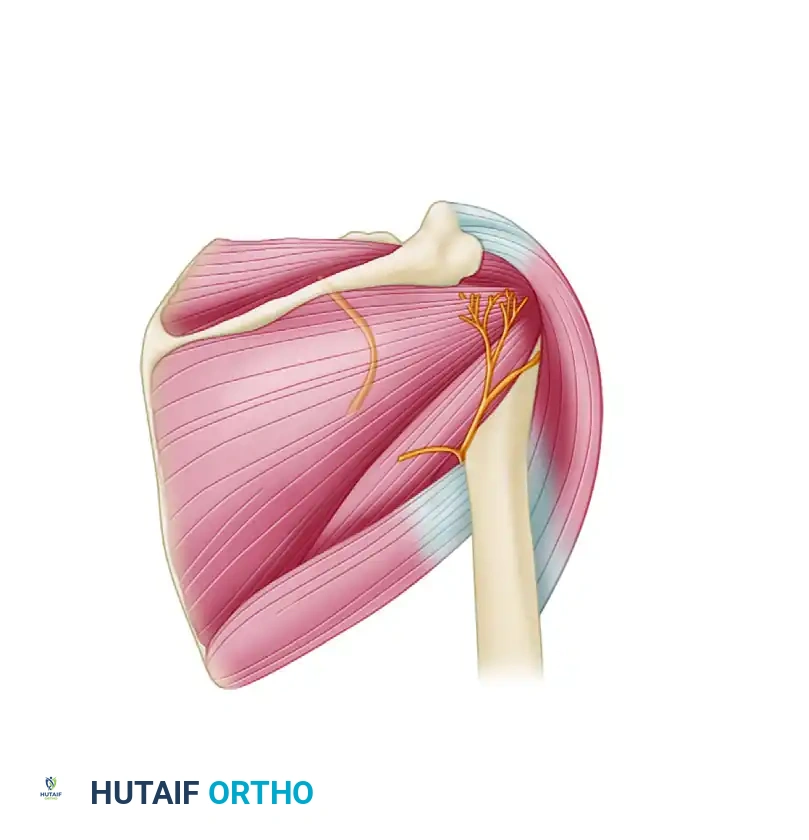
Deviation from the standard posterior soft spot carries significant neurovascular risks. Placing the portal too far medially endangers the suprascapular nerve as it courses through the spinoglenoid notch. Placing the portal too far inferiorly or laterally risks iatrogenic injury to the axillary nerve and posterior circumflex humeral artery as they exit the quadrangular space.
FIGURE 52-5: Posterior shoulder portal risks. Injury to the suprascapular nerve occurs if the portal is placed too medial, and to the axillary nerve if placed too inferior or lateral.
Modifications for Specific Procedures
If a posterior stabilization procedure (e.g., posterior Bankart repair) is contemplated, the standard posterior portal may not provide the optimal angle of approach. By placing the portal 1.0 cm medial to the posterolateral acromion, the trajectory can be made approximately parallel to the glenoid articular surface, facilitating easier passage of arthroscopic instrumentation to the anterior and inferior aspects of the joint.
Alternatively, if two posterior portals are necessary for complex posterior work, the initial viewing portal is made 1.5 to 2.0 cm inferiorly in line with the acromial edge. A second posterior working portal can subsequently be established under direct intraarticular vision.
ESTABLISHING ANTERIOR PORTALS
Anterior portals are essential working portals for both diagnostic examination and surgical stabilization. They allow direct observation of the posterior capsule, the articular surface of the rotator cuff, the glenohumeral ligaments, and the subscapularis tendon.
The Rotator Interval: The Anterior "Safe Zone"
All standard anterior portals pass through the anterior "soft spot," which corresponds anatomically to the rotator interval. This intraarticular triangle is bounded by:
* Superiorly: The intraarticular portion of the long head of the biceps tendon.
* Inferiorly: The superior rolled edge of the subscapularis tendon.
* Medially (Base): The anterior edge of the glenoid rim.
Techniques for Anterior Portal Placement
The anterior portal is always established after the posterior viewing portal has been created. The posteriorly placed arthroscope is used to visually assist and confirm the safe establishment of anterior portals. Two primary techniques are utilized:
1. The Outside-In (Antegrade) Technique
This is the preferred method for precise localization, particularly for complex reconstructions.
* A spinal needle is introduced percutaneously through the anterior skin, guided by external landmarks (typically slightly lateral to a point halfway between the anterolateral tip of the acromion and the coracoid process).
* The needle is visualized intraarticularly entering the rotator interval.
* The trajectory is assessed to ensure it provides the correct angle of approach to the targeted pathology (e.g., the anterior inferior glenoid for a Bankart repair).
* Once the optimal trajectory is confirmed, a skin incision is made, and a cannula is introduced over a switching stick or via direct visualization.
2. The Inside-Out (Retrograde) Technique
- The arthroscope is temporarily withdrawn from the posterior portal cannula.
- A Wissinger rod (a long, blunt-tipped switching stick) is passed through the posterior cannula, across the joint space, and pushed firmly against the anterior capsule within the rotator interval.
- The humerus is maximally adducted to relax the anterior structures.
- The rod is advanced until it tents the anterior skin. A small incision is made over the tented skin, allowing the rod to exit anteriorly.
- An anterior cannula is then slid over the Wissinger rod into the joint.
💡 Clinical Pearl: Portal Separation
When anterior stabilization procedures are contemplated, multiple anterior portals may be required. These portals should be separated by at least 1.5 to 2.0 cm to allow easy placement of instruments without overcrowding, instrument convergence ("sword-fighting"), or disruption of the visual field.
COMPREHENSIVE ATLAS OF SHOULDER PORTALS
The evolution of shoulder arthroscopy has led to the description of numerous specialized portals tailored to specific pathologies.
Anterior Working Portals
- Anterior Central Portal (Matthews): The most commonly utilized anterior portal. The skin entry point is just lateral to the coracoid process. It enters the joint precisely through the center of the rotator interval triangle.
- Anterior Inferior Portal (Wolf): Established by allowing the instrumentation to slide directly off the inferior edge of the coracoid tip. It enters the joint just superior to the inferior glenohumeral ligament, at the junction of the middle and inferior thirds of the subscapularis tendon. Excellent for low anterior Bankart repairs.
- 5 O’Clock Portal (Davidson): A percutaneous localization technique approximately 1 cm inferior and just lateral to the coracoid (maintaining a 1 cm safe distance from the cephalic vein). It targets the leading edge of the inferior glenohumeral ligament at the 5-o’clock position on the right shoulder.
- Anterior Superior Portal (Wolf): Located at the mid-distance between the coracoid and the anterolateral acromion. It enters the joint just anterior to the long head of the biceps tendon. Frequently used as an accessory portal for fluid inflow or suture management.
Posterior and Posteroinferior Portals
- Central Posterior Portal (Wolf): Located 2 cm medial and 3 cm inferior to the posterolateral corner of the acromion, directed toward the coracoid.
- Posterolateral Portal (Ellman): Located 2 cm below the lateral edge of the acromion, in the prolongation of its posterior edge. It enters medially to the subacromial bursa, just medial to the lateral ledge of the acromion.
- 7 O’Clock Posteroinferior Portal (Davidson and Rivenburgh): An accessory posterior working portal that allows direct access to the inferior glenohumeral capsule, crucial for posterior Bankart repairs and posterior capsular shifts.
- Technique: Can be created inside-out using a switching stick passed through an anterior 3-o’clock portal and directed posteroinferiorly. Alternatively, an outside-in technique utilizes a small skin incision 2 to 3 cm inferior to the standard posterior viewing portal, inserting a blunt-tipped rod under direct intraarticular vision to avoid the axillary nerve.
Superior and Lateral Portals
- Superolateral Portal (Laurencin): Located lateral to the acromion on a line drawn from the acromion to the coracoid. It enters the joint obliquely, directly above the biceps tendon, piercing the rotator interval tissue.
- Anterolateral Portal (Ellman/Altchek): Located 1 to 2 cm below the lateral edge of the acromion in the prolongation of its anterior edge. It enters the glenohumeral joint directly through the rotator interval.
- Surgical Warning: If this portal is utilized, a large-diameter inflow sheath should be avoided to prevent iatrogenic damage to the surrounding rotator cuff musculature.
- Portal of Wilmington: Located 1 cm anterior and 1 cm lateral to the posterolateral corner of the acromion. It provides a perfect 45-degree approach angle to the posterosuperior glenoid labrum, making it the premier portal for SLAP (Superior Labrum Anterior and Posterior) lesion repairs.
- Transrotator Cuff Portal (O’Brien): Located 1 cm posterior and 2 cm lateral to the anterolateral corner of the acromion. It passes directly through the muscular portion of the supraspinatus to target the 11-o’clock position on the glenoid labrum (in a right shoulder), medial to the rotator arch.
- Neviaser Portal (Superior Portal): Located in the superior "soft spot" bounded by the clavicle anteriorly, the medial edge of the acromion laterally, and the spine of the scapula posteriorly. The instrument is directed downward at a 30-degree angle laterally and slightly posteriorly into the glenohumeral joint. Excellent for superior labral repairs and passing sutures through the posterior band of the inferior glenohumeral ligament.
- Superior Suprascapular Nerve Portal (Lafosse): A highly specialized percutaneous portal located approximately 7 cm medial to the lateral border of the acromion and 2 cm medial to the Neviaser portal. It provides direct access to the suprascapular notch for arthroscopic nerve release.
POSTOPERATIVE PROTOCOLS AND COMPLICATION MANAGEMENT
Fluid Extravasation and Compartment Syndrome
Shoulder arthroscopy requires continuous fluid irrigation to maintain joint distension and visual clarity. However, prolonged surgical times or the use of high-pressure pumps can lead to significant fluid extravasation into the deltoid, pectoral, and cervical fascial planes.
* Prevention: Maintain pump pressures at the lowest effective setting (typically 30-40 mmHg, increasing temporarily only for bleeding control). Ensure outflow portals are patent.
* Management: Monitor the tension of the deltoid and pectoral muscles throughout the case. Severe extravasation can rarely lead to airway compromise or neurovascular compression, necessitating immediate cessation of the procedure.
Portal Closure and Wound Care
Following the completion of the arthroscopic procedure, the joint is thoroughly irrigated to remove debris and loose bodies. The portals are closed based on surgeon preference, typically utilizing simple interrupted non-absorbable sutures (e.g., 3-0 Nylon) or adhesive skin closures.
* In cases where significant capsular releases were performed, leaving the portals open to drain for 24 hours may reduce postoperative hematoma formation and swelling.
* Sterile compressive dressings are applied, and the patient is placed in a specialized shoulder immobilizer or sling, depending on the specific reconstructive procedure performed.
Early Rehabilitation Considerations
Portal placement directly influences early postoperative pain and rehabilitation. Trans-tendinous portals (such as the O'Brien portal or an aggressive anterolateral portal) may result in localized rotator cuff inhibition or pain during early active-assisted range of motion. Rehabilitation protocols must be tailored not only to the primary repair (e.g., Bankart or rotator cuff repair) but also with consideration of the muscular and capsular morbidity induced by the portal tracts themselves. Strict adherence to evidence-based, phased physical therapy is mandatory for optimal functional recovery.
You Might Also Like
