Acute Compartment Syndrome Diagnosis in Open Tibial Fractures: A Clinical Case Study
Key Takeaway
Acute compartment syndrome after tibial fracture presents with pain disproportionate to injury, unremitting despite analgesia. Key red flags include tense, 'wood-hard' compartments, severe pain on passive stretch, progressive neurological deficits (weakness, paresthesia), and evolving vascular compromise (diminished pulses, delayed capillary refill). Early recognition is vital.
Patient Presentation & History
A 28-year-old previously healthy male presented to the emergency department following a high-energy motor vehicle collision. He was an unrestrained driver whose vehicle struck a tree head-on at an estimated speed of 70 km/h. On scene, he was extricated by emergency services. Initial ATLS assessment revealed a GCS of 15, stable vital signs (HR 88 bpm, BP 125/78 mmHg, RR 16, SaO2 99% on room air). He complained of severe right lower leg pain. There was no history of significant medical comorbidities, allergies, or prior surgeries. His social history was non-contributory other than occasional alcohol use.
Initial primary survey identified an obvious deformity of the right lower leg with a 2 cm transverse laceration over the anterior tibia, bleeding actively. There was significant swelling noted. Distal pulses were palpable, and sensation was grossly intact. A provisional diagnosis of an open right tibial shaft fracture was made. Secondary survey was otherwise unremarkable, with no other acute traumatic injuries identified.
Upon arrival to the ED, he reported excruciating pain in his right lower leg, rated 10/10 on the Visual Analog Scale (VAS), despite receiving 10 mg IV morphine en route. He described the pain as deep, throbbing, and constant, unrelieved by repositioning. This pain was noticeably worse than his initial assessment in the field.
Clinical Examination
Upon arrival, the patient was alert and oriented but in significant distress due to pain.
The right lower extremity examination revealed:
Inspection
- Gross Deformity: Marked angulation and swelling of the mid-diaphyseal region of the right tibia.
- Skin: A 2 cm transversely oriented laceration over the anterior aspect of the distal third of the tibia, actively weeping serosanguinous fluid. Surrounding skin was tense, shiny, and erythematous. No blistering or ecchymosis initially, but swelling was rapidly progressive.
- Compartment Assessment: The anterior and lateral compartments of the right lower leg appeared overtly tense and firm to palpation, particularly compared to the contralateral limb and the posterior compartments. The skin over these compartments felt stretched.
Palpation
- Tenderness: Exquisite tenderness along the entire length of the tibia, specifically exacerbated by palpation over the anterior and lateral compartments.
- Compartment Turgor: The anterior compartment felt "wood-hard" and non-yielding to deep palpation. The lateral compartment was also firm. The superficial and deep posterior compartments, while swollen, were less tense.
-
Pain with Passive Stretch:
- Anterior compartment: Severe, excruciating pain with passive plantarflexion of the ankle and passive flexion of the toes (stretches the tibialis anterior, EHL, EDL). This was disproportionate to the movement.
- Lateral compartment: Severe pain with passive inversion of the ankle (stretches the peroneals).
- Posterior compartments: Mild to moderate pain with passive dorsiflexion of the ankle and passive extension of the toes, but notably less severe than the anterior and lateral compartments.
- Temperature: Skin was warm to touch.
Range of Motion (ROM)
- Active ROM of the ankle and toes was severely limited due to pain, especially for dorsiflexion and eversion.
- Passive ROM was restricted and elicited disproportionate pain as described above.
Neurological & Vascular Assessment
-
Motor Function:
- Anterior compartment: Weak dorsiflexion of the ankle (tibialis anterior - deep peroneal nerve) and toe extension (EHL, EDL - deep peroneal nerve), patient unable to overcome gravity. Initially 3/5, rapidly declining to 1/5.
- Lateral compartment: Weak eversion of the ankle (peroneals - superficial peroneal nerve). Initially 3/5, declining to 2/5.
- Superficial posterior compartment: Plantarflexion (gastroc/soleus - tibial nerve) initially 4/5, later 3/5.
- Deep posterior compartment: Toe flexion (FHL, FDL - tibial nerve) initially 4/5, later 3/5.
-
Sensory Function:
- Deep Peroneal Nerve: Numbness and paresthesia noted in the first web space (between 1st and 2nd toes), evolving from "pins and needles" to definite hypesthesia.
- Superficial Peroneal Nerve: Decreased sensation over the dorsum of the foot, lateral aspect.
- Sural/Saphenous/Tibial Nerves: Sensation remained grossly intact in their respective distributions, although some generalized decreased sensation distal to the injury was noted due to swelling.
-
Vascular Assessment:
- Pulses: Dorsalis pedis and posterior tibial pulses were initially palpable and strong (2+), but with increasing tension in the compartments, they became difficult to palpate and were eventually only weakly dopplerable.
- Capillary Refill: Initially brisk (<2 seconds), but progressively slowed to 3-4 seconds in the toes of the affected foot.
- Skin Color/Temperature: Toes initially pink and warm, later slightly pale with mild mottling.
Summary of Clinical Progression: The key "red flag" here was the pain out of proportion to the injury and unresponsive to analgesia, coupled with rapidly increasing tenseness of the anterior and lateral compartments, and progressive neurological deficits (weakness, paresthesia in deep and superficial peroneal distributions). The evolving vascular signs (diminished pulses, delayed cap refill) further heightened suspicion.
Imaging & Diagnostics
Initial Radiographs
- Anteroposterior (AP) and lateral views of the right tibia and fibula were obtained.
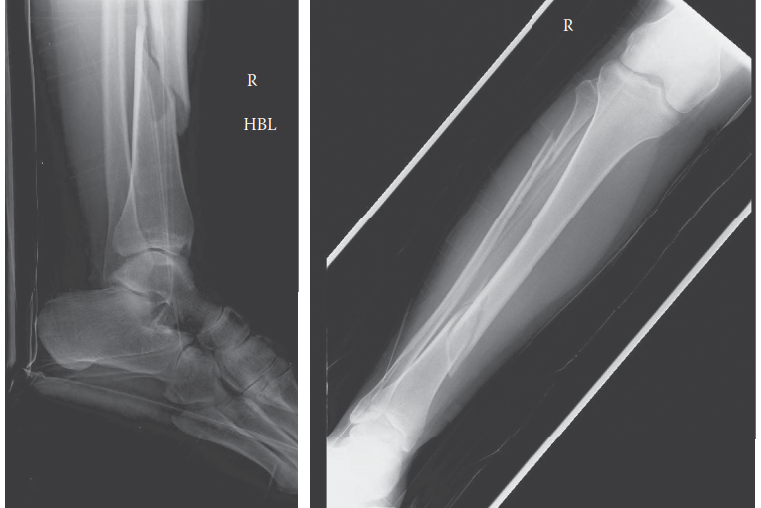
- Findings: A comminuted, spiral oblique fracture of the mid-diaphysis of the right tibia with significant displacement and angulation. The fibula was intact.
- Classification: Gustilo-Anderson Type II open fracture given the 2 cm laceration and moderate soft tissue damage. There was no gross contamination evident on initial inspection, but the wound edges were somewhat crushed.
Figure 1: AP radiograph of the right tibia and fibula demonstrating a comminuted spiral oblique mid-diaphyseal tibia fracture.
Compartment Pressure Measurement
Given the strong clinical suspicion for acute compartment syndrome, compartment pressures were measured using a Stryker STIC device. The patient was pre-medicated with local anesthetic at the insertion sites, though this does not impact true compartment pressure readings.
*
Technique:
Measurements were taken in the anterior, lateral, superficial posterior, and deep posterior compartments of the right lower leg. A 20-gauge needle was connected to the pressure transducer and inserted into each compartment, ensuring proper placement.
*
Results:
* Anterior Compartment: 65 mmHg
* Lateral Compartment: 58 mmHg
* Superficial Posterior Compartment: 32 mmHg
* Deep Posterior Compartment: 38 mmHg
*
Diastolic Blood Pressure:
The patient's diastolic blood pressure at the time of measurement was 70 mmHg.
*
Delta Pressure Calculation:
* Anterior Compartment Delta P = DBP - Compartment Pressure = 70 - 65 = 5 mmHg
* Lateral Compartment Delta P = DBP - Compartment Pressure = 70 - 58 = 12 mmHg
*
Interpretation:
A delta pressure (diastolic blood pressure minus compartment pressure) of less than 30 mmHg is highly indicative of compartment syndrome. With delta pressures of 5 mmHg and 12 mmHg in the anterior and lateral compartments respectively, the diagnosis of acute compartment syndrome was unequivocally confirmed. Absolute pressures >30-40 mmHg are also concerning, especially in normotensive patients.
Other Diagnostics
- Laboratory Tests: Routine blood work including CBC, metabolic panel, coagulation profile were obtained. Hemoglobin was stable, creatinine and electrolytes within normal limits.
- Arterial Duplex Ultrasound: Considered but deferred due to the urgency for fasciotomy. Clinical signs of diminished pulses and delayed capillary refill, combined with high compartment pressures, mandated immediate surgical intervention.
Differential Diagnosis
The acute presentation of severe leg pain and swelling following trauma, particularly with an open fracture, warrants consideration of several critical differential diagnoses. A detailed comparison is crucial for accurate and timely management.
| Feature | Acute Compartment Syndrome (ACS) | Deep Vein Thrombosis (DVT) | Cellulitis / Infection (Post-Trauma) | Direct Nerve Injury / Ischemia |
|---|---|---|---|---|
| Onset | Acute (minutes to hours) post-trauma/ischemia-reperfusion | Subacute to delayed (hours to days/weeks) post-trauma/immobility | Subacute to delayed (days) post-injury/wound contamination | Immediate post-trauma |
| Pain Character | Severe, deep, throbbing, constant, unrelenting, out of proportion to injury. Worsened by passive stretch. | Dull ache, tightness, cramping, worse with standing/walking. | Localized, burning, warm, exquisitely tender. | Sharp, burning, shooting, dysesthetic pain along nerve distribution. |
| Swelling | Tense, diffuse swelling in specific compartment(s) ; "wood-hard" feel. | Diffuse, pitting edema, usually entire limb. | Localized erythema, induration, warmth. May have discharge. | Variable, usually less prominent or localized to injury site. |
| Skin Changes | Tense, shiny, pale, cool (late sign). | Erythema (variable), warmth. | Erythema, warmth, tenderness, possibly streaking or bullae. | No primary skin changes unless associated with other injury. |
| Pulses | Often present but may be diminished/absent (late). | Present, usually normal. | Present, usually normal. | Present, usually normal. |
| Capillary Refill | Delayed (>2-3 seconds). | Normal. | Normal. | Normal. |
| Neurological Deficits | Progressive motor weakness & sensory deficits (paresthesia/anesthesia) distal to injury, specific to compromised nerves. | None directly related to nerve compression. | None directly related to nerve compression. | Immediate motor/sensory loss in specific nerve distribution. May be complete. |
| Passive Stretch Pain | Key Sign: Exquisite pain with passive stretch of muscles in affected compartment. | No significant pain with passive stretch of muscles. | Minor discomfort. | No specific pain with passive stretch of muscles unless co-existing injury. |
| Diagnostic Test | Compartment Pressure Measurement (Delta P < 30 mmHg). Clinical diagnosis paramount. | Duplex Ultrasound (venous compression, absence of flow). | Clinical diagnosis, wound culture, elevated inflammatory markers. | Nerve conduction studies/EMG (delayed), clinical exam. |
| Treatment | Emergency Fasciotomy. | Anticoagulation, compression, ambulation. | Antibiotics, wound care, debridement if abscess. | Rest, analgesia, sometimes surgical exploration/repair (e.g., neurorrhaphy). |
Surgical Decision Making & Classification
The decision for operative intervention in this patient was immediate and unequivocal, driven by the compelling clinical findings and objective compartment pressure measurements consistent with acute compartment syndrome. Acute compartment syndrome is a surgical emergency requiring urgent fasciotomy to prevent irreversible neuromuscular damage and limb loss. The presence of an open tibia fracture further complicated the case but did not defer the primary urgency of fasciotomy.
Why Operative vs. Non-operative?
- Acute Compartment Syndrome: The "6 Ps" – Pain out of proportion , Pallor , Paresthesia , Paralysis , Pulselessness , and Poikilothermia – even if not all present, form the clinical foundation. In this case, pain out of proportion , rapidly progressing paresthesia and paralysis (weakness), and compromised pulses/capillary refill strongly indicated ACS.
- Objective Confirmation: Compartment pressure measurements (delta P < 30 mmHg in anterior and lateral compartments) provided objective confirmation, leaving no room for non-operative management. Delay in fasciotomy beyond 6 hours significantly increases the risk of irreversible muscle necrosis, nerve damage, and subsequent functional deficits, contractures, and even amputation.
- Open Fracture: The Gustilo-Anderson Type II open tibia fracture required surgical debridement and stabilization. While addressing the fracture is critical, the compartment syndrome takes precedence for limb salvage.
Classification Systems Relevant to the Case
-
Gustilo-Anderson Classification for Open Fractures:
- Type I: < 1 cm wound, clean, minimal soft tissue damage.
- Type II: 1-10 cm wound, moderate soft tissue damage, moderate comminution.
- Type IIIA: > 10 cm wound, extensive soft tissue damage, high-energy, adequate soft tissue coverage possible.
- Type IIIB: > 10 cm wound, extensive soft tissue damage, periosteal stripping, inadequate soft tissue coverage requiring flap.
- Type IIIC: Arterial injury requiring repair, regardless of soft tissue damage.
- Our patient presented with a 2 cm laceration and moderate soft tissue damage, classifying it as Gustilo-Anderson Type II . This classification guides initial debridement, antibiotic prophylaxis, and subsequent fracture management. The presence of ACS does not alter the Gustilo classification but underscores the severity of soft tissue injury.
-
Tscherne Classification for Closed Fractures (Soft Tissue Injury Grading): While our patient had an open fracture, understanding the Tscherne classification is important for assessing the extent of soft tissue injury in closed fractures which can also lead to compartment syndrome.
- Grade 0: No or minimal soft tissue injury.
- Grade 1: Superficial abrasion, contusion, mild fracture configuration.
- Grade 2: Deep abrasion, muscle contusion, severe fracture configuration.
- Grade 3: Extensive skin contusion/crush, muscle destruction, compartment syndrome, impending vascular injury.
- Though not directly applicable to an open fracture, the severe soft tissue damage and the development of compartment syndrome would place this trauma equivalent to a Tscherne Grade 3 injury in terms of soft tissue insult.
Surgical Technique / Intervention
The patient was immediately transferred to the operating theatre for emergent four-compartment fasciotomy of the right lower leg and debridement of the open tibia fracture.
Patient Positioning and Preparation
- Positioning: Supine on a radiolucent operating table. A bump was placed under the ipsilateral hip to internally rotate the leg slightly for easier access to the lateral aspect. The leg was prepped and draped from the mid-thigh to the toes in a sterile fashion. A tourniquet was placed but not inflated initially, as circulation was compromised.
- Anesthesia: General endotracheal anesthesia.
- Antibiotics: Broad-spectrum IV antibiotics (e.g., Cefazolin and Gentamicin) were administered prior to incision, as per Gustilo-Anderson Type II open fracture protocol. Tetanus prophylaxis was also administered.
Two-Incision Four-Compartment Fasciotomy
The standard two-incision technique was employed to decompress all four fascial compartments of the lower leg.
-
Anterolateral Incision:
- A longitudinal incision was made, approximately 15-20 cm in length, midway between the fibular head and the lateral malleolus, avoiding the superficial peroneal nerve. The incision was made slightly curved towards the anterior border of the fibula proximally and towards the anterior border of the tibia distally, to optimize skin coverage at closure.
- The skin and subcutaneous tissue were incised.
- The fascia overlying the anterior compartment was identified and incised longitudinally along its entire length, releasing the tibialis anterior, extensor digitorum longus, extensor hallucis longus, and peroneus tertius muscles. The deep peroneal nerve and anterior tibial artery were carefully protected.
- Subfascial dissection was performed anterior to the fibula to identify the intermuscular septum separating the anterior and lateral compartments. The fascia overlying the lateral compartment (containing peroneus longus and brevis) was then incised longitudinally, parallel and posterior to the fibula, releasing these muscles. Care was taken to identify and protect the superficial peroneal nerve, which typically exits the lateral compartment distally.
- The muscles within both compartments bulged immediately upon release, confirming the diagnosis of compartment syndrome. The muscle appeared pale and somewhat edematous, but no frank necrosis was visible initially.
-
Medial Incision:
- A second longitudinal incision was made on the medial aspect of the lower leg, approximately 2 cm posterior to the palpable subcutaneous border of the tibia, extending from just distal to the tibial tuberosity to approximately 2 cm proximal to the medial malleolus.
- The skin and subcutaneous tissue were incised.
- The fascia overlying the superficial posterior compartment (gastrocnemius and soleus) was incised longitudinally along its entire length.
- The incision was then deepened through the soleus muscle, or posterior to it, to expose the deep transverse fascia. This fascia was carefully incised longitudinally, releasing the deep posterior compartment (tibialis posterior, flexor digitorum longus, flexor hallucis longus). Neurovascular structures (tibial nerve, posterior tibial artery and veins) within the deep posterior compartment were identified and carefully protected.
- Again, muscle bulging was evident, though less pronounced than in the anterior and lateral compartments.

Figure 2: Illustrative diagram depicting the two-incision four-compartment fasciotomy technique of the lower leg.
Fracture Debridement and Stabilization
- After fasciotomy, attention was turned to the Gustilo-Anderson Type II open tibial fracture. The open wound was thoroughly debrided, removing all devitalized tissue, foreign material, and contaminated bone fragments. Copious irrigation with 9 liters of normal saline was performed.
-
Stabilization:
Given the comminuted nature of the diaphyseal fracture and the significant soft tissue injury requiring open wounds from fasciotomy, definitive internal fixation with an intramedullary nail was chosen as the most appropriate method for stabilization.
- The fracture was provisionally reduced using indirect techniques and a fracture table.
- A standard patellar-splitting approach was utilized to gain access to the proximal tibia.
- The medullary canal was reamed to prepare for nail insertion.
- A 10 mm x 360 mm reamed intramedullary nail was inserted antegrade, and distal and proximal locking screws were placed under fluoroscopic guidance, achieving stable fixation of the tibia fracture.
- Wound Management: The fasciotomy incisions were left open. The fracture wound was partially closed only if feasible, otherwise left open for delayed primary closure or skin grafting. Steri-strips or elastic mesh dressings were applied to gently approximate the skin edges of the fasciotomy wounds without tension, allowing for continuous drainage and muscle expansion. A bulky, sterile dressing was applied, and the limb was splinted in a functional position.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Day 0-7)
- Wound Care: The fasciotomy wounds were inspected daily for signs of infection and to assess muscle viability. Dressings were changed daily, typically with sterile saline-soaked gauze to keep the wounds moist and prevent desiccation.
- Circulation Checks: Frequent neurovascular checks (every 2-4 hours) were maintained to ensure adequate perfusion and monitor for any recurrence of compartment syndrome (though rare post-fasciotomy).
- Pain Management: Aggressive multi-modal analgesia, including opioid and non-opioid medications, was crucial.
- Antibiotics: IV antibiotics were continued for 72 hours post-surgery for the open fracture, then transitioned to oral antibiotics as guided by cultures (if taken during debridement) and clinical response.
- Elevation: The extremity was kept elevated on pillows to reduce swelling.
- Early Mobilization: Gentle, active ankle and toe range of motion exercises were initiated as tolerated to prevent stiffness and promote venous return.
-
Delayed Primary Closure / Skin Grafting:
- Typically, the fasciotomy wounds are re-evaluated at 48-72 hours. If swelling has subsided and muscle tissue is viable, a staged closure is performed.
- Delayed Primary Closure: If skin edges can be approximated without tension (e.g., using vessel loops, shoelace technique, or staged approximation), this is preferred.
- Split-Thickness Skin Grafting (STSG): If the defect is too large for primary closure, split-thickness skin grafts are harvested (commonly from the ipsilateral thigh) and applied to cover the defects. The patient in this case required STSG for the anterior and lateral fasciotomy wounds due to significant skin retraction.
Early Rehabilitation (Week 1-6)
- Weight Bearing: Non-weight bearing (NWB) on the right lower extremity was maintained for the first 4-6 weeks to allow for initial fracture healing and soft tissue recovery. Crutches or a walker were used.
- Range of Motion: Aggressive active and passive ankle and toe range of motion exercises were continued to prevent contractures, particularly ankle equinus and toe flexion contractures, which are common sequelae of compartment syndrome.
- Muscle Strengthening: Isometric exercises for thigh and hip muscles were initiated. Gentle, active-assisted exercises for the ankle and foot were begun as pain allowed, focusing on improving dorsiflexion and eversion.
- Swelling Management: Compression stockings and continued elevation when at rest were utilized to manage persistent edema.
Progressive Rehabilitation (Week 6-12+)
- Weight Bearing Progression: Gradual progression to partial weight-bearing (PWB) as radiographic signs of healing progressed (typically around 6-8 weeks for a tibia fracture) and soft tissue wounds were stable. This progressed to full weight-bearing (FWB) over several weeks, guided by clinical and radiographic assessment.
- Strengthening: Progressive resistive exercises for all lower extremity muscle groups, especially focusing on strengthening muscles in the previously affected compartments to restore motor function.
- Balance & Proprioception: Balance training, proprioceptive exercises, and gait training were introduced to restore functional mobility.
- Scar Management: Silicone sheeting and massage were initiated for fasciotomy scars to minimize hypertrophy and improve pliability.
Long-Term Outcomes
- Patients require long-term follow-up to monitor for potential complications such as chronic pain, residual sensory deficits (e.g., foot drop), muscle weakness, contractures (most commonly ankle equinus, toe clawing), and chronic exertional compartment syndrome. Physiotherapy typically continues for several months.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Clinical Diagnosis First: Compartment syndrome is primarily a clinical diagnosis . Do not wait for objective pressure measurements if clinical suspicion is high. Time is muscle!
- Pain Out of Proportion: This is the most sensitive and often the earliest sign. Unrelenting pain, disproportionate to the apparent injury, and unresponsive to analgesia, must raise immediate suspicion.
- Pain with Passive Stretch: Highly specific and reliable sign, especially in conscious patients. Test each compartment.
- Neurological Changes are Variable: Paresthesia and motor weakness are late signs. If present, they indicate significant, prolonged ischemia. Pulses are often present until very late. Do not wait for pulselessness or paralysis.
- Absolute vs. Delta Pressures: While absolute pressures > 30 mmHg or >40 mmHg (depending on the source) are concerning, the delta pressure (Diastolic Blood Pressure - Compartment Pressure) is often a more reliable indicator, especially in hypotensive patients. A delta pressure < 30 mmHg is the accepted threshold.
- Pressure Monitoring Indications: Useful in unconscious/unreliable patients (e.g., head injury, intoxicated), or for equivocal clinical findings. Serial measurements are often more informative than a single reading.
- Incomplete Fasciotomy is Inadequate: Ensure all four compartments of the lower leg are released (anterior, lateral, superficial posterior, deep posterior).
- High-Risk Injuries: Tibia fractures (especially high-energy and open), revascularization of ischemic limbs, severe crush injuries, burns, and post-operative bleeding are high-risk scenarios. Maintain a high index of suspicion.
- Prophylactic Fasciotomy: Consider in high-risk scenarios where monitoring is impossible or unreliable (e.g., prolonged extrication, delayed presentation of severe crush injury).
Pitfalls
- Delay in Diagnosis: The most common pitfall. Misinterpreting pain as normal post-injury, failing to recognize "pain out of proportion," or relying solely on normal pulses/sensation.
- Over-reliance on Pressure Monitoring: While helpful, pressure measurements should supplement , not replace, clinical judgment. A normal pressure reading in a clinically suspicious patient should prompt repeat evaluation. Conversely, a high pressure in an asymptomatic patient may be monitored, but vigilance is key.
- Inadequate Fasciotomy: Missing a compartment, or making incisions too short, can lead to persistent compartment syndrome and poor outcomes.
- Sedation / Altered Mental Status: Patients with head injuries, poly-trauma, or under heavy sedation are at high risk for missed diagnosis as they cannot report pain reliably. Pressure monitoring becomes crucial here.
- Hypotension: A hypotensive patient can develop compartment syndrome at lower absolute compartment pressures due to a reduced perfusion gradient. Always consider the delta pressure.
- Failure to Address Underlying Cause: While fasciotomy is limb-saving, definitive fracture stabilization (if present) is also critical for long-term function. The sequence of intervention should prioritize life and limb, then function.
- Late Presentation: Patients presenting days after injury with signs of nerve palsy and muscle contracture may have irreversible damage. Fasciotomy is generally not beneficial in these late stages and can increase infection risk. Focus shifts to reconstructive options.
- Not Considering Bilateral Fasciotomy: Although rarer, bilateral compartment syndrome can occur in severe crush or systemic injuries. Always examine both limbs.
