High-Energy Diaphyseal Tibia Fractures: Epidemiology, Anatomy & Biomechanics Guide

Key Takeaway
High-energy diaphyseal tibia fractures result from severe trauma, often presenting with comminution, soft tissue damage, and high complication risks like compartment syndrome and non-union. Their complexity stems from the tibia's precarious subcutaneous location, vital neurovascular structures, and the need for meticulous management integrating anatomy, biomechanics, and soft tissue considerations to optimize outcomes.
Introduction & Epidemiology
High-energy midshaft diaphyseal tibia fractures represent a significant and complex challenge in orthopedic trauma surgery. The tibia, being the most commonly fractured long bone, especially in its diaphyseal segment, is particularly vulnerable to high-energy mechanisms due to its subcutaneous location and relatively sparse soft tissue envelope. These injuries often result from direct trauma, such as motor vehicle collisions (MVCs), pedestrian versus vehicle incidents, falls from significant heights, or ballistic injuries.
Epidemiologically, diaphyseal tibia fractures have an incidence of approximately 16.9 per 100,000 person-years, with a bimodal distribution, affecting young, active males involved in high-energy trauma and elderly individuals with lower-energy falls. High-energy mechanisms are frequently associated with comminution, segmental defects, significant soft tissue compromise, and a higher propensity for open fractures (up to 30-40% in some series). The severe nature of the initial insult significantly increases the risk of complications, including compartment syndrome, infection, non-union, malunion, and persistent functional deficits. A systematic and comprehensive trauma approach, integrating timely assessment, appropriate imaging, meticulous surgical planning, and a nuanced understanding of soft tissue management, is paramount to optimize patient outcomes and minimize morbidity. The presence of significant soft tissue injury often dictates the surgical strategy and timeline, moving beyond merely addressing the bone injury to a holistic approach encompassing vascular, neurologic, and dermatological considerations.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy and biomechanics of the tibia and fibula is fundamental to effective management of diaphyseal tibia fractures.
Tibia Anatomy
The tibia is the primary weight-bearing bone of the lower leg. Its diaphysis is triangular in cross-section proximally, becoming more rounded distally, and tapers towards its midshaft.
*
Bone Structure:
The anterior cortex is thick and dense, while the posteromedial and posterolateral cortices are thinner. The medullary canal is relatively wide, particularly at the isthmus, making it amenable to intramedullary nailing.
*
Blood Supply:
The main blood supply to the tibial diaphysis is primarily from the nutrient artery (a branch of the posterior tibial artery), which enters the posterior cortex just below the soleal line. Periosteal vessels contribute significantly, especially after trauma or reaming. Damage to this supply, particularly in high-energy injuries, can impair healing.
*
Muscle Attachments:
The extensive muscle attachments, particularly the soleus, tibialis posterior, flexor digitorum longus, and flexor hallucis longus posteriorly, and tibialis anterior, extensor digitorum longus, and extensor hallucis longus anteriorly, contribute to deforming forces on fracture fragments.
Fibula Anatomy
The fibula runs parallel to the tibia and serves as an important site for muscle attachments and provides stability to the ankle joint. While not directly weight-bearing in the same capacity as the tibia, an intact fibula can sometimes act as a "splint" to minimally displaced tibia fractures, or, conversely, a fractured fibula can destabilize a tibia fracture construct. In midshaft tibia fractures, the integrity of the fibula affects load sharing and rotational stability, though its primary biomechanical importance is at the ankle and knee.
Soft Tissue Envelope
The tibia has a precarious soft tissue envelope, particularly on its anteromedial surface, where it is largely subcutaneous.
*
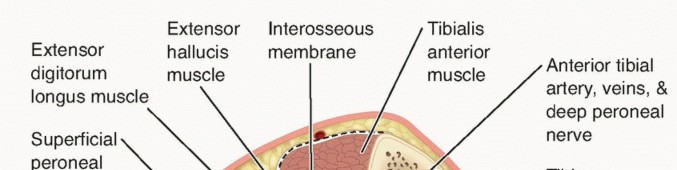
Compartments:
The lower leg is divided into four fascial compartments:
*
Anterior:
Tibialis anterior, extensor hallucis longus, extensor digitorum longus, fibularis tertius. Contains the deep peroneal nerve and anterior tibial artery.
*
Lateral:
Fibularis longus, fibularis brevis. Contains the superficial peroneal nerve.
*
Superficial Posterior:
Gastrocnemius, soleus, plantaris. Contains the sural nerve (variable).
*
Deep Posterior:
Tibialis posterior, flexor digitorum longus, flexor hallucis longus. Contains the tibial nerve and posterior tibial artery.
*
Clinical Significance:
High-energy injuries often cause extensive muscle necrosis and edema, placing the leg at high risk for
compartment syndrome
, a surgical emergency. The limited soft tissue coverage also predisposes to open fractures, wound healing complications, and infection, particularly on the anteromedial aspect.
Neurovascular Structures
Critical neurovascular structures are in close proximity to the tibial diaphysis:
*
Anterior Tibial Artery/Deep Peroneal Nerve:
Run in the anterior compartment, anterior to the interosseous membrane.
*
Peroneal Artery/Tibial Nerve/Posterior Tibial Artery:
Run in the deep posterior compartment.
*
Superficial Peroneal Nerve:
Runs in the lateral compartment, superficially, and is vulnerable to injury or entrapment, especially with lateral approaches or external fixation pin placement.
*
Clinical Significance:
These structures are at risk during initial trauma, fracture manipulation, and surgical approaches. Thorough neurovascular assessment pre- and post-operatively is essential.
Biomechanics of Fracture
High-energy midshaft tibia fractures frequently exhibit comminution, segmental bone loss, and extensive soft tissue stripping. This compromises the inherent stability of the fracture and its biological healing potential. Torsional forces often contribute to spiral or oblique fracture patterns, while direct impact can cause transverse or comminuted fractures. The goal of fixation is to restore length, alignment, and rotation, and to provide sufficient stability to allow for callus formation and union, balancing mechanical rigidity with biological preservation.
Indications & Contraindications
The decision-making process for the management of high-energy midshaft diaphyseal tibia fractures is complex, weighing fracture characteristics, soft tissue status, patient comorbidities, and surgeon experience.
Indications
Most displaced diaphyseal tibia fractures in healthy, active individuals are best treated operatively due to the high risk of malunion, non-union, and unacceptable functional outcomes with non-operative management.
Absolute Operative Indications:
*
Open fractures:
Regardless of displacement, emergent surgical debridement and stabilization are required.
*
Acute compartment syndrome:
Requires emergent fasciotomy, often followed by staged definitive fixation.
*
Vascular injury requiring repair:
Urgent vascular surgery consultation and repair, often with concomitant skeletal stabilization (usually external fixation initially).
*
Polytrauma patients:
Early stabilization of long bone fractures (damage control orthopedics) improves overall outcomes.
*
Pathologic fractures.
Relative Operative Indications:
*
Displaced closed fractures:
Displacement >50% of shaft diameter, angulation >5-10 degrees in any plane (valgus/varus, recurvatum/procurvatum), or shortening >1 cm.
*
Rotational instability:
Significantly displaced spiral or oblique fractures that are difficult to control non-operatively.
*
Irreducible fractures:
Due to soft tissue interposition or severe comminution.
*
Segmental fractures.
*
Associated neurovascular injury (without transection):
To protect compromised structures during healing.
*
Floating knee injury:
Concomitant ipsilateral femur fracture, demanding stable fixation of both bones.
*
Failure of non-operative treatment:
Progressive displacement, intractable pain, or impending skin compromise.
Contraindications
Contraindications are generally relative and must be weighed against the risks of non-operative treatment.
Absolute Contraindications:
*
Medical instability:
Patients unable to tolerate anesthesia or surgery. In these cases, temporary external fixation may be considered for comfort and stability.
Relative Contraindications:
*
Severe local contamination/poor soft tissue quality:
May necessitate staged procedures (external fixation followed by definitive internal fixation once soft tissue improves), or primary soft tissue coverage procedures.
*
Active local infection (non-fracture related):
Requires treatment prior to elective internal fixation.
*
Non-displaced or minimally displaced stable fractures (rare in high-energy context):
Can be managed non-operatively, though surveillance is critical.
Operative vs. Non-Operative Indications: A Summary
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Fracture Type | Displaced, comminuted, segmental, spiral, oblique, open fractures (Gustilo I-III) | Non-displaced or minimally displaced (<50% cortical apposition, <5-10° angulation, <1cm shortening) closed fractures (rare in high-energy) |
| Soft Tissue Status | Open fractures, impending compartment syndrome, significant soft tissue stripping | Closed fractures with minimal soft tissue swelling/ecchymosis |
| Vascular/Nerve | Vascular injury requiring repair, nerve impingement (rarely direct indication) | Intact neurovascular status |
| Patient Status | Medically stable for surgery, polytrauma requiring early stabilization | Medically unstable (absolute contraindication to surgery), uncooperative patient (relative) |
| Associated Injuries | Floating knee, severe foot/ankle trauma, irreducible due to soft tissue interposition | Isolated injury without significant associated soft tissue or bone trauma |
| Previous Treatment | Failure of non-operative treatment (progressive displacement, pain) | Early presentation of stable, minimally displaced injury for trial of casting (with close monitoring) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful management for high-energy midshaft diaphyseal tibia fractures, minimizing intraoperative complications and optimizing outcomes.
Pre-Operative Assessment
- ATLS Protocol: Adherence to Advanced Trauma Life Support (ATLS) principles is paramount for initial patient stabilization, especially in polytrauma patients. Address life-threatening injuries first.
- Primary and Secondary Surveys: A thorough head-to-toe examination is crucial to identify all injuries.
- Neurovascular Status: Document baseline sensory, motor, and vascular status (pulses, capillary refill, ankle-brachial index [ABI]). Repeat assessments frequently.
- Soft Tissue Assessment: Classify open fractures using Gustilo-Anderson (I, II, IIIA, IIIB, IIIC) and closed fractures using Tscherne classification (C0-C3). Note areas of degloving, skin contusion, blisters, and potential for compartment syndrome. Early plastic surgery consultation for complex soft tissue injuries is often beneficial.
- Comorbidities: Assess patient's medical history, including diabetes, peripheral vascular disease, smoking status, and nutritional status, all of which impact healing.
Imaging
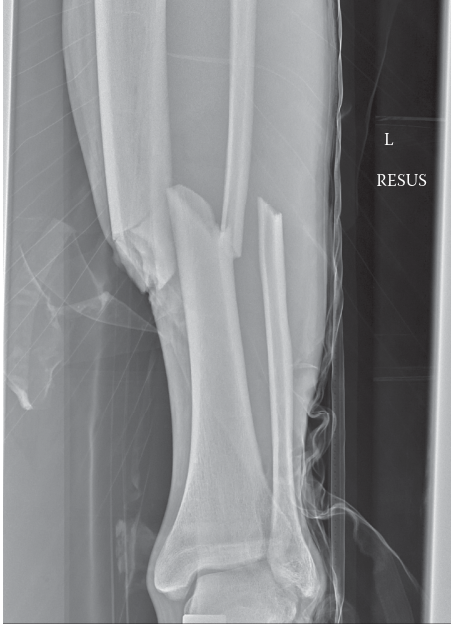
- Plain Radiographs: Anteroposterior (AP) and lateral views of the entire tibia, including the knee and ankle joints, are essential. Oblique views can further characterize fracture morphology.
-
Computed Tomography (CT) Scan:
- Useful for identifying subtle intra-articular extension at the knee or ankle, which can influence fixation strategy.
- Detailed assessment of comminution, bone loss, and fracture geometry.
- Can aid in pre-contoured implant selection.
- Angiography (CT Angiogram or Conventional): Indicated if there is suspicion of vascular injury (diminished/absent pulses, expanding hematoma, thrill/bruit, high-energy injury near known vascular structures).
- MRI: Rarely indicated acutely but may be useful for ligamentous injury assessment at knee/ankle if suspected post-reduction.
Timing of Surgery
- Open Fractures/Compartment Syndrome/Vascular Injury: Emergent surgery (within 6 hours for open fractures, immediately for compartment syndrome/vascular injury).
-
Closed Fractures:
The optimal timing for definitive fixation of closed high-energy tibia fractures depends on the soft tissue condition.
- Damage Control Orthopedics (DCO): For unstable polytrauma patients or those with severe soft tissue swelling/compromise, provisional external fixation is performed first. Definitive fixation (usually IM nailing) is delayed until the patient is physiologically stable and soft tissue swelling has subsided (typically 5-10 days, but can be longer). This reduces the "second hit" phenomenon.
- Early Total Care (ETC): For isolated fractures or stable polytrauma patients with good soft tissue, definitive fixation can proceed within 24-48 hours.
Implants & Equipment
-
Intramedullary (IM) Nailing:
The gold standard for midshaft diaphyseal tibia fractures.
- Nail Selection: Reamed vs. unreamed nails, diameter, length.
- Locking Options: Static (proximal and distal) for unstable/comminuted fractures; dynamic (allowing controlled axial micromotion) for stable fractures.
- Adjuncts: Blocking screws, cerclage wires (sparingly, for highly comminuted segments), reduction clamps.
-
Plates:
Useful for certain fracture patterns (e.g., extremely proximal/distal extension, segmental fractures with significant comminution, failed IM nailing, specific open fracture patterns).
- Types: Locking compression plates (LCP), non-locking plates.
- External Fixation: Primarily for provisional stabilization, damage control, or definitive fixation in severely contaminated open fractures or when internal fixation is contraindicated.
Patient Positioning
- Supine on Radiolucent Table: The standard position.
- Traction Table: Often preferred for facilitating reduction, controlling length and rotation. The injured leg is placed in a traction boot, and the contralateral leg is abducted. Ensure perineal post padding.
- Alternative: Supine with the knee flexed over a bolster/Bohlman table, allowing gravity-assisted reduction and easier access to the proximal tibia.
- Image Intensifier (C-arm): Must have unrestricted access for AP and lateral views of the entire tibia, knee, and ankle. Pre-draping of the C-arm may be considered.
- Tourniquet: Placed high on the thigh. Inflation is at surgeon's discretion, typically used for open fractures or extensive soft tissue work.
Detailed Surgical Approach / Technique
Intramedullary (IM) nailing is the preferred method for definitive fixation of most high-energy midshaft diaphyseal tibia fractures due to its load-sharing characteristics, biological preservation (when performed correctly), and high union rates.
General Principles
- Debridement (Open Fractures): For Gustilo I, II, IIIA fractures, thorough surgical debridement of all contaminated and devitalized tissue is paramount. Pulsatile lavage. Repeat debridement ("second look") after 24-48 hours may be necessary. For Gustilo IIIB/IIIC, plastic surgery collaboration for soft tissue coverage is critical.
- Provisional Stabilization: Often achieved with external fixation in the initial stages for damage control or severe open fractures.
- Definitive Fixation: Aims to restore length, alignment, and rotation, and provide sufficient stability for fracture healing while preserving soft tissue and bone biology.
Intramedullary Nailing Technique
1. Incision and Entry Point
The choice of entry point is critical to avoid malalignment (especially apex anterior/posterior deformity or valgus/varus) and iatrogenic injury.
*
Patellar Ligament Splitting:
A vertical incision just distal to the patella, splitting the patellar tendon centrally or paratendinously (medial or lateral to the tendon). This allows direct access to the tibial tubercle.
*
Suprapatellar (Transpatellar) Entry:
A more recent technique involving a small incision above the patella, passing a specialized cannula
through
the quadriceps tendon and patellofemoral joint into the tibia. This offers advantages in proximal fragment control and alignment, especially in obese patients or those with a high-riding patella. Requires careful attention to cartilage protection.
*
Entry Point Preparation:
Once the entry point is identified on the proximal tibia (usually medial to the lateral tibial spine and lateral to the medial tibial spine, aligning with the intercondylar notch), an awl or drill is used to open the cortex. The goal is to align with the central axis of the medullary canal in both AP and lateral planes.
2. Reaming vs. Unreamed Nailing
-
Reamed Nailing:
Involves sequentially enlarging the medullary canal with flexible reamers.
- Advantages: Maximizes nail-to-bone contact, allowing for a larger diameter and stiffer nail, which provides greater rotational and bending stability. Enhances primary callus formation. Creates a "bone paste" which may have osteoinductive properties.
- Disadvantages: Can damage endosteal blood supply, increase intramedullary pressure, potentially exacerbating fat embolism risk or compartment syndrome. Not ideal in contaminated open fractures due to potential spread of infection.
-
Unreamed Nailing:
Uses a smaller diameter nail without reaming.
- Advantages: Preserves endosteal blood supply, lower risk of fat embolism, generally preferred for Gustilo II and IIIA open fractures to avoid spreading contamination.
- Disadvantages: Smaller nail provides less mechanical stability, potentially higher rates of non-union or hardware failure in comminuted fractures.
3. Fracture Reduction
Achieving and maintaining anatomical or near-anatomical reduction is paramount. This can be challenging in high-energy, comminuted fractures.
*
Manual Traction:
Often used on a fracture table or with an assistant pulling longitudinal traction.
*
External Fixator Assist:
A temporary external fixator across the fracture site can provide excellent control over length, alignment, and rotation.
*
Blocking Screws (Poller Screws):
Small cortical screws placed adjacent to the IM nail track to guide the nail into the correct position, preventing malalignment in specific planes (e.g., apex anterior/posterior, valgus/varus). Especially useful for metadiaphyseal fractures or wide medullary canals.
*
Cerclage Wires:
Rarely used for midshaft diaphyseal fractures due to disruption of periosteal blood supply, but may be considered for large butterfly fragments that are difficult to reduce or stabilize. Use sparingly and with caution.
*
Percutaneous Clamps:
Pointed reduction clamps can be used percutaneously to reduce fragments under fluoroscopic guidance.
-
Image demonstrating fracture reduction or entry point planning:

4. Nail Insertion
Once reduction is achieved and confirmed with fluoroscopy, the appropriately sized IM nail is inserted.
*
Selection:
The nail should be of sufficient length to achieve fixation in both the proximal and distal fragments, typically extending to the subchondral bone of the knee and ankle. The diameter is chosen based on reaming size or canal width.
*
Insertion:
The nail is carefully advanced across the fracture site. Fluoroscopy is continuously used to monitor progress, ensure reduction is maintained, and prevent iatrogenic comminution.
*
Interlocking:
*
Proximal Interlocking:
Achieved first, typically with two screws in static mode to prevent shortening and rotation. Use a targeting device.
*
Distal Interlocking:
More challenging due to convergence of the canal and potential for neurovascular injury. Freehand technique often required. Aim for two screws, again for static stability. Fluoroscopy in two planes (AP and lateral) is critical. Some nails offer multi-planar distal locking options.
-
Image demonstrating final IM nail construct:
5. Verification
After nail insertion and locking, perform a final fluoroscopic check to confirm:
* Adequate length of the tibia.
* Appropriate axial and rotational alignment.
* Secure placement of all locking screws.
* No iatrogenic fracture or soft tissue impingement.
Plate Fixation (Alternative/Adjunct)
Plate fixation is generally a secondary option for midshaft diaphyseal tibia fractures but has specific indications.
*
Indications:
* Fractures with significant metaphyseal extension (proximal or distal) where IM nailing cannot achieve adequate purchase.
* Extremely wide medullary canals precluding stable IM nailing.
* Segmental fractures with large, reconstructible fragments.
* Open fractures with extensive bone loss or comminution requiring primary reconstruction, especially when IM nailing is contraindicated due to severe contamination.
* Failed IM nailing.
* Certain non-unions.
*
Approach:
Anteromedial approach to the tibia is most common, being aware of the superficial neurovascular structures and the limited soft tissue.
*
Technique:
*
Bridge Plating:
For comminuted fractures, a long locking compression plate (LCP) is used as a bridge, spanning the comminution without direct screw purchase into the comminuted zone. This provides relative stability, promoting callus formation. Restore length and alignment indirectly.
*
Compression Plating:
For simple transverse or short oblique fractures, interfragmentary compression with lag screws (if fracture geometry allows) combined with a neutralization plate for absolute stability. Less common in high-energy comminuted fractures.
-
Image demonstrating a specific reduction technique or complex fixation (e.g., blocking screws, temporary plate for reduction, or external fixator assisting IM nail):
External Fixation
Primarily used for damage control, especially in polytrauma patients, or as definitive fixation for highly contaminated Gustilo IIIB/IIIC open fractures, severe crush injuries, or infected non-unions.
*
Technique:
Placement of pins into the tibia and sometimes fibula, connecting them with external rods to create a rigid frame.
* Careful pin placement to avoid neurovascular structures and zones of future definitive fixation.
* Pins typically placed anteromedially or medially.
* Allows for wound care and soft tissue management without disturbing the fracture.
* Can be monoplanar or multiplanar.
Adjuvant Techniques
- Bone Grafting: For fractures with significant bone loss or at high risk for non-union, autogenous bone graft (iliac crest, fibula) or allograft can be used, often delayed until soft tissue healing is complete.
- Soft Tissue Coverage: For large soft tissue defects, plastic surgery consultation for local or free flap coverage is essential.
Complications & Management
High-energy midshaft diaphyseal tibia fractures carry a substantial risk of complications, necessitating vigilant monitoring and proactive management strategies.
Early Complications
-
Compartment Syndrome:
- Incidence: 5-10% in closed tibia fractures, higher in high-energy mechanisms.
- Description: Increased pressure within a closed fascial compartment leading to muscle and nerve ischemia. Classic signs: disproportionate pain with passive stretch, paresthesia, pallor, pulselessness (late sign), paralysis (late sign).
- Management: Emergent four-compartment fasciotomy. Delayed wound closure. Prognosis depends on timely diagnosis and intervention.
-
Infection (especially open fractures):
- Incidence: Up to 50% in Gustilo IIIB/IIIC open fractures, 1-5% in closed fractures treated with IM nailing.
- Description: Bacterial contamination leading to osteomyelitis and delayed healing.
- Management: Aggressive serial debridement, appropriate intravenous antibiotics, negative pressure wound therapy (NPWT), and often soft tissue coverage (flaps). May require hardware removal and external fixation or staged reconstruction.
-
Vascular Injury:
- Incidence: 5-10%, higher in Gustilo IIIC open fractures (by definition).
- Description: Laceration, transection, or thrombosis of major arteries (anterior/posterior tibial, peroneal). Presents as pulselessness, pallor, cold extremity.
- Management: Emergent vascular surgery consultation and repair (bypass or primary repair). Often requires temporary external fixation of the bone to provide stability for vascular repair.
-
Nerve Injury:
- Incidence: Varies, can affect peroneal nerve (foot drop) or tibial nerve.
- Description: Direct trauma, traction, or compression.
- Management: Observe for neuropraxia. Surgical exploration for complete deficits or open injuries.
-
Fat Embolism Syndrome (FES):
- Incidence: Rare but potentially life-threatening. Higher risk in poly-trauma, reamed IM nailing.
- Description: Triad of respiratory insufficiency, neurological dysfunction, and petechial rash.
- Management: Supportive care (ventilatory support), prevention (early stabilization of fractures, careful reaming).
Late Complications
-
Non-union:
- Incidence: 5-15% for IM nailing, higher in open fractures, comminuted fractures, and smokers.
- Description: Failure of fracture healing after 6-9 months, or no progression of healing for 3 consecutive months. Avascular vs. hypertrophic.
- Management: Revision surgery (exchange nailing, plate osteosynthesis with bone grafting, external fixation, biological stimulation like pulsed electromagnetic fields).
-
Malunion:
- Incidence: 10-20%, commonly rotational or angular.
- Description: Fracture healed in an unacceptable position (e.g., >10-15 degrees angulation, >10-15 degrees rotation, >1.5-2 cm shortening). Can lead to altered gait, pain, and future arthritis.
- Management: Corrective osteotomy and internal fixation, often with IM nail or plate.
-
Hardware Failure:
- Incidence: Varies, often associated with non-union or high-stress environments.
- Description: Breakage of the nail or plate, screw loosening/breakage.
- Management: Revision surgery, addressing the underlying reason for failure (e.g., non-union).
-
Chronic Pain/Stiffness:
- Incidence: Common, especially around the knee (anterior knee pain post-IM nailing) and ankle.
- Description: Persistent pain, limited range of motion.
- Management: Physical therapy, pain management, hardware removal (if symptomatic).
-
Refracture:
- Incidence: Rare but possible, often after hardware removal.
- Description: Fracture occurring after initial union and removal of hardware.
- Management: Re-fixation, typically with IM nailing.
Complications and Management Table
| Complication | Incidence (approx.) | Salvage Strategies / Management |
|---|---|---|
| Compartment Syndrome | 5-10% (closed tibia fx) | Emergent four-compartment fasciotomy; delayed wound closure. |
| Infection | 1-5% (closed); 5-50% (open) | Serial debridement, IV antibiotics, NPWT, soft tissue flaps, hardware retention/removal and re-stabilization. |
| Vascular Injury | 5-10% (high-energy) | Emergent vascular repair/bypass; provisional external fixation. |
| Nerve Injury | Variable | Observation (neuropraxia); surgical exploration for complete deficits. |
| Fat Embolism Syndrome | Rare (0.5-2%) | Supportive care (ventilatory support); prevention through early stabilization. |
| Non-union | 5-15% | Exchange nailing, plate osteosynthesis with bone graft, external fixation, biological stimulation. |
| Malunion | 10-20% | Corrective osteotomy, internal fixation (nail/plate). |
| Hardware Failure | Variable | Revision surgery to address underlying cause (e.g., non-union), new implant. |
| Chronic Pain | Common (e.g., anterior knee pain) | Physical therapy, pain management, hardware removal (if symptomatic). |
| Refracture | <5% | Re-fixation with appropriate implant (often IM nail). |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for achieving optimal functional outcomes following high-energy midshaft diaphyseal tibia fractures. Protocols must be tailored to the individual patient, considering fracture stability, fixation method, soft tissue healing, and comorbidities.
Phase 1: Immediate Post-Operative (Weeks 0-6)
- Goals: Control pain and swelling, protect fixation, maintain joint range of motion (ROM) in adjacent joints, prevent muscle atrophy, monitor for complications.
-
Weight Bearing:
- Non-weight bearing (NWB) or Touch-down weight bearing (TDWB): For highly comminuted, unstable fractures, poor bone quality, significant soft tissue injury, or when unreamed nails are used.
- Protected weight bearing (PWB) / Weight bearing as tolerated (WBAT): For stable fractures fixed with reamed IM nails, especially if cortical contact is good.
- Assistive devices (crutches, walker) are used.
-
Range of Motion:
- Ankle: Early active and passive ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion) to prevent stiffness and promote venous return.
- Knee: Early active and passive knee ROM exercises (flexion, extension) within pain limits, particularly for suprapatellar nailing to minimize arthrofibrosis.
-
Muscle Activation:
- Isometric quadriceps and hamstring sets.
- Gluteal sets.
- Calf pumps (non-weight bearing).
- Wound Care: Meticulous pin site care (if external fixation), wound dressing changes, monitoring for signs of infection.
Phase 2: Early Mobilization & Progressive Loading (Weeks 6-12)
- Goals: Increase weight bearing, improve ROM, restore muscle strength, progress functional mobility.
- Weight Bearing: Progress from NWB/TDWB to PWB/WBAT as radiological signs of healing (early callus formation) become evident and pain allows. Regular follow-up radiographs (every 4-6 weeks) guide progression.
- Range of Motion: Continue with full active and passive ROM for knee and ankle.
-
Strengthening:
- Progressive resistive exercises for quadriceps, hamstrings, and calf muscles (e.g., knee extensions/curls, heel raises).
- Core strengthening.
- Gait Training: Focus on normal gait mechanics, weaning off assistive devices as strength and confidence improve.
- Edema Management: Compression stockings, elevation.
Phase 3: Advanced Strengthening & Return to Activity (Weeks 12+)
- Goals: Achieve full functional ROM, strength, endurance, and proprioception; prepare for return to pre-injury activities.
- Weight Bearing: Full weight bearing as tolerated, without assistive devices, once clinical and radiographic union are confirmed.
- Strengthening: Advanced strengthening exercises including eccentric loading, plyometrics (if appropriate), single-leg balance, and functional movements specific to the patient's goals.
- Proprioception/Balance: Wobble board, single-leg stance, dynamic balance exercises.
- Cardiovascular Fitness: Low-impact activities (swimming, cycling) progressing to higher-impact as appropriate.
- Return to Sport/Work: Gradual progression, guided by functional assessments, strength testing, and psychological readiness. Full return to high-impact sports typically takes 9-18 months.
Considerations
- Smoking Cessation: Absolutely critical to promote healing and reduce complication rates.
- Nutrition: Adequate protein and micronutrient intake are vital for bone healing.
- Pain Management: Multimodal approach to manage post-operative pain.
- Hardware Removal: Elective hardware removal (e.g., IM nail for anterior knee pain) may be considered 12-24 months post-union, but only after careful consideration of risks versus benefits, and only if symptoms persist and are directly attributable to the hardware.
Summary of Key Literature / Guidelines
The management of high-energy midshaft diaphyseal tibia fractures has evolved significantly, guided by extensive research and consensus from organizations such as the Orthopaedic Trauma Association (OTA) and AO Foundation. Key principles and controversies persist:
1. Intramedullary Nailing as the Gold Standard
- Evidence: Numerous meta-analyses and randomized controlled trials (RCTs) confirm that reamed intramedullary nailing is the gold standard for diaphyseal tibia fractures due to superior union rates, lower reoperation rates, and faster time to union compared to plating or casting for most patterns.
- Specifics: Reamed nailing generally results in higher union rates and stronger constructs than unreamed nailing, particularly in closed and Gustilo I/II open fractures. Unreamed nailing is often favored for Gustilo IIIA/B open fractures to minimize infection spread and preserve endosteal blood supply, although controversy exists regarding its long-term outcomes versus delayed reamed nailing.
2. Timing of Definitive Fixation
- Damage Control Orthopedics (DCO): For polytrauma patients or those with severe soft tissue swelling, provisional external fixation followed by delayed definitive internal fixation (typically within 5-10 days) is supported by evidence to reduce systemic inflammatory response and improve outcomes ("early appropriate care").
- Early Total Care (ETC): For isolated tibia fractures or physiologically stable patients, definitive fixation within 24-48 hours is generally safe and often preferred. Delayed fixation beyond 2 weeks can increase the risk of malunion and technical difficulty.
3. Soft Tissue Management
- Open Fractures: Early, aggressive, and serial debridement (within 6 hours for Gustilo I/II, potentially longer for III if limb is viable and patient stable) remains the cornerstone of open fracture management. The goal is conversion of a contaminated wound to a clean surgical wound.
- Antibiotics: Broad-spectrum antibiotics (first/second-generation cephalosporin and an aminoglycoside; penicillin for severe contamination) should be administered as early as possible and continued for 24-72 hours post-debridement, depending on Gustilo grade.
- Soft Tissue Coverage: For Gustilo IIIB/IIIC fractures, early definitive soft tissue coverage (within 7 days) by plastic surgery has been shown to reduce infection rates and improve outcomes.
4. Anterior Knee Pain Post-IM Nailing
- Prevalence: Up to 50% of patients experience anterior knee pain after IM nailing of the tibia.
- Etiology: Likely multifactorial, including patellar tendon irritation, hardware prominence, nerve impingement, and quadriceps atrophy.
- Management: While common, hardware removal for symptomatic pain is often effective, but should be delayed until complete union. Suprapatellar nailing techniques may reduce this incidence by avoiding direct patellar tendon disruption, though further long-term studies are needed.
5. Role of Adjuncts
- Blocking Screws: Evidence supports the use of blocking screws (Poller screws) to optimize alignment and prevent malreduction, especially in metadiaphyseal fractures or those with wide canals.
- Bone Grafting: Autogenous bone grafting is generally indicated for fractures with significant bone loss, delayed union, or non-union. Prophylactic grafting for highly comminuted open fractures is controversial but may be considered for large segmental defects.
6. Malunion and Non-union
- Prevention: Meticulous surgical technique, appropriate choice of implant, and rigorous post-operative follow-up are critical.
- Management: Exchange nailing is a highly effective treatment for aseptic hypertrophic non-unions. Other options include plating with bone grafting or external fixation with bone transport. Corrective osteotomies are utilized for symptomatic malunions.
The principles of high-energy midshaft diaphyseal tibia fracture management emphasize prompt trauma assessment, meticulous soft tissue handling, stable internal fixation, and comprehensive rehabilitation, continuously adapting to new evidence and surgical innovations.
You Might Also Like