Comprehensive Guide to Subtrochanteric Femoral Fractures: Epidemiology, Anatomy, & Management
Key Takeaway
Subtrochanteric femoral fractures are challenging hip injuries at the metaphyseal-diaphyseal junction. They exhibit unique biomechanical stresses and powerful muscle forces causing characteristic displacement. The thick cortical bone and reduced vascularity complicate fixation, demanding precise surgical planning. This careful approach is crucial for optimal healing outcomes and to mitigate higher rates of nonunion.
Introduction & Epidemiology
Subtrochanteric femoral fractures represent a distinct and challenging subset of hip fractures, characterized by their anatomical location, unique biomechanical environment, and propensity for complications. These fractures occur in the metaphyseal-diaphyseal junction of the femur, an area subjected to immense physiological loads and surrounded by powerful muscle groups. Accurate diagnosis, meticulous surgical planning, and precise execution are paramount for achieving optimal outcomes.
Subtrochanteric fractures account for approximately 10% to 30% of all hip fractures. While commonly associated with high-energy trauma in younger individuals and falls in the elderly, their incidence exhibits a bimodal distribution. A greater incidence is observed in individuals 20 to 40 years of age, typically resulting from high-velocity trauma such as motor vehicle collisions or falls from height. A second, larger peak occurs in persons older than 60 years of age, often associated with lower-energy mechanisms in osteoporotic bone. The increasing prevalence of atypical femoral fractures (AFFs) associated with long-term bisphosphonate use has also contributed to the rising incidence, particularly in the elderly population. These iatrogenic fractures often present with prodromal thigh pain and specific radiographic features.
Surgical Anatomy & Biomechanics
A subtrochanteric femur fracture is precisely defined as a fracture occurring between the lesser trochanter and a point 5 cm distal to the lesser trochanter. This region is a critical transition zone between the cancellous bone of the proximal metaphysis and the thick cortical bone of the diaphysis.
Bony Architecture and Stress Distribution
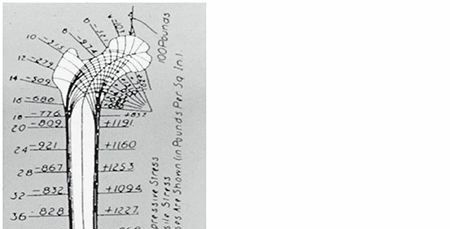
The subtrochanteric segment of the femur is subject to high biomechanical stresses. During ambulation and weight-bearing, the femur acts as a long lever arm, transmitting forces from the pelvis to the tibia. The medial and posteromedial cortices are the sites of high compressive forces, whereas the lateral cortex experiences high tensile forces. The anterolateral cortex is also a zone of significant tensile stress. The interplay of these forces, exacerbated by muscle pull, contributes to the instability and characteristic displacement patterns observed in subtrochanteric fractures. The strong cortical bone in this region makes fixation challenging, as implants must withstand significant cyclic loading.

The subtrochanteric area of the femur is composed mainly of thick cortical bone, in contrast to the more trabecular nature of the intertrochanteric region. This cortical dominance has significant implications for both vascularity and healing potential. Cortical bone, while strong, possesses comparatively less intrinsic vascularity than cancellous bone, relying heavily on periosteal and endosteal blood supplies. The potential for healing is therefore compromised, contributing to higher rates of delayed union and nonunion if surgical principles are not meticulously adhered to.

Muscle Attachments and Deforming Forces
The powerful musculature surrounding the proximal femur exerts considerable deforming forces on fracture fragments, often leading to characteristic displacement patterns that complicate reduction.
-
Proximal Fragment:
- Abduction: Gluteus medius and minimus, inserting on the greater trochanter, abduct the proximal fragment.
- Flexion: The iliopsoas muscle, inserting on the lesser trochanter, powerfully flexes the proximal fragment.
- External Rotation: The short external rotators (piriformis, obturator internus, superior and inferior gemelli, quadratus femoris) insert on or near the greater trochanter, externally rotating the proximal fragment.
- The combined effect of these muscles results in an abducted, flexed, and externally rotated proximal fragment.
-
Distal Fragment:
- Adduction: The adductor magnus, longus, and brevis muscles pull the distal fragment medially, causing adduction.
- Shortening: The quadriceps and hamstrings, acting across the knee, contribute to shortening of the limb.
- The overall effect is a distal fragment that is adducted and shortened relative to the proximal fragment.
Understanding these deforming forces is critical for pre-operative planning and intra-operative reduction maneuvers.
Vascular Supply
The vascular supply to the subtrochanteric region is robust but can be compromised by high-energy trauma and extensive surgical dissection. The primary blood supply originates from the profunda femoris artery and its branches, including the medial and lateral circumflex femoral arteries. These vessels contribute to both the periosteal and endosteal blood flow. Maintaining soft tissue attachments, particularly the periosteum, is crucial during surgical intervention to preserve the remaining vascularity and enhance healing potential. Significant devitalization of the fracture fragments, especially with extensive comminution or stripping, increases the risk of delayed union and nonunion.
Innervation
The major nerves of concern in this region include the femoral nerve anteriorly and the sciatic nerve posteriorly. While direct injury to these nerves is uncommon with closed fractures, iatrogenic injury during surgical approaches or vigorous retraction can occur. Branches of the femoral nerve supply the vastus muscles, and care must be taken during approaches to minimize denervation.

Indications & Contraindications
Operative Indications
The vast majority of subtrochanteric fractures require operative stabilization due to the inherent instability caused by powerful muscle forces and the risk of significant displacement, malunion, and nonunion with conservative management.
- Displaced Subtrochanteric Fractures: All displaced fractures are indications for surgical intervention to restore alignment, stability, and facilitate early mobilization.
- Unstable Fracture Patterns: This includes comminuted fractures (e.g., AO/OTA 32-B3, 32-C2, C3), segmental fractures, and those with significant bone loss.
- Pathological Fractures: Due to metastatic disease, primary bone tumors, or conditions like Paget's disease. Prophylactic fixation may be indicated for impending pathological fractures with cortical involvement >50% or pain.
- Atypical Femoral Fractures (AFFs): Often treated with intramedullary nailing, even in the absence of significant displacement, due to the high risk of complete fracture propagation and the associated prodromal pain.
- Polytrauma Patients: Early stabilization is crucial for damage control orthopedics, reducing systemic inflammatory response, and facilitating overall patient management.
- Failed Non-Operative Management: While rarely attempted, progressive displacement or intractable pain would necessitate surgery.
Non-Operative Indications
Non-operative management is exceedingly rare and generally reserved for exceptional circumstances where the risks of surgery outweigh the potential benefits.
- Moribund Patient: Patients with severe, uncorrectable medical comorbidities and extremely limited life expectancy where surgical intervention would add unacceptable physiological stress.
- Non-Displaced, Stable Fractures (Rare): Extremely uncommon in the subtrochanteric region due to high deforming forces. Even minimally displaced fractures typically progress to displacement.
- Palliative Care Setting: In patients receiving end-of-life care where comfort and symptom management are the primary goals, and surgical intervention would not improve quality of life.
Table: Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | All displaced fractures | Not applicable (displacement almost always necessitates surgery) |
| Fracture Stability | Unstable fractures (e.g., comminuted, segmental) | Extremely rare: Non-displaced, highly stable (very uncommon for this location) |
| Pathology | Pathological fractures (primary, metastatic, AFFs), impending pathological fractures | Not applicable |
| Patient Condition | Medically fit patients, polytrauma patients (for damage control) | Moribund patient, severe medical comorbidities precluding surgery, end-of-life palliative care |
| Functional Goals | Restore function, facilitate early mobilization and weight bearing | Primarily for comfort care; extremely limited functional recovery expected |
| Risk-Benefit Analysis | Benefits of stability and mobility outweigh surgical risks | Surgical risks outweigh potential benefits |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is the cornerstone of successful subtrochanteric fracture management, given the complex anatomy, powerful deforming forces, and high complication rates.
Imaging and Classification
- Standard Radiographs: AP and lateral views of the entire femur, including the hip and knee, are essential. Traction-internal rotation views can help delineate fracture patterns and assess stability.
- Contralateral Femur Radiographs: Often obtained for templating to determine appropriate implant length, diameter, and anticipated neck-shaft angle, especially for intramedullary nails.
- Computed Tomography (CT) Scan: Indicated for highly comminuted fractures, articular involvement, extension into the piriformis fossa, or to characterize complex bone loss. This provides a detailed 3D understanding of the fracture pattern, aiding in reduction strategy and implant choice.
- Classification Systems: The AO/OTA classification system is widely used (32-A, 32-B, 32-C) to describe fracture morphology and guide treatment. Russell-Taylor and Seinsheimer classifications specifically address subtrochanteric fractures, focusing on involvement of the lesser trochanter and piriformis fossa, which influences nail entry point and construct stability.
Implant Selection
The choice of implant is critical and typically involves an intramedullary nail or, less commonly, a plate.
*
Intramedullary Nailing (IMN):
Considered the gold standard for most subtrochanteric fractures.
*
Cephalomedullary Nails (Reconstruction or Long):
Preferred due to their ability to provide fixation in both the femoral head/neck and the diaphyseal segment, effectively bypassing the fracture site. Long nails are often chosen for extended comminution or when prophylactic fixation of the entire diaphysis is desired (e.g., AFFs).
*
Standard Antegrade Femoral Nails:
May be used for fractures distal to the lesser trochanter or those without significant proximal comminution that would compromise cephalic screw purchase.
*
Advantages of IMN:
Load-sharing device, minimizes soft tissue stripping, biomechanically superior in resisting bending and torsional forces, allows for earlier weight-bearing.
*
Plate Fixation:
Less commonly used as primary fixation but has specific indications.
*
Dynamic Condylar Screw (DCS) / Fixed-Angle Devices:
Historically used, but technically demanding, requiring extensive soft tissue stripping, and associated with higher failure rates in this region.
*
Locking Plates (e.g., Proximal Femoral Locking Compression Plate - PF-LCP):
Can be used for specific fracture patterns, such as very proximal subtrochanteric fractures extending to the greater trochanter, failed IMN, or when an IMN entry point is contraindicated. Locking plates act as internal fixators, reducing the need for plate-bone contact and preserving periosteal blood supply.
*
Advantages of Plates:
Can address complex proximal geometry, may be preferred in certain pediatric cases.
*
Disadvantages:
Load-bearing device (prone to fatigue failure), extensive soft tissue dissection, higher risk of infection and nonunion compared to IMN.
Patient Positioning and Surgical Setup
- Positioning: The patient is typically placed supine on a fracture table. This allows for controlled traction, rotation, and abduction/adduction of the lower extremity, which are essential for reduction maneuvers. The contralateral limb is typically flexed and abducted to allow C-arm access.
- C-arm Access: Full anteroposterior (AP) and lateral fluoroscopic views of the entire femur, hip, and knee are mandatory. The C-arm should be draped and positioned to allow unobstructed views without needing to reposition the patient during the procedure.
- Traction: Manual or mechanical traction is applied to the injured leg through a foot holder. This aids in restoring length and alignment. Adjustments to traction, rotation, and abduction/adduction are made throughout the procedure.
- Preparation and Draping: Standard sterile preparation and draping from the iliac crest to the foot are performed, allowing for potential extension of the incision or conversion to an open approach if necessary.

Detailed Surgical Approach / Technique
The primary goal of surgical fixation of subtrochanteric fractures is to achieve stable fixation that withstands physiological loads, promotes healing, and allows for early mobilization. The gold standard technique is intramedullary nailing.
Intramedullary Nailing (IMN) – The Gold Standard
1. Reduction
Adequate reduction is critical before nail insertion. The characteristic displacement (flexed, abducted, externally rotated proximal fragment; adducted, shortened distal fragment) must be overcome.
*
Traction:
Mechanical traction on the fracture table helps restore length and reduce adduction.
*
Manipulation:
Manual manipulation of the limb, often involving internal rotation and gentle adduction of the distal fragment, is used to align the fragments.
*
Percutaneous Aids:
Percutaneous reduction clamps (e.g., pointed reduction clamp, Verbrugge clamp) applied through stab incisions can be invaluable for achieving and holding reduction, especially in comminuted or multi-planar fractures.
*
Cerclage Wires:
In select cases of highly comminuted or spiral fractures, one or two cerclage wires may be used to achieve provisional reduction and provide rotational control. However, caution is advised as they can impede endosteal blood supply and complicate subsequent nail removal. They should be placed meticulously to avoid soft tissue damage and kept to a minimum.
2. Incision and Entry Point
- Incision: A longitudinal incision is made over the tip of the greater trochanter, typically 3-5 cm in length, centered proximally. The fascia lata and gluteus maximus are incised, and the gluteus medius is split longitudinally in line with its fibers.
-
Entry Point:
The ideal entry point for most cephalomedullary nails is directly at or slightly medial to the tip of the greater trochanter, in line with the femoral canal on both AP and lateral views. Too lateral an entry point can lead to varus malalignment, while too medial can cause iatrogenic fracture of the femoral neck. For nails designed with a specific entry portal, strict adherence to the manufacturer's guidelines is essential.
- Piriformis Fossa vs. Greater Trochanter: Historically, piriformis fossa entry was common, but it carries a higher risk of injury to the superior gluteal artery and nerve, as well as avascular necrosis of the femoral head. Modern nails are predominantly designed for a greater trochanteric entry.

3. Guide Wire Insertion
- A guide wire (often curved or 'banana' shaped) is carefully advanced down the femoral canal. It should be placed centrally on both AP and lateral fluoroscopic views.
- Particular attention is paid to ensuring the wire crosses the fracture site without displacing fragments or creating a false passage. This may require additional reduction maneuvers.
4. Reaming
- Progressive Reaming: Flexible reamers are advanced over the guide wire to progressively enlarge the femoral canal. Reaming should be performed cautiously, increasing reamer size by 0.5 mm increments.
- Maintaining Alignment: Continuous fluoroscopic monitoring is essential to ensure concentric reaming and prevent cortical impingement or iatrogenic fracture, especially at the fracture site.
- Reamer Diameter: The canal is reamed typically 1.0 to 1.5 mm larger than the chosen nail diameter to allow for easier nail insertion and rotational stability. Over-reaming should be avoided.
5. Nail Insertion
- The chosen intramedullary nail is then inserted over the guide wire using an insertion handle.
- Gentle, controlled blows with a mallet are used to advance the nail, constantly monitoring with fluoroscopy for any signs of impingement, distraction, or displacement.
- The nail should be seated to the appropriate depth, ensuring the proximal locking screws (cephalic screws) can be placed correctly within the femoral head.

6. Proximal Locking (Cephalic Screws)
- For cephalomedullary nails, one or two lag screws are inserted into the femoral head/neck through the nail's proximal interlocking holes.
- These screws provide rotational stability and prevent cutout. Accurate placement within the femoral head is crucial, aiming for the infero-posterior quadrant on the AP view and central on the lateral view, respecting safe zones. Dynamic compression can be achieved with appropriate screw selection.

7. Distal Locking
- Distal locking screws are essential for preventing shortening and controlling rotation of the distal fragment.
- These screws are typically inserted using a targeting guide or freehand technique under fluoroscopic guidance.
- The number of screws (usually two) depends on the nail design and fracture stability. Bi-cortical purchase is preferred for maximum stability.

8. Confirmation and Closure
- Final fluoroscopic images in AP and lateral views confirm appropriate nail position, screw placement, reduction, and length.
- The guide wire is removed, and the incision is irrigated.
- The fascia, subcutaneous tissue, and skin are closed in layers.
Plate Fixation (Alternative Technique)
Plate fixation, particularly with locking plates (e.g., PF-LCP), is reserved for specific indications such as:
* Fractures extending too proximally for IMN entry.
* Severe piriformis fossa comminution.
* As salvage for failed IMN.
* Certain pediatric cases.
*
Approach:
Typically a direct lateral approach to the femur, often utilizing a subvastus or vastus-splitting technique to expose the fracture site.
*
Reduction:
Direct reduction is often necessary. Reduction clamps and sometimes temporary K-wires are used.
*
Plate Application:
The plate is contoured and applied to the lateral cortex. Locking screws are inserted bicortically, spanning the fracture with a "bridge plating" technique (relative stability) or with compression if a simple fracture pattern allows for absolute stability. Minimizing periosteal stripping is critical to preserve vascularity.
Complications & Management
Subtrochanteric fractures are associated with a high rate of complications due to the high biomechanical forces, compromised vascularity, and often complex fracture patterns.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (approx.) | Salvage Strategies |
|---|---|---|
| Nonunion | 5-20% | Revision fixation (e.g., exchange nailing, conversion to plate), autogenous bone grafting, fibular strut grafting, reamed nailing. |
| Malunion | 10-30% | Corrective osteotomy (valgus, rotational, apex anterior/posterior), limb length equalization procedures. |
| Infection | 1-5% | Debridement, irrigation, antibiotics. Deep infection: hardware removal, staged reconstruction, Girdlestone resection. Superficial: wound care, antibiotics. |
| Hardware Failure | 5-15% | Revision fixation with stronger/longer construct, plate exchange, conversion to IMN. Address underlying nonunion. |
| Avascular Necrosis (AVN) of Femoral Head | <1% (rare, often related to entry point) | Core decompression, vascularized fibula graft, total hip arthroplasty (THA). |
| Iatrogenic Fracture | <5% | Intra-operative fixation with cerclage wire or plate, conversion to longer nail/plate. |
| Nerve/Vascular Injury | <1% | Immediate surgical exploration and repair. |
| DVT/PE | 1-2% (clinical) | Anticoagulation, IVC filter in select cases. Prophylaxis is key. |
| Heterotopic Ossification | 10-20% (radiographic) | NSAID prophylaxis (post-op), radiation therapy, surgical excision (if symptomatic and mature). |
Discussion of Complications
- Nonunion: This is a formidable challenge in subtrochanteric fractures, often exacerbated by persistent distraction at the fracture site, inadequate reduction, comminution, and poor bone biology. Revision strategies often involve exchange nailing, which capitalizes on the osteogenic potential of reaming and provides a larger, stiffer implant. Bone grafting (autogenous cancellous or structural allograft) is frequently used to augment healing.
- Malunion: Incorrect rotational, angular (varus/valgus, apex anterior/posterior), or length alignment can lead to significant functional impairment, pain, abductor insufficiency, and altered gait. Varus malunion is particularly common and detrimental. Prevention through meticulous intraoperative technique and proper reduction is paramount. Symptomatic malunion may necessitate corrective osteotomy.
- Hardware Failure: Fatigue failure of implants (nail breakage, screw pullout) is typically a consequence of persistent nonunion, where the implant continues to bear excessive load over time. Revision surgery must address both the implant failure and the underlying healing problem.
- Infection: Despite prophylactic antibiotics, deep surgical site infections remain a serious complication, particularly in open fractures or prolonged procedures. Management requires aggressive debridement, appropriate antibiotic therapy, and often hardware removal or exchange, potentially in a staged manner.
- Iatrogenic Fracture: Occurring during reaming (e.g., eccentric reaming), nail insertion (e.g., mal-directed nail, forcing too large a nail), or screw placement. These often require immediate intra-operative management, such as the application of cerclage wires or a longer nail/plate.
- Atypical Femoral Fractures (AFFs): A specific type of subtrochanteric/diaphyseal fracture often associated with long-term bisphosphonate use. These fractures characteristically present with a simple transverse or short oblique pattern, localized cortical thickening, and a medial spike. They have a higher nonunion rate than typical trauma-induced subtrochanteric fractures and often require prophylactic nailing of the contralateral femur due to bilateral involvement.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring function, preventing complications, and achieving a successful outcome following subtrochanteric fracture fixation. Protocols are tailored to the individual patient, fracture stability, quality of fixation, and bone quality.
Immediate Post-Operative Period (Day 0-7)
- Pain Management: Multimodal analgesia is critical, including opioids, NSAIDs (with caution for bone healing), acetaminophen, and regional nerve blocks, to facilitate early mobilization.
- DVT Prophylaxis: Chemical (e.g., low molecular weight heparin) and mechanical (e.g., sequential compression devices) prophylaxis are initiated immediately and continued according to institutional guidelines.
- Wound Care: Regular wound checks for signs of infection or hematoma.
-
Early Mobilization:
- Bed Mobility: Instruct patient on bed mobility, transfers, and precautions.
-
Weight Bearing Status:
This is highly individualized.
- Touch-Down Weight Bearing (TDWB) / Partial Weight Bearing (PWB): Often prescribed initially for unstable fractures, comminuted fractures, or in patients with poor bone quality, to protect the construct and allow for callus formation.
- Weight Bearing As Tolerated (WBAT): May be allowed immediately for stable, well-fixed fractures (e.g., simple patterns treated with a stable IMN in good bone).
-
Physical Therapy (PT) Evaluation:
Early PT evaluation focuses on:
- Initiating gentle, active and passive range of motion (ROM) of the hip and knee (within pain limits).
- Isometric strengthening exercises for quadriceps and gluteal muscles.
- Gait training with appropriate assistive devices (walker, crutches) and adherence to prescribed weight-bearing status.
- Emphasis on maintaining independence in activities of daily living (ADLs).
Early Rehabilitation (Weeks 1-6)
- Progressive Weight Bearing: As pain decreases and radiographic signs of early healing appear (typically 4-6 weeks), weight bearing is gradually progressed from TDWB/PWB to WBAT. Clinical and radiographic assessment dictates progression.
-
Strengthening:
- Progression of hip and knee strengthening exercises (e.g., straight leg raises, hip abduction/adduction, knee flexion/extension).
- Core strengthening exercises.
- Gait Training: Continued emphasis on proper gait mechanics, reduction of assistive device reliance.
- Functional Activities: Incorporating functional movements such as stair climbing, sit-to-stand transfers.
Late Rehabilitation (Weeks 6-12 and Beyond)
- Full Weight Bearing: Typically achieved by 6-12 weeks, contingent on radiographic evidence of bridging callus and clinical stability.
- Advanced Strengthening: Progressive resistive exercises for all major muscle groups of the injured limb.
- Proprioception and Balance Training: Crucial for restoring neuromuscular control and reducing fall risk, especially in elderly patients.
- Activity-Specific Training: For younger, active patients, rehabilitation progresses to sport-specific drills or return-to-work simulations.
- Radiographic Follow-up: Serial radiographs are obtained at regular intervals (e.g., 6 weeks, 3 months, 6 months, 1 year) to monitor fracture healing, detect signs of nonunion or malunion, and assess implant integrity. Clinical union is typically achieved when the patient is pain-free with full weight bearing and shows radiographic evidence of bridging callus across at least three cortices.
Summary of Key Literature / Guidelines
Subtrochanteric fracture management has evolved significantly, with extensive literature guiding contemporary practice.
- Intramedullary Nailing as the Gold Standard: Numerous studies and systematic reviews consistently demonstrate the superiority of intramedullary nailing (specifically cephalomedullary nails) over plate osteosynthesis for the vast majority of subtrochanteric fractures. IMNs are associated with lower rates of nonunion, malunion, and hardware failure, as well as faster time to weight bearing and union. The load-sharing nature and minimally invasive application contribute to these favorable outcomes.
- Biomechanics of Fixation: The importance of achieving stable fixation within the femoral head/neck and across the diaphyseal fracture is well-established. Implants must resist both bending and torsional forces. The concept of "working length" of the nail and screw configuration is critical to prevent fatigue failure.
- Reduction Principles: Indirect reduction techniques, minimizing soft tissue stripping, are preferred to preserve the precious vascularity of the cortical bone. The use of a fracture table, manual traction, and percutaneous reduction aids are commonly cited techniques for achieving acceptable alignment.
- Atypical Femoral Fractures (AFFs): The recognition and specific management protocols for AFFs have emerged as a significant area of focus. Guidelines recommend intramedullary nailing for complete AFFs and often prophylactic nailing for symptomatic impending AFFs, even with minimal displacement, due to high risk of propagation. Discontinuation of bisphosphonate therapy, if appropriate, is also recommended.
- Role of Adjunctive Measures: The use of bone grafting for nonunions or significant bone defects is a well-accepted practice. The judicious use of cerclage wires for comminution, while potentially affecting endosteal blood supply, can be beneficial for achieving and maintaining reduction in specific complex patterns.
- Outcomes and Complications: While outcomes have improved with modern techniques, subtrochanteric fractures still carry a significant complication burden, particularly nonunion and malunion. These are often attributable to persistent deforming muscle forces, fracture comminution, and suboptimal surgical technique.
- Guidelines: Major orthopedic trauma associations, such as the AO Foundation, provide comprehensive principles and surgical techniques that form the basis of current practice. These emphasize meticulous pre-operative planning, proper entry point, anatomical reduction, and stable fixation.
In conclusion, the successful management of subtrochanteric femoral fractures hinges upon a profound understanding of their unique anatomy and biomechanics, meticulous pre-operative planning, precise surgical execution, and diligent post-operative rehabilitation. Intramedullary nailing remains the treatment of choice, offering superior biomechanical stability and biological advantages, thereby facilitating early mobilization and improved patient outcomes, though vigilant monitoring for complications remains paramount.
You Might Also Like