Acetabular Revision: Solving Challenges Post Two-Stage Arthroplasty

Key Takeaway
For anyone wondering about Acetabular Revision: Solving Challenges Post Two-Stage Arthroplasty, A **title acetabular revision** is a complex procedure addressing issues like septic loosening, dislocation, and significant osteolysis in total hip arthroplasty. For a 71-year-old male with a dislocated left THA due to infection and periacetabular bone loss, treatment involved a two-stage exchange followed by revision with a press-fit hemispherical cup and screw fixation.
Acetabular Revision: Solving Challenges Post Two-Stage Arthroplasty
Introduction & Epidemiology
Two-stage exchange arthroplasty remains the gold standard for the treatment of chronic periprosthetic joint infection (PJI) of the hip. While highly effective, a subset of patients will present for subsequent acetabular revision due to persistent or recurrent infection, aseptic loosening, component malposition, or progressive bone loss following the reimplantation stage. Addressing these challenges requires a sophisticated understanding of complex acetabular reconstruction. The increasing incidence of total hip arthroplasty (THA) coupled with an aging population and higher rates of comorbidities contributes to a rising burden of PJI, subsequently increasing the demand for complex revision surgeries.
PJI is a devastating complication, with reported incidences ranging from 0.5% to 2% for primary THA and significantly higher, up to 10% or more, for revision procedures. Following a successful two-stage exchange, approximately 5-10% of patients may still experience treatment failure, necessitating further intervention. This failure can stem from a variety of causes, including inadequate debridement during the first stage, biofilm persistence, suboptimal antibiotic delivery, or the development of aseptic mechanical complications post-reimplantation. Persistent deep infection is a primary concern, but mechanical failure of the acetabular component due to underlying bone deficiency, improper component selection, or technical errors during reimplantation also mandates revision. The decision-making process for these complex cases is often multifactorial, requiring a comprehensive diagnostic approach and a tailored surgical strategy.
Surgical Anatomy & Biomechanics
A thorough understanding of acetabular anatomy and biomechanics is paramount for successful acetabular revision surgery. The acetabulum is a complex structure formed by the ilium, ischium, and pubis, articulating with the femoral head. Its integrity is crucial for load bearing and hip stability.
Key Anatomical Considerations:
- Pelvic Columns: The anterior (iliopectineal) and posterior (ilioischial) columns provide structural support. Defects in these columns significantly compromise acetabular stability and require specific reconstructive strategies.
- Acetabular Quadrants: The superior, anterior, posterior, and inferior quadrants help delineate bone loss patterns.
-
Bone Stock Assessment:
The Paprosky classification system (Type I-IV) is widely utilized to categorize acetabular bone defects based on the amount of remaining host bone, specifically the integrity of the rim and columns.
- Type I: Minimal bone loss, intact rim and columns.
-
Type II:
Significant cavitary defects, intact columns.
- IIA: Superior migration, intact ischium.
- IIB: Medial migration, intact ischium.
- IIC: Global cavitary defect.
-
Type III:
Extensive bone loss involving rim and columns.
- IIIA: >50% host bone contact for uncemented cup, often superior-posterior column defect.
- IIIB: <50% host bone contact for uncemented cup, often extensive column and medial wall involvement.
-
Type IV:
Pelvic discontinuity (complete separation of the acetabulum from the rest of the pelvis).
Proper assessment guides implant selection and reconstruction technique.
-
Neurovascular Structures:
Proximity to critical structures dictates surgical approach and dissection.
- Superior Gluteal Nerve and Artery: Superior to the piriformis, vulnerable during superior dissection, especially with revision via posterior or modified lateral approaches.
- Sciatic Nerve: Courses posterior to the acetabulum, susceptible to injury during posterior approach, component insertion (screws), or limb lengthening.
- Femoral Nerve and Vessels: Anterior to the acetabulum, at risk during anterior approaches or medial wall perforation.
- Obturator Nerve and Vessels: Medial to the acetabulum, vulnerable with excessive medial reaming or perforation.
- Muscle Attachments: The gluteal muscles (maximus, medius, minimus), iliopsoas, and adductors contribute to hip function and stability. Their integrity and reattachment are critical for functional recovery.
Biomechanical Considerations:
- Cup Position and Orientation: Restoration of appropriate inclination (40° ± 10°) and anteversion (20° ± 10°) is crucial to prevent impingement and dislocation. In revision, achieving ideal positioning can be challenging due to bone loss and scarring.
- Restoration of Hip Mechanics: Re-establishing native hip center, femoral offset, and leg length is vital for optimal abductor tension, gait mechanics, and to minimize hip reaction forces. Discrepancies can lead to limp, pain, or increased wear.
- Load Sharing vs. Stress Shielding: Revision constructs should ideally encourage load sharing with host bone to promote osteointegration and prevent stress shielding. This is particularly relevant for porous-coated implants and bone graft reconstructions.
- Construct Stability: The primary goal is achieving stable fixation, either biological (press-fit with porous coating) or mechanical (screws, cages, cement). Extensive bone defects require augmented fixation strategies to ensure initial stability for biological integration.
- Implant Selection: The choice of implant (e.g., jumbo cups, highly porous implants, anti-protrusio cages, custom triflange components) must match the defect morphology and biomechanical demands.
Indications & Contraindications
The decision for acetabular revision following a two-stage arthroplasty is complex and requires careful consideration of both patient factors and local hip conditions.
Indications for Operative Intervention:
- Persistent or Recurrent Periprosthetic Joint Infection (PJI): This is a primary indication, confirmed by positive cultures from synovial fluid or tissue, elevated inflammatory markers (ESR, CRP), or evidence of purulence. This often necessitates further debridement, spacer exchange, or definitive reimplantation if not done previously.
- Aseptic Loosening of the Acetabular Component: Manifests as progressive pain, implant migration, or radiographic evidence of loosening (e.g., progressive lucency, component migration).
- Significant Osteolysis with Bone Loss: Progressive bone resorption around the component, often secondary to particulate wear debris, threatening the structural integrity of the acetabulum.
- Periprosthetic Acetabular Fracture: Either intra-operative during component insertion or post-operative due to trauma or bone fatigue.
- Component Malposition: Leading to recurrent dislocation, impingement, restricted range of motion, or accelerated wear.
- Painful Non-union of Previous Reconstruction: Failure of an acetabular defect reconstruction to integrate, resulting in pain and instability.
- Mechanical Failure of Previous Reconstruction: Breakage of a revision cage or structural allograft collapse.
Contraindications for Operative Intervention:
- Active Systemic Infection Not Controlled: Uncontrolled systemic sepsis or active infection elsewhere in the body typically precludes elective revision surgery.
- Extensive, Irreconstructible Bone Loss: In cases of severe Paprosky Type IIIB or Type IV defects, where reconstruction is deemed impossible or offers minimal chance of success, palliation or limb salvage might be considered.
- Prohibitive Surgical Risk: Severe comorbidities (e.g., end-stage cardiac, pulmonary, or renal disease, uncontrolled diabetes) that place the patient at extremely high risk for major surgery and anesthesia.
- Insufficient Patient Compliance: Inability or unwillingness to adhere to post-operative weight-bearing restrictions, activity modifications, or rehabilitation protocols, which are critical for success in complex revision cases.
- Neurovascular Compromise Precluding Safe Surgery: Pre-existing severe peripheral neuropathy or vascular disease that would make the surgical approach or subsequent recovery unduly hazardous.
- Charcot Arthropathy of the Hip: Although rare, it can lead to rapidly destructive arthropathy and poor implant fixation.
Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Infection | Persistent/recurrent culture-positive PJI | Suppressed infection with oral antibiotics (rare, selected cases) |
| Mechanical Failure | Aseptic loosening, component migration | Asymptomatic radiographic lucency, stable components |
| Periprosthetic fracture, component breakage | Stable, non-displaced fractures without implant compromise | |
| Bone Loss | Significant progressive osteolysis, bone stock compromise | Minimal, non-progressive osteolysis without mechanical symptoms |
| Instability | Recurrent dislocation due to component malposition | Infrequent dislocation manageable with bracing/precautions |
| Pain/Function | Disabling pain, severe functional limitation | Mild, manageable pain with conservative measures |
| Patient Factors | Medically fit, good surgical candidate, compliant | High surgical risk, non-compliant, significant comorbidities |
| Irreconstructible Defects | N/A | Palliation, limb salvage, Girdlestone-type arthroplasty |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful acetabular revision, particularly after a two-stage exchange for PJI, where scarring and altered anatomy are anticipated.
Diagnostic Workup:
-
Detailed History and Physical Examination:
- Thorough history of previous surgeries, including types of components, infection workup, antibiotic regimens, and prior complications.
- Assess for ongoing signs of infection (fever, fistula, persistent drainage).
- Evaluate hip range of motion, stability, leg length discrepancy, and neurovascular status.
-
Imaging:
-
Standard Radiographs:
AP pelvis, true lateral (cross-table or frog-leg), Judet views (obturator oblique, iliac oblique) are essential to assess component position, signs of loosening (lucent lines, cement mantle integrity), osteolysis, and column integrity.
-
Computed Tomography (CT) Scan with Metal Artifact Reduction (MAR):
Crucial for detailed assessment of bone stock (Paprosky classification), defect morphology, pelvic column integrity, and presence of pelvic discontinuity. It helps quantify bone loss and plan for specific reconstructive strategies.
- Magnetic Resonance Imaging (MRI) with Metal Suppression Sequences: May be beneficial to evaluate soft tissue inflammation, pseudotumors, or occult abscesses if infection is suspected but radiographs are inconclusive, however, its utility can be limited by artifact.
- Bone Scintigraphy / PET Scan: Occasionally used for further investigation of infection or loosening, but often supplanted by advanced CT/MRI.
-
Standard Radiographs:
AP pelvis, true lateral (cross-table or frog-leg), Judet views (obturator oblique, iliac oblique) are essential to assess component position, signs of loosening (lucent lines, cement mantle integrity), osteolysis, and column integrity.
-
Infection Workup (if recurrence suspected):
- Laboratory Tests: Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein (CRP).
- Synovial Fluid Aspiration: Crucial for cell count and differential, culture (aerobic/anaerobic, fungal, atypical organisms), alpha-defensin, and leukocyte esterase testing. Aspiration should ideally be performed after a recommended antibiotic holiday (2-4 weeks).
- Peri-prosthetic Tissue Biopsy: Intra-operative biopsies for histopathology and culture remain the gold standard.
-
Pre-operative Templating:
- Utilize digital templating software with calibrated radiographs or CT scans.
- Determine size and type of planned acetabular component (e.g., jumbo cup, highly porous, cage, custom component).
- Plan for bone graft (autograft, allograft) or augmentation components (wedges, sleeves).
- Anticipate femoral component revision if indicated.
- Consider specific hardware for pelvic discontinuity (e.g., plates, screws for column fixation).
Pre-operative Optimization:
- Medical Co-morbidities: Optimize cardiac, pulmonary, renal, and endocrine status. Patients undergoing complex revision often have multiple comorbidities.
- Nutritional Status: Assess and optimize albumin, prealbumin, and vitamin D levels, as malnutrition can impair wound healing and infection resistance.
- Smoking Cessation: Encourage cessation for at least 6-8 weeks pre-operatively to improve wound healing and reduce complications.
- Dental Clearance: To minimize sources of bacteremia.
- Antibiotic Prophylaxis: Administer appropriate intravenous antibiotics typically 30-60 minutes prior to incision, adjusted based on prior cultures and local antibiograms.
Patient Positioning:
-
Lateral Decubitus Position:
Most commonly used for posterior and modified lateral (Hardinge) approaches.
- Pros: Excellent visualization of the acetabulum, easy access to the femur. Allows for controlled disarticulation and soft tissue release.
- Cons: Potential for brachial plexus injury if not positioned correctly; limb length assessment can be challenging.
-
Supine Position:
Preferred for anterior approaches (e.g., ilioinguinal) or if an extended iliofemoral approach is anticipated for extensive anterior column defects.
- Pros: Good for true AP pelvis intra-op imaging, accurate leg length measurement.
- Cons: Limited posterior exposure; requires significant patient manipulation for posterior acetabular work.
- Padding: Meticulous padding of all pressure points (axilla, malleoli, knees) to prevent nerve palsies and skin breakdown.
- Vascular Access & Monitoring: Secure IV access, arterial line for blood pressure monitoring, and central venous access may be considered in high-risk patients.
- Urinary Catheterization: Routine to monitor urine output and keep the bladder decompressed.
- Image Intensifier (Fluoroscopy) Setup: Ensure clear anterior-posterior and lateral views of the hip and pelvis are achievable without repositioning the patient.
Detailed Surgical Approach / Technique
Revision acetabular surgery after two-stage arthroplasty for PJI presents unique challenges due to scarring, altered tissue planes, and often significant bone loss. A systematic, meticulous approach is essential.
General Principles for Revision:
- Re-utilize Existing Incision: Whenever possible, an existing incision should be utilized and extended as needed. Scar tissue can make dissection challenging.
- Careful Dissection: Due to scarring, neurovascular structures may be tethered or displaced. Sharp dissection through fibrous tissue is often necessary, avoiding indiscriminate blunt dissection.
-
Explant of Retained Components:
If a spacer or prior components (cemented or uncemented) are present, careful extraction is required. For cement spacers, often osteotomies or careful removal with osteotomes are needed.

- Meticulous Debridement: All fibrous, necrotic, or infected tissue, as well as any foreign material, must be meticulously debrided. This includes removal of pseudocapsule and any retained cement or loose debris. Intra-operative cultures (at least 5-7 samples) are critical if infection is suspected.
-
Assessment of Bone Loss:
After debridement, a comprehensive assessment of the acetabular bone defect is performed, confirming or refining the pre-operative Paprosky classification.

Common Approaches and their Indications in Revision:
-
Posterior Approach (Kocher-Langenbeck):
Most common. Offers excellent exposure of the posterior column and posterior superior acetabulum.
- Indications: Most Paprosky Type I, II, and IIIA defects. Suitable for explantation and cup revision.
- Challenges: Risk of sciatic nerve injury, particularly with posterior column plating or extensive medialization.
-
Anterolateral Approach (Watson-Jones / Hardinge Modified Lateral):
Provides good access to the anterior and superior acetabulum.
- Indications: Often chosen for anterior-superior defects, or if a previous posterior approach failed due to hip instability. Potentially lower dislocation rates.
- Challenges: Risk to superior gluteal nerve (abductor dysfunction), often requires osteotomy of the greater trochanter for optimal exposure.
-
Extended Trochanteric Osteotomy (ETO):
A powerful extensile approach that allows for circumferential visualization of the acetabulum and femoral canal.
- Indications: Complex acetabular reconstructions (e.g., Paprosky Type IIIB, Type IV pelvic discontinuity, massive allografts), difficult femoral component removal.
- Challenges: Prolonged operative time, potential for non-union of the osteotomy, abductor weakness.
-
Ilioinguinal / Iliofemoral Approach:
Reserved for extensive anterior column or anterior-superior defects, particularly in cases of pelvic discontinuity requiring anterior plate fixation.
- Indications: Paprosky Type IV defects, anterior column fractures, severe anterior bone loss.
- Challenges: Highly invasive, significant risk to femoral nerve and vessels, lateral femoral cutaneous nerve, and genitofemoral nerve. Requires extensive soft tissue dissection.
Reconstruction Strategies for Acetabular Bone Defects:
-
Cavitary Defects (Paprosky Type I, IIA/B/C):
-
Hemispherical Porous-Coated Cups:
Standard uncemented cups can be used if adequate host bone contact (typically >50%) and stable press-fit are achievable. Reaming to healthy, bleeding bone is critical.
- Impaction Bone Grafting: Can fill contained cavitary defects to restore bone stock, often used with cemented liners or cages. Autograft or allograft cancellous bone chips are impacted to create a stable bed.
- Augmentation with Wedges/Sleeves: Modular metallic wedges or sleeves can address segmental bone loss and improve cup seating. These are typically porous-coated and screwed into the remaining host bone.
-
Highly Porous Metals (Trabecular Metal, Porous Titanium):
These implants offer high friction coefficients and excellent ingrowth potential, making them highly effective for cavitary and some segmental defects. They can be manufactured in various shapes (hemispherical, oblong, augments) to match defect morphology.

-
Hemispherical Porous-Coated Cups:
Standard uncemented cups can be used if adequate host bone contact (typically >50%) and stable press-fit are achievable. Reaming to healthy, bleeding bone is critical.
-
Segmental Defects (Paprosky Type IIIA/B):
- Jumbo Cups: Larger diameter hemispherical cups (>60mm) can bypass smaller segmental defects, provided sufficient host bone contact is achieved.
-
Metal Augments:
Pre-fabricated porous metal augments (e.g., dome, posterior, column) are designed to fill specific segmental defects and restore the acetabular rim. These are screwed to the host bone and provide a stable base for a standard or jumbo cup.

-
Antiprotrusio Cages/Rings (e.g., Burch-Schneider, Kerboull):
Used for extensive medial wall defects, superior migration, or column deficiencies. These cages are typically cemented or screw-fixated to the intact peripheral bone, and then a cemented cup is inserted into the cage. Bone graft is often packed around and within the cage.


- Structural Allografts: For very large segmental defects (e.g., superior dome, posterior column). These are shaped to fit the defect and fixed with screws and/or plates, providing structural support. A standard cup is then implanted into the allograft/host bone complex. Risk of allograft non-union or resorption exists.
-
Pelvic Discontinuity (Paprosky Type IV):
- This is the most challenging defect, involving complete separation of the acetabulum from the rest of the innominate bone.
- Principles: Re-establish continuity, stabilize the columns, reconstruct the acetabular component.
-
Techniques:
- Column Plating: Anterior and/or posterior column plates are used to fix the fractured fragments, restoring the integrity of the pelvic ring.
- Cages with Supplemental Fixation: Antiprotrusio cages or custom triflange components are often used in conjunction with column plating.
-
Custom Triflange Components:
CAD/CAM custom-designed implants, based on pre-operative CT scans, offer a precise fit for complex, unique defects, providing direct fixation to the remaining intact bone of the ilium, ischium, and pubis. These are particularly useful in Paprosky Type IIIB and Type IV defects.


- Combined Techniques: Often a combination of structural allografts, metal augments, and cages or custom components is necessary.
Component Insertion and Final Steps:
- Trial Reduction: After the acetabular component is secured, trial reduction is performed to assess stability, range of motion, and leg length.
- Definitive Head and Liner: Select appropriate head size and length, and liner type (e.g., highly cross-linked polyethylene, dual mobility) based on stability requirements and patient activity level. Dual mobility liners are frequently considered in revision cases due to their enhanced stability and reduced dislocation rates.
- Femoral Component: If the femoral component is well-fixed and functioning, it is retained. If loose, infected, or poorly positioned, it is also revised.
-
Closure:
Meticulous hemostasis. Layered closure of soft tissues. Drain placement is often indicated, especially in extensive reconstructions or if hematoma formation is a concern.

Complications & Management
Acetabular revision following a two-stage arthroplasty carries a higher risk of complications compared to primary THA due to extensive surgery, compromised host tissues, and often, a history of infection.
| Complication Category | Incidence | Salvage Strategies ## Post-Operative Rehabilitation Protocols
The rehabilitation protocol following complex acetabular revision is critical for optimizing outcomes and preventing complications. It must be individualized based on the stability of the reconstruction, quality of host bone, soft tissue status, and patient comorbidities. Close communication between the surgeon and physical therapist is essential.
General Principles:
- Protection of Reconstruction: Avoid excessive stress on the healing bone-implant interface and any reconstructed columns or grafts.
- Early, Controlled Motion: Prevent stiffness and preserve muscle strength while respecting weight-bearing precautions.
- Progressive Weight-Bearing: Gradually increase load on the limb as bone ingrowth and healing progress.
- Patient Education: Crucial for adherence to precautions and exercises.
Phase 1: Immediate Post-operative (Day 0 - 6 weeks)
- Goals: Protect the surgical site, manage pain and swelling, initiate early motion, prevent complications.
-
Weight-Bearing (WB):
- Protected Weight-Bearing: Often toe-touch (TDWB) or partial weight-bearing (PWB) (10-25% body weight) on the operated limb, especially for extensive reconstructions (cages, custom implants, structural allografts, Paprosky Type IIIB/IV).
- Full Weight-Bearing (FWB): May be allowed earlier for stable, non-augmented hemispherical cup revisions in excellent bone stock (Paprosky Type I/IIA).
- Ambulation: Initially with crutches or walker, with strict adherence to WB restrictions.
-
Range of Motion (ROM):
- Hip Precautions: Maintain strict hip precautions (e.g., avoid hip flexion >90°, adduction past midline, internal rotation) as per surgical approach, to minimize dislocation risk.
- Gentle Passive/Active-Assist ROM: Within protected ranges. Avoid aggressive stretching.
-
Therapeutic Exercises:
- Ankle Pumps and Foot Circles: To prevent deep venous thrombosis (DVT).
- Isometric Quadriceps and Gluteal Sets: To maintain muscle tone.
- Gentle Hip Abduction/Adduction Isometrics: If appropriate for the approach and fixation.
- Upper Extremity Strengthening: For ambulation aid use.
- Pain Management: Multimodal analgesia.
- DVT Prophylaxis: Pharmacological and mechanical.
Phase 2: Intermediate (6 weeks - 3 months)
- Goals: Increase weight-bearing, improve ROM, restore muscle strength, progress gait.
-
Weight-Bearing:
- Progressive Increase: Gradual transition to PWB (50%) or FWB as tolerated, based on radiographic evidence of healing and stability, and surgeon's discretion.
- Assistive Devices: Progress from two crutches to one crutch or cane.
-
Range of Motion:
- Continue Precautions: Maintain hip precautions, though some surgeons may relax them for specific constructs (e.g., dual mobility).
- Active ROM: Progress active hip flexion, extension, abduction, and adduction.
-
Therapeutic Exercises:
- Progressive Strengthening: Focus on hip abductors, extensors, and core musculature (e.g., sidelying abduction, bridging, mini-squats within limits).
- Gait Training: Emphasize normal heel-to-toe pattern, minimize Trendelenburg gait.
- Stationary Bicycle: With low resistance and elevated seat, can be introduced to improve ROM and endurance.
Phase 3: Advanced (3 months - 6+ months)
- Goals: Maximize strength, endurance, balance, and functional independence.
-
Weight-Bearing:
- Full Weight-Bearing: All patients should be FWB without assistive devices unless specific issues persist.
-
Range of Motion:
- Restore Full Functional ROM: Within the limits of the prosthesis and soft tissue healing.
- Gradual Relaxation of Precautions: Usually by 3-6 months, depending on stability and patient risk factors.
-
Therapeutic Exercises:
- Advanced Strengthening: Incorporate resistance bands, light weights, balance exercises (e.g., single-leg stance).
- Proprioception Training: Enhance neuromuscular control.
- Functional Activities: Stair climbing, negotiating uneven surfaces.
- Low-Impact Activities: Swimming, cycling, elliptical training. Avoid high-impact sports.
- Long-Term Monitoring: Regular follow-up for radiographic assessment of implant integration and wear, and to monitor for late complications.
Specific Considerations for Extensive Reconstructions (Cages, Custom Implants, Pelvic Discontinuity):
These cases often require more prolonged protected weight-bearing (3-6 months or more) to allow for bone graft incorporation and implant osteointegration. Radiographic evidence of healing is critical before advancing weight-bearing. Close communication with the surgeon regarding individual patient status is paramount.
Summary of Key Literature / Guidelines
Acetabular revision following two-stage arthroplasty, particularly for PJI, represents one of the most challenging areas in orthopedic surgery. The literature highlights several key principles and evolving strategies to optimize outcomes.
-
Diagnosis of PJI: The Musculoskeletal Infection Society (MSIS) criteria and newer criteria incorporating alpha-defensin and leukocyte esterase continue to be the standard for PJI diagnosis. Accurate diagnosis is critical to avoid unnecessary revision or inappropriate management. Studies consistently show that synovial fluid analysis (cell count, differential, culture, alpha-defensin) is essential, with an antibiotic holiday prior to aspiration improving sensitivity.
-
Efficacy of Two-Stage Exchange: While acknowledged as the gold standard for chronic PJI, success rates vary, typically ranging from 85-95%. A small but significant proportion of patients will face persistent infection or mechanical failure, necessitating further revision. The choice of antibiotics, duration of treatment, and thoroughness of debridement during the first stage significantly impact the success of the two-stage protocol.
-
Acetabular Bone Defect Classification and Reconstruction: The Paprosky classification remains the universally accepted system for guiding acetabular reconstruction.
- Highly Porous Metals (Trabecular Metal, Porous Titanium): Numerous studies support the use of highly porous acetabular components for Paprosky Type II and IIIA defects. Their high frictional coefficient and excellent osteointegration properties demonstrate superior stability and comparable long-term survival to primary THA in some series. They have largely supplanted structural allografts for many contained and segmental defects due to lower rates of non-union and resorption.
- Antiprotrusio Cages/Rings: Cages remain a viable option for Paprosky Type IIIB defects and some Type IV cases, often in conjunction with impaction bone grafting. Long-term results demonstrate reasonable survivorship, though complications such as aseptic loosening and cage fracture can occur. Careful technique, including appropriate tensioning and secure fixation to intact host bone, is crucial.
- Custom Triflange Components: For Paprosky Type IIIB and IV defects, especially pelvic discontinuity, custom triflange components have shown promising results in specialist centers. They offer excellent conformity and direct fixation to remaining host bone, potentially reducing aseptic loosening rates compared to traditional cages, but require extensive pre-operative planning and specialized manufacturing. Long-term data is still accumulating, but mid-term results are encouraging.
- Pelvic Discontinuity Management: Consensus generally favors restoration of pelvic ring integrity via column fixation (plates/screws) in addition to reconstruction of the acetabulum with a cage, custom triflange, or modular components with augments. Outcomes are significantly worse than for less severe defects.
-
Role of Dual Mobility: Dual mobility acetabular components have gained significant traction in revision THA, particularly in cases with high dislocation risk (e.g., abductor deficiency, previous instability, revision for infection). Meta-analyses consistently demonstrate a reduced dislocation rate compared to conventional bearings in revision settings, albeit with specific concerns about intraprosthetic dislocation (rare) and polyethylene wear (long-term data evolving).
-
Complication Management: Dislocation, persistent infection, and aseptic loosening remain the leading causes of failure after revision acetabular surgery.
- Dislocation: May necessitate further revision, dual mobility conversion, or constrained liners.
- Recurrent PJI: Often requires repeat two-stage exchange, debridement and implant retention (DAIR) in highly selected cases, or in salvage situations, Girdlestone resection arthroplasty or permanent antibiotic suppression.
- Neurovascular Injury: Careful surgical technique, intra-operative neuromonitoring (if available), and prompt recognition are paramount.
-
Multidisciplinary Approach: The complexity of these cases underscores the importance of a multidisciplinary team, including orthopedic surgeons, infectious disease specialists, rehabilitation physicians, and dedicated nursing staff, to optimize patient selection, pre-operative optimization, surgical execution, and post-operative care.
In conclusion, acetabular revision post two-stage arthroplasty requires a sophisticated armamentarium of diagnostic tools, surgical techniques, and reconstructive implants. The judicious application of these resources, guided by established classification systems and emerging evidence, is essential to achieve durable and functional outcomes for these challenging patients.
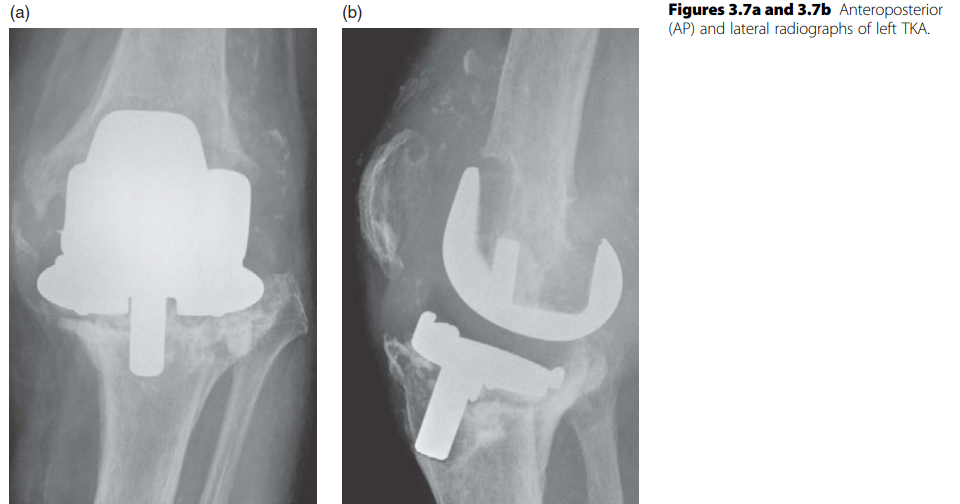
Clinical & Radiographic Imaging

You Might Also Like