Radial Head Fractures: Comprehensive Epidemiology, Classification, Anatomy & Biomechanics

Key Takeaway
Radial head fractures are elbow injuries classified by Mason-Hotchkiss (Types I-IV) based on displacement. Associated injuries like MCL/LCL tears are critical. Understanding surgical anatomy, the radial head's role in axial load and forearm rotation, plus overall elbow biomechanics, is paramount for guiding effective treatment and restoring long-term function.
Introduction & Epidemiology
Radial head fractures constitute a significant proportion of all elbow fractures, representing approximately 1.7% of all fractures and 33% of elbow fractures in adults. These injuries are more prevalent in adults aged 30-40 years, with a slight male predominance. The typical mechanism of injury involves a fall onto an outstretched hand (FOOSH) with the elbow in slight flexion and the forearm pronated, often resulting in an axial load combined with a valgus stress across the elbow joint.
While often considered relatively benign, radial head fractures can be associated with severe soft tissue and osseous injuries, leading to significant long-term disability if not appropriately managed. Associated injuries are crucial to identify and include capitellum fractures, coronoid process fractures, medial collateral ligament (MCL) tears, lateral collateral ligament (LCL) complex injuries, and interosseous membrane disruption (Essex-Lopresti injury). The presence of these concomitant injuries significantly impacts treatment algorithms and prognosis.
Classification systems are integral for guiding treatment and predicting outcomes. The most widely adopted system is the
Mason-Hotchkiss classification
:
*
Type I:
Nondisplaced or minimally displaced (<2 mm) crack or marginal impaction, no mechanical block to forearm rotation.
*
Type II:
Displaced (>2 mm) or angulated fracture, involving a portion of the articular surface, often with a mechanical block to forearm rotation.
*
Type III:
Comminuted fracture involving the entire radial head, often with significant displacement, impaction, and mechanical block. These are typically unreconstructible.
*
Type IV (Added by Hotchkiss):
Radial head fracture with associated elbow dislocation.
This classification, combined with an assessment of associated ligamentous and osseous injuries, dictates the decision-making process between non-operative and operative management strategies. The primary goals of treatment are to restore painless elbow motion, stability, and function, particularly forearm rotation, and to minimize the risk of post-traumatic arthritis.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the elbow joint, particularly the proximal radius, is paramount for successful management of radial head fractures.
Radial Head and Proximal Radius
The radial head is a cylindrical structure, articulating proximally with the capitellum of the humerus and medially with the radial notch of the ulna, forming the humeroradial and proximal radioulnar joints, respectively. Its superior surface is concave and cartilage-covered, facilitating articulation with the capitellum. The circumference of the radial head is also covered by articular cartilage, crucial for smooth rotation within the annular ligament and against the radial notch.
Distal to the radial head lies the radial neck, which narrows considerably before flaring out to the radial tuberosity, the insertion site for the biceps brachii tendon. The blood supply to the radial head primarily arises from branches of the radial recurrent artery, forming an extensive arterial ring around the neck.
Ligamentous Structures
The stability of the elbow joint is conferred by its bony architecture and, critically, by its robust ligamentous complexes.
*
Lateral Collateral Ligament (LCL) Complex:
Comprises the radial collateral ligament (RCL), annular ligament, and the lateral ulnar collateral ligament (LUCL). The LUCL is the primary stabilizer against posterolateral rotatory instability, originating from the lateral epicondyle and inserting into the supinator crest of the ulna. The annular ligament encircles the radial head, securing it within the radial notch, while the RCL provides varus stability. Integrity of the LUCL is paramount in radial head fractures, especially when considering excision or arthroplasty, as its compromise can lead to significant instability.
*
Medial Collateral Ligament (MCL) Complex:
Composed of the anterior bundle (primary valgus stabilizer), posterior bundle, and transverse ligament. While less commonly injured with isolated radial head fractures, MCL tears are frequently seen in severe fracture-dislocations (e.g., terrible triad).
Biomechanics of the Radial Head
The radial head plays a crucial role in axial load transmission across the elbow, accounting for approximately 60% of the axial load in elbow extension and increasing to 80% with valgus stress. It also acts as a secondary valgus stabilizer, particularly when the MCL is intact. Its articulation with the capitellum and the ulna allows for forearm rotation (pronation and supination), a function that is often severely compromised by displaced or comminuted radial head fractures. An intact radial head is essential for maintaining the length of the radius relative to the ulna, thus preventing proximal radial migration and subsequent wrist pain (ulnar impaction syndrome) – a known sequela of radial head excision without replacement in certain contexts.
Neurovascular Structures
Understanding the spatial relationship of nerves and vessels is critical during surgical approaches.
*
Posterior Interosseous Nerve (PIN):
A branch of the radial nerve, it passes through the supinator muscle, supplying the extensors of the forearm. Its proximity to the radial head, particularly its course within the supinator, makes it vulnerable during lateral surgical approaches.
*
Radial Nerve:
Lies anterior to the lateral epicondyle, dividing into superficial (sensory) and deep (PIN) branches.
*
Median Nerve:
Located medially, less commonly at risk with standard lateral approaches.
*
Brachial Artery:
Located anteriorly, along with the median nerve, within the cubital fossa.
Knowledge of these anatomical relationships informs the choice of surgical approach, extent of dissection, and precautions required to minimize iatrogenic injury.
Indications & Contraindications
The decision-making process for radial head fractures involves a careful assessment of the fracture pattern, associated injuries, patient factors, and the stability of the elbow joint. The primary goal is to restore a stable, mobile, and pain-free elbow.
Non-Operative Indications
Non-operative management is typically reserved for stable fracture patterns without mechanical blockage or associated instability.
*
Mason Type I fractures:
These are nondisplaced or minimally displaced (<2 mm) and inherently stable.
*
Select Mason Type II fractures:
If displacement is minimal, angulation is minor, and there is no demonstrable mechanical block to forearm rotation (pronation/supination) or elbow flexion/extension, a trial of non-operative management may be considered. These patients require close follow-up to ensure maintenance of reduction and resolution of pain.
Contraindications for Non-Operative Management:
* Gross instability on examination (valgus/varus stress testing).
* Mechanical block to forearm rotation (>30 degrees loss compared to contralateral side).
* Significant displacement (>2 mm), articular step-off (>2 mm), or angular deformity (>30 degrees).
* Associated unstable elbow dislocation, coronoid fracture, or complete LCL disruption.
* Essex-Lopresti lesion (radial head fracture with interosseous membrane disruption and distal radioulnar joint instability).
Operative Indications
Operative intervention is warranted for fractures that are unstable, mechanically symptomatic, or associated with other significant injuries that compromise elbow stability and function.
-
Mason Type II fractures:
- Significant displacement (>2 mm) or angulation.
- Mechanical block to forearm rotation (e.g., inability to achieve full pronation/supination).
- Persistent pain or instability.
- Associated LCL injury or suspected instability.
- Mason Type III fractures: These are inherently unstable and typically unreconstructible. The standard of care often involves radial head arthroplasty, or, less commonly, excision in carefully selected, low-demand patients without associated instability.
- Mason Type IV fractures (fracture-dislocations): Always require operative intervention. The radial head fracture contributes significantly to elbow instability in these complex injuries.
-
Associated Injuries:
- Coronoid fractures: Especially if >50% involvement or associated with elbow instability.
- Complete LCL complex rupture: Particularly in the context of elbow dislocation or posterolateral rotatory instability.
- Essex-Lopresti injury: Requires radial head replacement to restore forearm length and prevent proximal radial migration.
- Open fractures: Require urgent debridement and stabilization.
Absolute Contraindications for Surgery:
* Severe medical comorbidities precluding safe anesthesia and surgery.
* Active infection at the surgical site.
* Non-ambulatory, low-demand patients with minimal symptoms from a stable fracture (relative contraindication).
Summary of Operative vs. Non-Operative Indications
| Indication Category | Non-Operative Treatment | Operative Treatment (ORIF, Excision, or Arthroplasty) |
|---|---|---|
| Mason Classification | Type I (nondisplaced) | Type II (displaced, mechanical block, or associated instability) |
| Select Type II (minimal displacement, no mechanical block) | Type III (comminuted, unreconstructible) | |
| Type IV (fracture with elbow dislocation) | ||
| Displacement/Angulation | <2 mm displacement, <30° angulation | >2 mm displacement, >30° angulation, articular step-off >2 mm |
| Mechanical Block | None | Present (e.g., >30° loss of forearm rotation or significant block to flexion/extension) |
| Associated Ligamentous | None/Mild sprain | LCL rupture (clinically or radiographically unstable) |
| Associated Osseous | None/Stable minor associated fracture | Coronoid fracture (>50% involvement, unstable), Capitellum fracture, Olecranon fracture, Essex-Lopresti lesion |
| Open Fractures | N/A | All open fractures |
| Patient Factors | Elderly, low demand, high surgical risk | Active, high-demand, otherwise healthy, with fracture amenable to reconstruction or replacement for functional return |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for predictable outcomes in radial head fracture surgery.
Imaging
-
Standard Radiographs: AP, lateral, and oblique views (Greenspan/radiocapitellar view, capitellum view) are initial studies. These provide basic information on fracture pattern, displacement, and angulation. Oblique views are particularly useful for visualizing the articular surface of the radial head and assessing comminution.
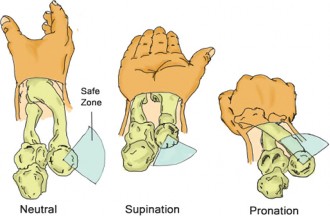
Figure 1: Standard anteroposterior radiograph demonstrating a displaced radial head fracture. Note the comminution and lateral displacement of the radial head fragment. -
Computed Tomography (CT) Scan: Indispensable for complex fractures (Mason Type II, III, IV), especially those with comminution, significant displacement, or associated coronoid fractures. 3D reconstructions are invaluable for understanding the fracture morphology, degree of articular involvement, and planning fixation strategies (e.g., screw trajectory). A CT scan also helps identify subtle capitellar or coronoid involvement often missed on plain radiographs.
-
Magnetic Resonance Imaging (MRI): Generally not routinely indicated unless there is strong suspicion of significant ligamentous injury (MCL, LCL complex), particularly in the absence of dislocation, or persistent pain after initial stabilization. It can be useful in evaluating interosseous membrane disruption in suspected Essex-Lopresti injuries.
Patient Selection and Implant Choice
Patient age, activity level, functional demands, and bone quality significantly influence implant choice. For reconstructible fractures (Mason Type II), small fragment screws (headless compression screws, 2.0 or 2.4 mm cortical screws) or specialized radial head plates are utilized. For unreconstructible fractures (Mason Type III) or those with significant instability (Mason Type IV, Essex-Lopresti), radial head arthroplasty (RHA) with a prosthesis is typically indicated. Prostheses can be monoblock or modular, stemmed or non-stemmed, and made of various materials (cobalt-chrome, titanium, pyrocarbon). Excision is reserved for very selective cases in low-demand patients without associated instability.
Patient Positioning and Setup
The patient is typically positioned
supine
on a standard operating table or a radiolucent table.
*
Arm Board:
The affected arm is placed on a padded arm board, allowing for full range of motion (flexion, extension, pronation, supination) and access for intraoperative fluoroscopy. Some surgeons prefer to flex the elbow to 90 degrees and support it with a sterile bolster, particularly if a posterior approach or significant ligamentous work is anticipated.
*
Tourniquet:
A pneumatic tourniquet is applied to the upper arm for a bloodless field, crucial for visualization of small fragments and delicate neurovascular structures.
*
C-arm Fluoroscopy:
Essential for intraoperative assessment of reduction, implant placement, and confirmation of elbow stability. The C-arm should be draped sterilely and positioned to allow unobstructed AP and lateral views of the elbow.
*
Pneumatic Distraction (Optional):
In complex fracture-dislocations, a mini-external fixator or pneumatic distractor across the elbow can aid in restoring joint alignment and facilitating reduction before definitive fixation.
Preparation involves standard sterile draping, encompassing the entire limb from shoulder to hand to allow full manipulation and visualization of the forearm and wrist.
Detailed Surgical Approach / Technique
The choice of surgical approach depends on the fracture pattern, the need to address associated injuries, and the surgeon's preference. The anterolateral approach (modified Kocher or Kaplan approach) is the most common for radial head fractures.
Anterolateral Approach (Modified Kocher or Kaplan)
-
Incision: A longitudinal incision is made over the lateral aspect of the elbow, typically centered just anterior to the lateral epicondyle, extending proximally 3-5 cm and distally 5-7 cm along the lateral supracondylar ridge and proximal forearm. This allows direct access to the radial head and the lateral collateral ligament complex.
-
Dissection and Internervous Plane:
- The subcutaneous tissue and fascia are incised. Care is taken to identify and protect superficial nerves and veins.
- The deep fascia is opened, exposing the muscle bellies. The internervous plane for this approach is generally considered between the anconeus and extensor carpi ulnaris (ECU) muscles posteriorly, and the extensor carpi radialis brevis (ECRB) and supinator muscles anteriorly.
- Alternatively, a plane between the brachioradialis and extensor carpi radialis longus/brevis can be utilized, providing a more anterior approach.
- The lateral collateral ligament (LCL) complex , specifically the lateral ulnar collateral ligament (LUCL) , is identified. If unstable or avulsed, its repair will be critical. If the joint is stable, a limited longitudinal capsulotomy can be performed. If stability is questionable or the fracture complex, a full Kocher approach may be required, which dissects between the anconeus posteriorly and the extensor carpi ulnaris anteriorly.
- A critical step is the careful subperiosteal elevation of the supinator muscle from the posterior aspect of the proximal radius, commencing distally and moving proximally. This protects the posterior interosseous nerve (PIN) , which enters the supinator muscle approximately 2-4 cm distal to the radial head. The forearm should be kept in full supination during this maneuver to move the PIN anteriorly and away from the surgical field.
-
Capsulotomy and Fracture Exposure: Once the supinator is safely retracted, a longitudinal or L-shaped capsulotomy is performed to expose the radial head fracture. The fracture fragments are identified, and hematoma and any loose osteochondral fragments are debrided from the joint.
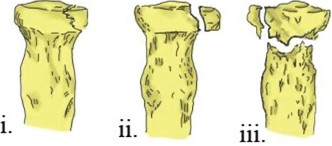
Figure 2: Intraoperative view through a lateral approach, demonstrating the exposed radial head fracture. Note the comminution and displacement of articular fragments.
Reduction and Fixation Techniques
A. Open Reduction Internal Fixation (ORIF) - For Mason Type II Fractures
- Fragment Reduction: The fracture fragments are meticulously reduced using gentle manipulation, small pointed reduction clamps, and temporary K-wires. Articular congruity is prioritized. Fluoroscopy is used to confirm reduction.
-
Fixation with Headless Compression Screws:
This is the preferred method for reconstructible radial head fractures.
- Small diameter (2.0 or 2.4 mm) headless compression screws are inserted.
- Screws should be placed from the non-articulating portion of the radial head (typically anterior or posterior) across the fracture line into the largest fragment.
- Crucially, screws must be placed parallel to the articular surface , ideally 2-3 mm distal to the articular margin, and should not violate the proximal radioulnar joint (PRUJ) or impinge on the capitellum during rotation. This placement avoids prominent hardware in the articular surface.
- Multiple screws may be needed for stable fixation.
-
Fixation with Plates:
Small fragment plates (e.g., 2.0 mm or 2.4 mm locking plates designed for the radial head) are considered for:
- More comminuted Mason Type II fractures where screws alone may not provide sufficient stability.
- Fractures with a large, displaced wedge fragment.
- Radial head plates are contoured to the anatomy and secured with locking or non-locking screws. The plate position should avoid impingement with the ulna or capitellum during forearm rotation and elbow flexion/extension.
B. Radial Head Arthroplasty (RHA) - For Mason Type III and IV Fractures
- Indications: Irreparable comminuted radial head fractures (Mason Type III), radial head fractures with elbow dislocation (Mason Type IV), or Essex-Lopresti injuries, especially in younger, active patients where excision alone would lead to instability or proximal radial migration.
- Resection of Radial Head: The comminuted radial head fragments are carefully removed. The radial neck is then prepared by reaming or burring to create a smooth, cylindrical surface for the prosthesis.
-
Trial Sizing:
Trial implants are used to determine the appropriate head diameter and stem length. The goal is to restore radial length and provide appropriate tension to the lateral ligamentous structures, while avoiding overstuffing the radiocapitellar joint.
Figure 3: Illustration depicting a modular radial head prosthesis designed for arthroplasty. Such prostheses aim to restore articular congruity and maintain radial length. - Implant Insertion: The definitive prosthesis (monoblock or modular) is inserted, usually press-fit or cemented depending on the design. Modular designs allow independent sizing of head and stem components.
- Stability Assessment: After implant insertion, the elbow is taken through a full range of motion (flexion/extension, pronation/supination) under fluoroscopy. The surgeon assesses radiocapitellar tracking and joint stability, particularly against varus/valgus stress. If an LCL injury was present, it is repaired at this stage.
C. Radial Head Excision - Select Cases
- Historically common, but now largely discouraged due to potential long-term complications (proximal radial migration, valgus instability, post-traumatic osteoarthritis, LCL insufficiency).
- Indications (very limited): Isolated Mason Type III fractures in elderly, very low-demand patients with no associated ligamentous injury or elbow instability, and no evidence of Essex-Lopresti injury.
- Technique: The comminuted radial head is resected flush with the radial neck. Care must be taken to not resect too much bone, which could shorten the radius, or leave sharp edges that could impinge.
Closure
- The capsule is repaired if possible, particularly if a significant capsulotomy was performed.
- If the LUCL was repaired or reconstructed, its integrity is re-checked.
- The deep fascia is repaired.
- Subcutaneous tissues and skin are closed in layers.
-
A sterile dressing and a posterior splint with the elbow at 90 degrees flexion and neutral forearm rotation are applied. For unstable elbows, particularly after LCL repair or in fracture-dislocations, a hinged external fixator or a hinged elbow brace may be considered to allow protected early motion.

Figure 4: Post-operative lateral radiograph following open reduction and internal fixation of a radial head fracture with headless compression screws. Note the anatomical reduction and appropriate screw placement.
Complications & Management
Radial head fracture management, whether operative or non-operative, carries a risk of various complications that can compromise functional outcomes.
Common Complications and Management Strategies
| Complication | Incidence (Approximate) | Description & Management Strategy | Elbow Stiffness/Contracture | 20-50% | The most frequent complication. Stiffening can result from post-traumatic arthrofibrosis, heterotopic ossification (HO), or malunion/nonunion.
Management:
Aggressive physical therapy, dynamic/static progressive splinting. If conservative measures fail, arthroscopic or open arthrolysis with removal of impinging osteophytes or HO may be necessary. Manipulation under anesthesia is considered if severe capsular contracture is the primary issue. |
| Nonunion / Malunion | Rare to 10% (more for complex) | Failure of bone healing or healing in an unacceptable alignment. Can lead to pain, restricted motion, instability, or early arthritis.
Management:
Symptomatic malunions may require corrective osteotomy. Nonunions may require revision ORIF with bone grafting or conversion to radial head arthroplasty, depending on bone quality and functional demands. |
| Heterotopic Ossification (HO) | 10-20% (higher with severe trauma) | Ectopic bone formation in soft tissues around the elbow, leading to progressive loss of motion. More common in fracture-dislocations and patients with TBI/burns.
Management:
Prophylaxis with NSAIDs (e.g., Indomethacin) for 3-6 weeks post-op, or low-dose radiation therapy for high-risk patients. Established HO that limits motion may require surgical excision after maturation (6-12 months). |
| Nerve Injury (PIN/Radial Nerve) | <5% (higher with revision surgery) | Iatrogenic injury during surgical exposure or fixation, particularly to the posterior interosseous nerve (PIN).
Management:
Most neurapraxias recover spontaneously. Observation for 3-6 months. If no recovery, EMG/NCS may be indicated. Surgical exploration and neurolysis may be considered for persistent deficits. |
| Post-Traumatic Arthritis | Varies (higher with articular incongruity) | Progressive degeneration of articular cartilage due to joint incongruity, instability, or malunion.
Management:
Symptomatic management (NSAIDs, activity modification, injections). Advanced arthritis may necessitate revision arthroplasty, total elbow arthroplasty (rare for isolated radial head), or arthrodesis (salvage). |
| Implant-Related Complications | 5-15% (for ORIF or RHA) |
ORIF:
Prominent hardware (impingement with capitellum/ulna), screw loosening/pull-out, fracture around screws.
RHA:
Loosening, subsidence, overstuffing, wear, periprosthetic fracture.
Management:
Symptomatic hardware removal, revision fixation, or revision arthroplasty. Overstuffing may require revision with a smaller prosthesis. |
| Persistent Instability | Varies (higher with LCL injury, excision) | Valgus instability (often due to unaddressed LCL injury or radial head excision), posterolateral rotatory instability, or proximal radial migration (after excision).
Management:
Ligament repair/reconstruction (LCL, LUCL). Conversion from excision to RHA. External fixation in severe cases. |
| Infection | <2% | Superficial or deep surgical site infection.
Management:
Superficial infections respond to oral antibiotics. Deep infections require surgical debridement, intravenous antibiotics, and potentially implant removal/revision. |
| Complex Regional Pain Syndrome (CRPS) | 2-5% | Chronic pain condition characterized by pain, swelling, stiffness, and skin changes.
Management:
Multidisciplinary approach including pain management specialists, physical therapy, sympathetic blocks, and medication (e.g., gabapentin, pregabalin). Early recognition and treatment are key. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing outcomes and minimizing complications, particularly stiffness, following radial head fracture management. Protocols vary based on the specific fracture pattern, surgical intervention, and associated injuries, with stability being the guiding principle.
General Principles
- Early Motion: Generally, early, protected active and passive range of motion (ROM) is encouraged to prevent stiffness and promote cartilage health.
- Pain Control: Adequate pain management is essential to facilitate patient participation in therapy.
- Gradual Progression: Therapy progresses from passive to active-assisted, then active, and finally resistive exercises.
- Ligamentous Stability: If the LCL complex was repaired or reconstructed, ROM may be restricted, particularly limiting extension and varus/valgus stress, to protect the repair.
Non-Operative Management (Mason Type I, Select Type II)
- Immobilization: Sling for comfort for 1-2 weeks.
- Early Phase (Weeks 0-2): Gentle active and passive ROM exercises within pain tolerance. Focus on elbow flexion/extension and forearm pronation/supination. Avoid resisted movements.
- Intermediate Phase (Weeks 2-6): Gradual increase in ROM. Light isometric strengthening exercises. Introduction of low-impact functional activities.
- Late Phase (Weeks 6+): Progressive strengthening with light weights/resistance bands. Gradual return to activities of daily living and work. Full recovery can take 3-6 months.
Open Reduction Internal Fixation (ORIF)
- Immobilization: Posterior splint for 5-7 days for comfort and swelling control, with the elbow at 90 degrees flexion and neutral forearm rotation.
-
Early Phase (Weeks 0-2):
- Initiate gentle active-assisted and active ROM exercises for flexion, extension, pronation, and supination.
- Avoid stressing the repair site; for instance, if the fracture involved the posterior radial head, avoid forceful pronation.
- Gravity-assisted exercises can be beneficial.
- Sling for comfort between exercise sessions.
-
Intermediate Phase (Weeks 2-6):
- Continue to increase ROM as tolerated.
- Introduce light isometric strengthening for elbow flexors/extensors and forearm rotators.
- Initiate scar mobilization.
-
Late Phase (Weeks 6-12):
- Progress to isotonic strengthening with light weights and resistance bands.
- Full ROM should be achievable.
- Gradual return to sport-specific or work-related activities.
- Return to Activity: Typically 3-6 months for most activities, up to 6-12 months for heavy labor or contact sports.
Radial Head Arthroplasty (RHA)
- Immobilization: Similar to ORIF, a posterior splint for 5-7 days. Some surgeons advocate for immediate, protected motion.
-
Early Phase (Weeks 0-2):
- Often more aggressive than ORIF, as the prosthesis provides immediate stability.
- Initiate active-assisted and active ROM for flexion, extension, pronation, and supination.
- If associated ligamentous repairs (LCL, MCL) were performed, motion may be restricted, e.g., in a hinged elbow brace with limits on extension and varus/valgus stress.
-
Intermediate Phase (Weeks 2-6):
- Progress ROM, aiming for near-full motion.
- Begin light isometric strengthening.
-
Late Phase (Weeks 6-12):
- Progress to isotonic strengthening.
- Functional activities.
- Return to Activity: Similar timeline to ORIF, often with quicker progression due to immediate stability of the construct.
Special Considerations for Complex Injuries (e.g., Terrible Triad, LCL Repair)
- Protective Immobilization: Often requires a hinged elbow brace or even dynamic external fixation.
- ROM Restrictions: Specific limitations may be imposed (e.g., avoiding the "danger zone" of 0-30 degrees extension if the LUCL was repaired/reconstructed). Avoid varus/valgus stress.
- Gradual Progression: Rehabilitation is slower and more cautious, with progression based on the stability of the entire reconstructive effort.
- Close Monitoring: Regular clinical and radiographic assessment for signs of instability or loss of reduction.
Throughout all rehabilitation protocols, close communication between the surgeon and the physical therapist is paramount to tailor the program to the individual patient's needs and intraoperative findings.
Summary of Key Literature / Guidelines
The management of radial head fractures has evolved significantly over recent decades, driven by a deeper understanding of elbow biomechanics, improved surgical techniques, and advanced implant technology. Landmark contributions and contemporary guidelines inform current practice.
Classification and Initial Management
The Mason classification , as modified by Hotchkiss, remains the cornerstone for assessing radial head fractures. While Mason Type I fractures are consistently managed non-operatively, the distinction between Mason Type II and III, particularly regarding reconstructibility, is often debated and heavily influenced by imaging, especially CT scans. Early literature, such as Mason and Van Gorder (1937) , focused on simple excision.
Evolution from Excision to Preservation/Replacement
Historically, radial head excision was a common treatment for displaced or comminuted radial head fractures. However, a wealth of literature has highlighted the long-term sequelae of radial head excision, particularly in the presence of associated ligamentous injuries or interosseous membrane disruption. Studies by
Morrey and Chao (1987)
and
Hotchkiss (1996)
emphasized the radial head's critical role in axial load transmission (up to 60% of valgus load) and secondary valgus stability. Uncompensated radial head excision can lead to:
* Proximal radial migration, causing distal radioulnar joint (DRUJ) pain and instability (Essex-Lopresti lesion).
* Progressive valgus instability of the elbow.
* Post-traumatic capitellar degeneration.
This understanding has shifted the paradigm towards either anatomical open reduction and internal fixation (ORIF) for reconstructible fractures or radial head arthroplasty (RHA) for irreparable fractures, especially in unstable elbows.
Open Reduction Internal Fixation (ORIF)
For reconstructible Mason Type II fractures, ORIF with small headless compression screws is the preferred method. Herbert and Fisher (1984) popularized the concept of headless compression screws, which minimize hardware prominence. Ring et al. (2002) provided a comprehensive review of radial head fracture management, emphasizing that ORIF for reconstructible fractures yields good to excellent results in the majority of patients, with low rates of complications when anatomical reduction and stable fixation are achieved. Plates are reserved for more comminuted fractures or specific patterns where screw fixation alone is insufficient.
Radial Head Arthroplasty (RHA)
RHA has emerged as the treatment of choice for irreparable radial head fractures (Mason Type III) and fracture-dislocations (Mason Type IV), particularly in the context of associated ligamentous injuries (e.g., "terrible triad" of elbow dislocation, coronoid fracture, and radial head fracture) or Essex-Lopresti injuries. Popov (1987) and subsequent work by Garrison et al. (2007) and Doornberg and Ring (2014) demonstrated improved outcomes with RHA compared to excision in these complex scenarios, showing better restoration of stability, prevention of proximal radial migration, and improved functional results. There is ongoing research comparing monoblock versus modular prostheses, and stemmed versus non-stemmed designs, with current evidence suggesting good outcomes with both, provided appropriate sizing and surgical technique are employed.
Management of Associated Injuries
The identification and management of concomitant injuries are critical. Hotchkiss (1997) introduced the concept of the "terrible triad" injury, highlighting the importance of addressing all components: radial head fracture, coronoid fracture, and LCL complex injury. Similarly, the Essex-Lopresti injury (radial head fracture, interosseous membrane tear, DRUJ disruption) necessitates radial head replacement to restore forearm length and prevent long-term wrist and elbow dysfunction. Failure to address these associated injuries can lead to persistent instability and poor functional outcomes, even if the radial head fracture itself is adequately treated.
Rehabilitation Guidelines
Current rehabilitation protocols emphasize early, protected range of motion to prevent stiffness while safeguarding the surgical repair or implant. Coonrad and Morrey (1994) established a foundation for early mobilization protocols for elbow fractures. Modifications are made for specific ligamentous repairs (e.g., LCL repair often requires a hinged brace limiting extension and varus stress) to prevent re-injury.
Future Directions
Ongoing research focuses on biomechanical studies to refine implant design, optimize surgical approaches, and further delineate the indications for various treatment modalities. Long-term outcome studies comparing ORIF, RHA, and excision in specific patient cohorts continue to provide valuable insights into durability and functional restoration. The role of advanced imaging, particularly CT-based surgical planning and intraoperative navigation, is also evolving.
Clinical & Radiographic Imaging

