Arthroscopic Management of Degenerative Shoulder Pathologies: Calcific Tendinitis, Osteoarthritis, and Acromioclavicular Resection
Key Takeaway
Degenerative shoulder conditions, including calcific tendinitis, glenohumeral osteoarthritis, and acromioclavicular joint arthropathy, frequently require surgical intervention when conservative measures fail. This guide details the pathogenesis of rotator cuff calcification, the role of arthroscopic debridement in early osteoarthritis, and a step-by-step surgical technique for arthroscopic distal clavicle excision using the superior approach. Mastery of these techniques ensures optimal joint preservation, pain relief, and functional restoration.
INTRODUCTION TO DEGENERATIVE SHOULDER PATHOLOGIES
The management of degenerative and reactive conditions of the shoulder requires a profound understanding of glenohumeral and acromioclavicular biomechanics, cellular pathology, and precise arthroscopic anatomy. Conditions such as calcific tendinitis of the rotator cuff, early glenohumeral osteoarthritis, and acromioclavicular (AC) joint arthropathy frequently present with overlapping clinical symptoms, including insidious pain, mechanical catching, and restricted range of motion.
While conservative modalities remain the first line of treatment, arthroscopic intervention is highly efficacious for refractory cases. This chapter provides an exhaustive, evidence-based analysis of the pathogenesis, clinical evaluation, and advanced arthroscopic management of these three distinct yet frequently coexisting shoulder pathologies.
CALCIFIC TENDINITIS OF THE ROTATOR CUFF
Calcific tendinitis is a reactive, self-limiting condition characterized by the deposition of basic calcium phosphate crystals within the tendons of the rotator cuff, most commonly affecting the supraspinatus tendon (specifically the critical zone, approximately 1 to 2 cm proximal to its insertion on the greater tuberosity).
Pathogenesis and Cellular Biomechanics
Although the exact etiology remains a subject of academic debate, the prevailing consensus supports the theory of local tissue hypoxia and subsequent fibrocartilaginous metaplasia. Hypoperfusion in the critical zone of the rotator cuff induces tenocyte necrosis and degeneration, creating a microenvironment conducive to calcium precipitation.
The natural history of calcific tendinitis is classically divided into three distinct phases, as described by Uhthoff:
* Precalcific Phase: Localized tissue hypoxia leads to fibrocartilaginous transformation of the tendon tissue. This phase is typically asymptomatic.
* Calcific Phase: Subdivided into formative, resting, and resorptive stages. During the formative stage, calcium crystals are deposited in matrix vesicles. The resting stage is characterized by a stable calcific deposit bordered by fibrocartilage. The resorptive stage involves intense neovascularization and macrophage infiltration to phagocytose the calcium.
* Postcalcific Phase: Fibroblasts remodel the resultant defect, restoring the normal collagenous architecture of the tendon.
Clinical Pearl: The acute resorptive phase is characterized by an intense inflammatory response. The intratendinous pressure rises dramatically as the calcium deposit transforms into a toothpaste-like consistency. Patients present with excruciating, unremitting pain, profound inflammation, and severe pseudoparalysis, a clinical picture that closely mimics acute septic arthritis of the shoulder.
Clinical Evaluation and Nonoperative Management
Diagnosis is confirmed via standard orthogonal radiographs (anteroposterior, scapular Y, and axillary lateral views), which reveal amorphous radiodensities within the cuff footprint. Ultrasound is highly sensitive for localizing the deposit and assessing its consistency (hard and shadowing vs. soft and cystic).
Conservative treatment is the mainstay for this exquisitely painful condition and consists of:
* Pharmacotherapy: Aggressive use of nonsteroidal anti-inflammatory drugs (NSAIDs) to modulate the inflammatory cascade.
* Cryotherapy: Intermittent icing to induce local vasoconstriction and reduce edema.
* Corticosteroid Injections: A local subacromial injection of a long-acting anesthetic (e.g., bupivacaine) combined with a corticosteroid can provide rapid symptomatic relief, particularly during the acute resorptive phase.
* Ultrasound-Guided Barbotage: Needling and lavage of the calcific deposit to decompress the tendon and aspirate the calcium.
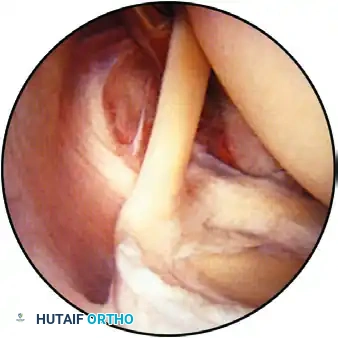
Arthroscopic Management
Surgical intervention is indicated for chronic, refractory pain lasting longer than 6 months, or for recurrent acute attacks that fail conservative management. Arthroscopic excision involves localizing the deposit (often visible as a hyperemic "strawberry lesion" on the bursal surface of the cuff), incising the tendon longitudinally in line with its fibers, and meticulously curetting the calcium. If a significant structural defect remains following excision, a formal rotator cuff repair must be performed to restore the footprint biomechanics.
GLENOHUMERAL OSTEOARTHRITIS: ARTHROSCOPIC DEBRIDEMENT
Glenohumeral osteoarthritis in the young, active patient presents a complex surgical dilemma. While total shoulder arthroplasty remains the gold standard for end-stage disease, arthroscopic debridement serves as a valuable joint-preserving, palliative procedure for patients with mild to moderate degenerative changes who wish to delay arthroplasty.
Rationale and Clinical Evidence
Arthroscopic debridement aims to eliminate mechanical irritants, reduce the intra-articular inflammatory burden, and improve kinematics. Weinstein et al. reported a landmark series of 25 patients who underwent arthroscopic debridement for degenerative arthritis. Their comprehensive treatment protocol yielded an 80% success rate in carefully selected patients.
The procedure, often referred to as Comprehensive Arthroscopic Management (CAM), typically includes:
* Copious Lavage: To remove inflammatory cytokines, metalloproteinases, and microscopic cartilaginous debris.
* Loose Body Removal: Extraction of osteochondral fragments that cause mechanical catching and third-body wear.
* Labral Debridement: Excision of unstable, degenerative labral tears that contribute to mechanical symptoms.
* Chondroplasty: Debridement of unstable chondral flaps to a stable rim, preventing further delamination.
* Rotator Cuff Debridement: Smoothing of partial-thickness articular-sided rotator cuff tears.
* Capsular Release: In cases with concomitant adhesive capsulitis or significant contracture, a targeted capsular release (particularly the inferior and posterior capsule) can significantly restore range of motion.
Surgical Warning: Arthroscopic debridement for osteoarthritis is strictly palliative. Patients must be extensively counseled preoperatively that the procedure does not alter the underlying natural history of the disease, and future arthroplasty may still be required. Poor prognostic factors include joint space narrowing of less than 2 mm, large kissing lesions, and significant posterior glenoid wear (B2 glenoid).
ACROMIOCLAVICULAR JOINT PATHOLOGY: THE SUPERIOR APPROACH
Osteoarthritis and osteolysis of the acromioclavicular (AC) joint are common sources of superior shoulder pain. When conservative measures (activity modification, NSAIDs, intra-articular corticosteroid injections) fail, surgical excision of the distal clavicle is highly effective.
Historically performed via an open approach, arthroscopic distal clavicle excision has become the gold standard due to its ability to preserve the superior AC capsular ligaments, thereby maintaining anteroposterior stability of the clavicle.
Biomechanics of the Acromioclavicular Joint
The AC joint is a diarthrodial joint stabilized by static and dynamic restraints. The static restraints include the AC ligaments (superior, inferior, anterior, and posterior) and the coracoclavicular (CC) ligaments (conoid and trapezoid).
* The superior and posterior AC ligaments are the primary restraints to anteroposterior translation of the distal clavicle.
* The CC ligaments are the primary restraints to superior translation.
The critical advantage of the arthroscopic superior approach is the meticulous preservation of the superior AC ligament complex. Open resections often violate this structure, leading to postoperative anteroposterior instability and persistent pain.
🔪 Surgical Technique 52-25: Arthroscopic Distal Clavicle Excision (Flatow et al.)
The following technique describes a direct superior arthroscopic approach to the AC joint, allowing for precise, visually controlled resection of the distal clavicle while preserving the vital stabilizing soft tissue envelope.
1. Preoperative Setup and Anesthesia
- Positioning: Place the patient in the standard "beach chair" position. Ensure the head and neck are securely stabilized in a neutral position to prevent cervical spine complications. The operative arm should be draped free to allow dynamic manipulation during the procedure.
- Anesthesia: Administer a regional interscalene block (scalene block) in conjunction with general anesthesia to ensure profound intraoperative muscle relaxation and optimal postoperative pain control.
2. Portal Placement and Joint Localization
- Needle Localization: The AC joint can be narrow and difficult to access, particularly in the presence of large osteophytes. Use 18-gauge spinal needles to accurately determine the location, inclination, and orientation of the joint space before introducing any surgical instruments.
- Joint Distention: Inject several milliliters of normal saline solution through the 18-gauge needle directly into the AC joint to distend the capsule and facilitate instrument insertion.
- Portal Creation: Make two distinct portal sites directly superior to the joint: one anterior to the joint line and one posterior to the joint line.
3. Diagnostic Arthroscopy and Synovectomy
- Initial Instrumentation: Due to the tight confines of the degenerative AC joint, begin by introducing a 2.7-mm wrist arthroscopy unit. Utilize this smaller scope until adequate space is created for a standard 4.0-mm shoulder arthroscope.
- Hemostasis and Irrigation: Use a radiofrequency electrocautery probe to coagulate small bleeders immediately. Maintaining a clear visual field is paramount. Use normal saline (or glycine) mixed with 1:300,000 epinephrine delivered via a pressure pump for continuous irrigation.
- Synovectomy: Introduce a full-radius resector (shaver) through the alternating portal. Perform a complete, meticulous synovectomy. Clean all intervening soft tissue, meniscoid intra-articular disc remnants, and any remaining degraded cartilage from the articular surface of the outer end of the clavicle using a combination of the shaver and an arthroscopic curet.
4. Bone Resection: The "Shelling Out" Technique
- Capsular Preservation: Using the electrocautery unit, carefully "shell out" the outer end of the clavicle. The goal is to subperiosteally dissect the bone away from the capsule so that the robust tube of soft tissue containing the superior acromioclavicular ligament and capsule is strictly preserved.
- Burr Resection: Begin the bone resection using a small (2.0-mm) arthroscopic burr to establish the initial working space. Once adequate space is achieved, upsize to larger (3.5-mm to 4.5-mm) burrs to expedite bone removal.
- Alternating Portals: Switch the arthroscope and the burr between the anterior and posterior portals. This alternating perspective is critical to ensure that bone is removed adequately and symmetrically under direct vision, preventing asymmetric resection.
- Resection Depth: Resect approximately 5 to 8 mm of the distal clavicle. Resection beyond 10 mm is generally unnecessary and risks compromising the coracoclavicular ligaments, which insert roughly 1.5 to 3 cm medial to the joint line.
Pitfall: Failure to resect the posterior-superior corner of the distal clavicle is the most common cause of persistent postoperative pain. The alternating portal technique ensures this blind spot is adequately visualized and resected.
5. Final Sculpting and Inspection
- Beveling: Perform final beveling of the resected clavicular edge using arthroscopic rasps or a fine burr. The goal is to create a smooth, contoured surface without sharp cortical edges that could abrade the overlying capsule.
- Dynamic Examination: Carefully examine the joint with the arthroscope from both the anterior and posterior portals. Probe the edges of the resection to confirm that no overhanging ridges or residual osteophytes remain.
- Debris Clearance: Thoroughly irrigate the joint and visually check for any loose fragments of bone or cartilage that may have fallen into the dependent recesses of the joint. The direct superior approach affords excellent, unobstructed exposure for this final "sculpturing" phase.
6. Closure and Postoperative Analgesia
- Analgesia: After withdrawing the arthroscopic instruments, inject 10 to 15 mL of 0.25% bupivacaine (Marcaine) without epinephrine directly into the AC joint space and surrounding subcutaneous tissues for extended postoperative comfort.
- Closure: Close the anterior and posterior portal sites using resorbable sutures (e.g., 3-0 Monocryl) in a subcuticular fashion, followed by sterile adhesive strips and a compressive dressing.
Postoperative Care and Rehabilitation Protocol
The preservation of the superior AC capsule allows for an accelerated rehabilitation protocol, as there is no structural repair requiring prolonged immobilization.
- Immediate Postoperative Phase (Days 1-2): A standard shoulder sling is worn strictly for comfort. Passive range of motion (PROM) exercises, including pendulum exercises, are allowed and encouraged on the first postoperative day to prevent capsular adhesions.
- Early Active Phase (Days 3-5): Active-assisted and fully active range of motion exercises are initiated as soon as the acute postoperative discomfort resolves, typically within 3 to 5 days. The sling is weaned and discontinued.
- Strengthening Phase (Weeks 2-6): Progressive isometric and isotonic strengthening of the deltoid and rotator cuff musculature is introduced. Scapular stabilization exercises are emphasized to ensure proper periscapular mechanics.
- Return to Activity: Patients are generally cleared to return to full, unrestricted activities, including heavy lifting and overhead sports, by 8 to 12 weeks postoperatively, contingent upon the restoration of painless, full range of motion and symmetric strength.
You Might Also Like