Distal Femoral Fractures: Epidemiology, Anatomy, Biomechanics, and Surgical Principles
Key Takeaway
Distal femoral fractures (DFX) occur near the knee. Management involves anatomical reduction, stable fixation, and alignment restoration, guided by AO/OTA classification. Understanding surgical anatomy, biomechanics, and neurovascular risks is crucial for optimizing outcomes, restoring joint mechanics, and preventing post-traumatic arthritis and stiffness.
Introduction & Epidemiology
Distal femoral fractures (DFX), defined as fractures of the femur within 9 cm of the knee joint line, represent a significant orthopedic challenge. These injuries typically involve the supracondylar or intercondylar regions of the distal femur. Their incidence exhibits a bimodal distribution: predominantly high-energy trauma in younger, active individuals (e.g., motor vehicle collisions, falls from height) and low-energy falls in the elderly, often osteoporotic population. The rising global prevalence of osteoporosis contributes to an increasing incidence of DFX in older adults.
These fractures are frequently associated with substantial soft tissue damage, articular incongruity, and potential neurovascular compromise, particularly with high-energy mechanisms. Given their proximity to the knee joint, stable anatomical reduction is paramount to restore joint mechanics, preserve limb function, and prevent long-term sequelae such as post-traumatic arthritis and stiffness. Urgent and meticulous assessment, followed by appropriate surgical intervention, is critical for optimal patient outcomes. Initial management adheres to Advanced Trauma Life Support (ATLS) principles, including provisional stabilization with a splint or traction, thorough neurovascular assessment, and pain control. Open fractures necessitate immediate debridement and antibiotic prophylaxis.
The primary classification system utilized for distal femoral fractures is the AO/OTA classification, which categorizes fractures based on their articular involvement and comminution:
*
Type A:
Extra-articular (supracondylar).
*
Type B:
Partial articular (involving one condyle).
*
Type C:
Complete articular (involving both condyles and the metaphysis).
This framework guides surgical decision-making and prognostication, highlighting the increasing complexity and demands for anatomical reduction as articular involvement increases.
Surgical Anatomy & Biomechanics
A profound understanding of distal femoral anatomy and regional biomechanics is foundational for successful surgical management of DFX.
Bone Anatomy
The distal femur transitions from a cylindrical shaft proximally to a flattened, broad metaphysis and epiphysis distally, forming the two femoral condyles.
*
Medial Condyle:
Larger, more prominent, extends further distally than the lateral condyle. Bears a greater proportion of weight in standing.
*
Lateral Condyle:
Provides stability and articulation with the tibia.
*
Intercondylar Notch:
Houses the anterior and posterior cruciate ligaments.
*
Supracondylar Region:
The flare of the metaphysis where cortical bone thins, making it a common site for fracture.
*
Blood Supply:
Primarily via the descending genicular artery (branch of superficial femoral artery), superior genicular arteries (medial and lateral, branches of popliteal artery), and the periosteal plexus. Extensive surgical dissection can compromise this delicate vascularity, particularly in the distal fragment.
Ligamentous and Muscular Influences
- Cruciate Ligaments (ACL, PCL): Attach within the intercondylar notch. Articular fractures can disrupt their attachments.
- Collateral Ligaments (MCL, LCL): Stabilize the knee joint medially and laterally. Their integrity must be assessed, especially with condylar fractures.
- Gastrocnemius Muscle: Originates from the posterior aspect of the femoral condyles. Its strong pull can result in apex posterior angulation and shortening of the distal fragment, making reduction challenging.
- Quadriceps Femoris: Comprised of rectus femoris, vastus medialis, vastus lateralis, and vastus intermedius. These muscles exert traction on the patella and patellar tendon, influencing the position of the distal fragment during knee motion.
- Adductors and Hamstrings: Contribute to rotational and translational deformities.
Neurovascular Anatomy
The popliteal artery and vein traverse the popliteal fossa, immediately posterior to the distal femur. The tibial nerve and common peroneal nerve are also in close proximity. High-energy DFX, particularly those with significant displacement or posterior angulation, carry a substantial risk of neurovascular injury (e.g., popliteal artery intimal tear or transection, common peroneal nerve stretch). Thorough preoperative and intraoperative neurovascular assessment is mandatory.
Biomechanics of Fracture Patterns
The interplay of bone morphology and muscular forces dictates common fracture patterns:
*
Supracondylar (Type A):
Often transverse or oblique. Gastrocnemius pull causes posterior tilt of the distal fragment.
*
Intercondylar (Type C):
Involve the articular surface, often T- or Y-shaped patterns. Shear forces, impaction, and direct trauma contribute to comminution.
*
Condylar (Type B):
Pure unicondylar fractures result from direct axial or valgus/varus loads.
*
Bone Quality:
Osteoporotic bone in elderly patients often leads to highly comminuted, unstable fractures, challenging stable fixation. The biomechanical demands on fixation implants are significant due as the distal femur transmits substantial axial and rotational loads during weight-bearing. Restoration of articular congruity and mechanical axis is critical to distribute these loads evenly across the knee joint and prevent post-traumatic arthrosis.
Indications & Contraindications
The decision between operative and non-operative management for distal femoral fractures is complex and depends on multiple factors, including fracture characteristics, patient comorbidities, functional demands, and soft tissue status.
Operative Indications
Surgical intervention is the gold standard for most displaced distal femoral fractures. The primary goals are anatomical reduction (especially of the articular surface), stable internal fixation, restoration of limb alignment, length, and rotation, and early functional rehabilitation.
- Displaced Articular Fractures (AO/OTA Type B or C): Any displacement or incongruity of the articular surface requires operative intervention to restore joint anatomy and minimize the risk of post-traumatic arthritis.
- Displaced Extra-articular Fractures (AO/OTA Type A): Significant angulation (>5-10 degrees), shortening (>1 cm), or rotational deformity warrants surgical correction to restore the mechanical axis and functional limb length.
- Open Fractures: Require urgent surgical debridement, irrigation, and stabilization to prevent infection and facilitate soft tissue management.
- Fractures with Neurovascular Compromise: Mandate immediate surgical exploration, reduction of fracture, and repair of any injured neurovascular structures.
- Polytrauma Patients: Early stable fixation facilitates mobilization, reduces complications (e.g., DVT/PE, ARDS), and aids nursing care.
- Ipsilateral Tibia Fracture (Floating Knee): Both fractures typically require stable fixation for optimal rehabilitation.
- Failed Non-Operative Management: Progressive displacement or non-union during conservative treatment.
- Pathologic Fractures: Often require surgical stabilization for pain relief and improved weight-bearing capacity.
Non-Operative Indications
Non-operative management is reserved for a select group of patients and fracture patterns.
- Minimally Displaced, Stable Extra-articular Fractures: In non-ambulatory or very low-demand patients where acceptable alignment can be maintained with external support (e.g., brace, cast).
- Medically Unstable Patients (ASA Class IV/V): Where the risks of anesthesia and surgery significantly outweigh the potential benefits of operative fixation. Limited options like external fixation or palliative care may be considered.
- Severe Local Soft Tissue Compromise: Where immediate internal fixation is contraindicated due to a high risk of wound complications or infection. Temporary external fixation may be used as a bridge to definitive internal fixation.
- Palliative Care: In patients with limited life expectancy or severe comorbidities, comfort and pain management may supersede aggressive surgical intervention.
Contraindications (Relative)
- Active Local Infection: Relative contraindication to internal fixation; may require debridement, antibiotics, and delayed fixation.
- Uncontrolled Systemic Infection (Sepsis): Surgical deferral until systemic infection is managed.
- Severe Soft Tissue Compromise: Open wounds, large degloving injuries, or extensive crush injury may necessitate temporary external fixation or delayed definitive management.
- Extreme Comminution: In some rare cases, particularly in severely osteoporotic elderly patients with highly comminuted articular fractures, the bone stock may be insufficient for stable internal fixation. Primary total knee arthroplasty (TKA) might be considered as a salvage or definitive procedure in such situations, though its use as a primary intervention for acute DFX remains controversial and restricted to highly selected cases.
Operative vs. Non-Operative Indications Summary Table
| Indication Type | Specific Condition | Rationale |
|---|---|---|
| Operative | Displaced articular fractures (AO/OTA B, C) | Restore joint congruity, prevent post-traumatic arthritis, facilitate early ROM. |
| Displaced extra-articular fractures (AO/OTA A) | Restore mechanical axis, length, rotation, achieve stable union, enable weight-bearing. | |
| Open fractures (Gustilo-Anderson > Type I) | Urgent debridement, irrigation, stabilization to prevent infection. | |
| Neurovascular compromise | Direct repair/decompression required for limb salvage. | |
| Polytrauma patients | Facilitate early mobilization, reduce DVT/PE, pneumonia, ARDS risk. | |
| Ipsilateral tibia fracture / "Floating knee" | Require stable fixation for comprehensive rehabilitation. | |
| Pathologic fractures | Pain relief, prevent further collapse, enable controlled weight-bearing. | |
| Failed non-operative management | Progressive displacement or non-union indicates need for surgical stabilization. | |
| Non-Operative | Minimally displaced, stable extra-articular fractures | Acceptable alignment, minimal risk of further displacement, especially in low-demand patients. |
| Non-ambulatory, low-demand patients | Functional outcome may not be significantly improved by surgery; comfort care. | |
| Medically unstable patients (ASA IV/V) | High perioperative risk outweighs benefits of surgical fixation; consider limited external fixation or hospice. | |
| Severe, uncontrolled local infection | Risk of hardware infection; requires staged approach or non-operative limb care. | |
| Palliative care situations | Symptomatic management and comfort are primary goals. |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is indispensable for successful outcomes in distal femoral fractures. This stage integrates detailed imaging analysis, templating, and strategic decision-making regarding implant choice and surgical approach.
Imaging Modalities
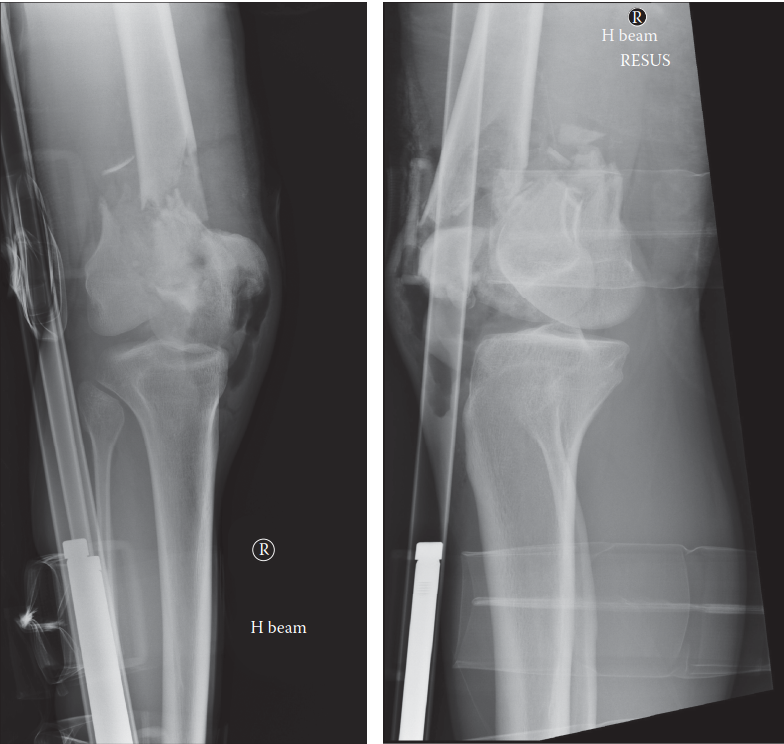
- Standard Radiographs: AP and Lateral views of the knee and entire femur (including hip and ankle for mechanical axis assessment) are initial requirements. Traction radiographs can provide valuable information regarding fracture reducibility.
- Computed Tomography (CT) Scan: Essential for all articular fractures (AO/OTA Type B and C) and highly comminuted extra-articular fractures. CT with 3D reconstructions provides detailed information regarding fragment size, displacement, articular step-off, and associated impaction, guiding surgical strategy.
- Magnetic Resonance Imaging (MRI): Rarely indicated for acute DFX, but can be useful to assess associated ligamentous injuries (e.g., ACL/PCL tears) or occult osteochondral injuries if clinical suspicion remains after fixation.
- Arteriography: Indicated if there is clinical suspicion of vascular injury (e.g., diminished pulses, expanding hematoma, Doppler flow abnormalities, high-energy injury mechanism with significant displacement).
Templating and Surgical Strategy
Templating involves using radiographic images to pre-plan the surgical procedure. This includes:
*
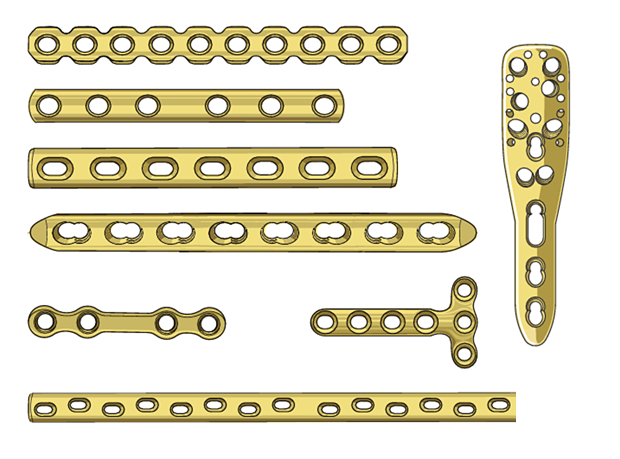
Implant Selection:
Determining the appropriate length, contour, and type of plate (e.g., lateral locking plate, antegrade/retrograde intramedullary nail).
*
Screw Trajectory:
Pre-planning screw placement to maximize purchase in the distal fragments, avoiding joint penetration.
*
Reduction Maneuvers:
Identifying specific reduction tools (e.g., distractors, external fixators, pointed reduction clamps, temporary K-wires) and sequences for fragment manipulation.
*
Bone Grafting:
Assessing the need for bone grafting in cases of significant metaphyseal comminution or bone loss.

Integrating detailed templating for distal femoral fractures, such as determining plate length, screw trajectories, and potential reduction strategies, is crucial. This image exemplifies various fracture patterns and appropriate implant choices, facilitating precise pre-operative planning for restoration of anatomical alignment and joint congruity.
The surgical strategy considers the chosen approach:
*
Open Reduction Internal Fixation (ORIF):
Allows direct visualization and anatomical reduction, particularly critical for articular fractures. Requires more extensive soft tissue dissection.
*
Minimally Invasive Plate Osteosynthesis (MIPO):
Utilizes indirect reduction techniques and submuscular plate insertion to preserve soft tissue vascularity, advantageous for comminuted metaphyseal fractures.
*
Retrograde Intramedullary Nailing (RIMN):
A load-sharing device, often favored for extra-articular supracondylar fractures (AO/OTA A types) or in certain geriatric patients due to its biological advantages, but less suitable for articular involvement.
Patient Optimization and Positioning
- Medical Optimization: Address any underlying medical comorbidities (diabetes, hypertension, cardiac disease). Optimize nutrition, manage pain, and administer appropriate DVT prophylaxis and perioperative antibiotics.
- Patient Positioning: The patient is typically positioned supine on a radiolucent operating table. A bump may be placed under the ipsilateral hip to facilitate positioning. For fractures requiring intraoperative traction (e.g., for length restoration), a fracture table may be used, although this can restrict C-arm access. The knee should be allowed to flex to approximately 90 degrees to facilitate reduction and implant placement. The entire limb should be prepped and draped to allow free manipulation of the knee and ankle and to permit long-leg alignment checks with the C-arm. Ensure unimpeded access for the C-arm to obtain AP, lateral, and oblique views throughout the procedure, particularly for checking articular reduction and implant position.
Detailed Surgical Approach / Technique
The goal of surgical fixation is anatomical reduction of the articular surface, restoration of the mechanical axis, limb length, and rotation, and stable fixation to permit early rehabilitation.
General Principles
- Articular Reduction First: For articular fractures (Type B and C), prioritize reduction and temporary fixation of the articular fragments.
- Restore Length, Alignment, Rotation: Once the articular block is reconstructed, attention shifts to re-establishing the relationship between the articular segment and the femoral shaft.
- Stable Fixation: Employ implants that provide sufficient stability for the specific fracture pattern and bone quality, typically locking plates.
- Preserve Biology: Minimize soft tissue stripping, particularly in the distal fragment, to maintain vascularity. MIPO techniques are favored when appropriate.
Surgical Approaches
-
Lateral Approach (Lateral Subvastus or Minimally Invasive):
- Incision: A straight lateral incision centered over the distal femur, extending proximally along the shaft and distally to the lateral epicondyle or joint line. Length varies based on fracture complexity and chosen technique (ORIF vs. MIPO).
- Internervous Plane: The critical plane is between the vastus lateralis (anteriorly) and the lateral intermuscular septum/biceps femoris (posteriorly).
-
Dissection:
- Standard Lateral: Incise the fascia lata. Develop the interval between the vastus lateralis and the lateral intermuscular septum. The vastus lateralis is then either split longitudinally or, preferably, elevated anteriorly as a subvastus approach, preserving its innervation and blood supply. This exposes the lateral femoral shaft and condyle. Care must be taken to preserve the perforating vessels from the profunda femoris artery that enter the vastus lateralis.
- MIPO (Subvastus/Minimally Invasive): A smaller distal incision is made. The vastus lateralis is elevated subperiosteally or submuscularly from the lateral femoral cortex. A subcutaneous tunnel is created proximally for plate insertion. This minimizes soft tissue disruption but relies on indirect reduction techniques.
- Exposure: Provides excellent access to the lateral aspect of the distal femur, supracondylar region, and lateral condyle. This is the most common approach for plating distal femoral fractures.
-
Anteromedial Approach:
- Indications: Less common as a primary approach, but may be used for medial condyle fractures (rare) or for specific reduction maneuvers, or in conjunction with a lateral approach for bicondylar fixation.
- Internervous Plane: Between the vastus medialis (lateral) and the sartorius/gracilis (medial).
- Exposure: Provides access to the medial femoral condyle and supracondylar region. Requires careful identification and protection of the saphenous nerve and vein.
-
Posterior Approach:
- Indications: Rarely used for primary fixation of distal femoral fractures, typically reserved for removal of posteriorly placed hardware or for very specific posterior condylar fragments.
- Risks: High risk of injury to the popliteal neurovascular bundle.
Reduction Techniques
- Articular Reconstruction: For articular (Type B, C) fractures, the joint surface must be reconstructed first. Fragments are anatomically reduced under direct visualization and temporarily fixed with small K-wires. Fluoroscopy is used to confirm articular congruity and ensure no K-wires penetrate the joint.
-
Restoring Length and Alignment:
- Traction: Manual longitudinal traction or skeletal traction via a distal tibia pin (external fixator, femoral distractor) can help restore length and de-rotate the main fragments.
- Direct Manipulation: Large fragment clamps (e.g., Verbrugge, Farabeuf) can be used to achieve provisional reduction of the articular block to the femoral shaft.
- Indirect Reduction: For MIPO, reduction is achieved indirectly using ligamentotaxis, external fixators as joysticks, or percutaneous clamps. Fluoroscopy guides the process, aiming for correct length, alignment (valgus/varus, apex anterior/posterior), and rotation.
- De-rotation: The patella is used as a rotational guide; it should point straight anteriorly when the hip and knee are flexed to 90 degrees.
- Provisional Fixation: Once reduction is achieved, temporary fixation with K-wires or large cerclage wires may be used to hold the reduction while the definitive implant is applied.
Fixation Strategies
-
Lateral Locking Plate (LCP Distal Femur Plate):
- Principle: A fixed-angle construct that provides angular stability, crucial in comminuted metaphyseal fractures and osteoporotic bone. Functions as a bridge plate or compression plate depending on the fracture pattern.
-
Application:
- Contour the plate to match the anatomy of the lateral distal femur.
- Place the plate submuscularly via a MIPO technique or directly on the bone via an open approach.
- Distal Fixation: Place multiple locking screws into the distal articular block. Screws should be divergently aimed to capture as many fragments as possible and achieve bicortical purchase if feasible. Ensure no screws penetrate the articular surface; this is confirmed with intraoperative fluoroscopy in multiple planes (AP, lateral, obliques).
- Proximal Fixation: Place at least 3-4 locking screws into the femoral shaft proximally. Aim for a long plate with a good working length (empty holes) across the comminuted zone to allow for micro-motion and promote secondary bone healing.
- Compression (optional): For simple transverse or short oblique fractures, a lag screw through the plate or a compression screw in a dynamic compression unit (DCU) hole can provide interfragmentary compression before locking screws are inserted.
- Positioning: The plate is usually placed slightly posterior to the midline on the lateral aspect of the femur to optimize screw trajectories into the condyles and avoid the intercondylar notch.
-
Retrograde Intramedullary Nailing (RIMN):
- Indications: Primarily for extra-articular supracondylar fractures (AO/OTA A types) or some minimally displaced partial articular fractures. Less ideal for significantly comminuted or displaced articular fractures where anatomical reduction of the joint surface is paramount.
-
Technique:
- Entry Point: The nail is typically inserted through the intercondylar notch (between the femoral condyles) or, less commonly, through the medial or lateral condyle. Intercondylar entry risks patellar chondral damage or avascular necrosis of the patella.
- Nail Insertion: Guide wire insertion, reaming, and nail insertion proceeds proximally into the femoral shaft.
- Distal Locking: Multiple locking screws are placed from medial to lateral (and sometimes anterior to posterior) to capture the distal fragment.
- Proximal Locking: Standard proximal locking screws provide rotational stability.
- Advantages: Load-sharing, less soft tissue stripping, potential for faster union.
- Disadvantages: Limited ability to control articular fragments, risk of malalignment (valgus, apex anterior) due to fixed entry point and challenging rotation control.
-
Combined Techniques: For complex bicondylar fractures (Type C), a combination of lag screws for articular reconstruction and then plate fixation (often lateral LCP) for metadiaphyseal stability is common.
-
Bone Grafting: Autogenous bone graft (e.g., from iliac crest) or allograft can be used to fill significant metaphyseal defects, particularly in cases of severe comminution or non-unions, to promote healing.
Assessment of Fixation
- Intraoperative Fluoroscopy: Obtain meticulous AP, lateral, and oblique views to confirm anatomical reduction, correct alignment, appropriate implant position, and absence of intra-articular screw penetration.
- Stability Assessment: Manually stress the fracture to ensure robust fixation.
- Wound Closure: Layered closure of the muscle fascia, subcutaneous tissue, and skin. Drain placement is controversial and typically reserved for cases with significant bleeding or dead space.
Complications & Management
Distal femoral fractures, even with optimal surgical management, are associated with a range of potential complications, which can significantly impact patient outcomes. Vigilant post-operative monitoring and prompt intervention are critical.
General Surgical Complications
- Infection: Superficial or deep wound infection.
- Thromboembolic Events: Deep vein thrombosis (DVT) and pulmonary embolism (PE).
- Nerve Injury: Most commonly the common peroneal nerve or saphenous nerve.
- Vascular Injury: Popliteal artery or vein injury, especially with severe displacement.
- Hemorrhage: Intraoperative or post-operative bleeding.
- Anesthetic Complications: General risks associated with anesthesia.
Specific Complications and Management Strategies
| Complication | Incidence | Management / Salvage Strategy |
|---|---|---|
| Non-union | 5-15% |
Definition:
Failure of fracture to achieve radiographic union within 6-9 months, with persistent motion at the fracture site.
Management: Comprehensive workup to identify underlying causes (e.g., infection, inadequate stability, biology). Revision surgery is often required, involving: 1. Enhanced Stability: Plate exchange (e.g., longer, stiffer plate), intramedullary nailing (e.g., exchange nailing from retrograde to antegrade if applicable), or hybrid constructs. 2. Biologic Enhancement: Autogenous bone grafting (e.g., iliac crest aspirate or structural graft) for bone defects or atrophic non-unions. Biologic augmentation with bone morphogenetic proteins (BMPs) may be considered in specific cases. 3. Infection Exclusion: Thorough investigation for occult infection prior to or during revision. |
| Malunion | 10-20% |
Definition:
Healing of the fracture in an unacceptable anatomical or functional alignment (e.g., excessive angulation, rotation, shortening).
Management: 1. Asymptomatic/Mild: Observation, physiotherapy. 2. Symptomatic (Pain, gait disturbance, joint overload): Corrective osteotomy (supracondylar or intra-articular), with rigid internal fixation, to restore mechanical axis. 3. Severe Intra-articular Malunion with Arthritis: Total Knee Arthroplasty (TKA) may be considered, often requiring complex primary or revision TKA techniques due to distorted anatomy and bone loss. |
| Infection | 1-5% |
Definition:
Presence of bacterial colonization in the wound or around hardware. Incidence higher in open fractures.
Management: 1. Superficial: Oral antibiotics, local wound care. 2. Deep: Urgent surgical debridement, copious irrigation, deep tissue cultures, appropriate targeted IV antibiotics (often prolonged course). Depending on stability and host factors: - Retain Hardware: If fracture is stable and infection controlled early. - Staged Protocol: If infection is severe or chronic: hardware removal, extensive debridement, antibiotic spacer, delayed re-implantation or definitive fixation once infection is eradicated. |
| Stiffness / Arthrofibrosis | 20-30% |
Definition:
Restricted range of motion (ROM) of the knee joint due to capsular contracture, scarring, or heterotopic ossification.
Management: 1. Early: Aggressive, physician-supervised physical therapy, continuous passive motion (CPM) machine. 2. Persistent: Manipulation under anesthesia (MUA) if ROM plateaued and pain is acceptable. 3. Chronic: Arthroscopic or open arthrolysis, quadricepsplasty for severe quadriceps contracture. |
| Post-traumatic Arthritis | 10-25% |
Definition:
Degenerative changes of the knee joint following intra-articular fracture, due to articular incongruity, cartilage damage, or malalignment. Higher incidence in Type B and C fractures.
Management: 1. Conservative: Activity modification, NSAIDs, intra-articular injections (corticosteroids, hyaluronic acid). 2. Surgical: Unicompartmental or Total Knee Arthroplasty (TKA), often technically demanding due to retained hardware, distorted anatomy, and bone deficits. |
| Hardware Failure | Varies (e.g., 5-10% in osteoporosis) |
Definition:
Bending, breakage, or loosening of implants (plate, screws). Often indicative of non-union or excessive early loading.
Management: Revision surgery, often involving removal of failed hardware, achieving stable reduction, applying a stronger construct (e.g., longer, thicker plate, different implant type), and frequently incorporating bone grafting for underlying non-union. |
| Neurovascular Injury | 1-3% |
Definition:
Injury to the popliteal artery/vein or peroneal/tibial nerves.
Management: Urgent surgical exploration. 1. Vascular: Repair (primary anastomosis, interposition vein graft), fasciotomy if compartment syndrome develops. 2. Nerve: Decompression, direct repair if transected (often with delayed recovery or permanent deficit). |
| Avascular Necrosis (AVN) of Patella | Rare (with specific nailing techniques) |
Definition:
Ischemic death of patellar bone, typically associated with intercondylar entry for retrograde nails.
Management: Conservative initially for symptomatic relief. For severe, symptomatic cases, patellectomy or partial patellectomy may be considered. |
| Implant Prominence / Soft Tissue Irritation | Common, but highly variable |
Definition:
Pain or discomfort due to palpable hardware or irritation of overlying soft tissues.
Management: Hardware removal (HWR) after radiographic and clinical union of the fracture is achieved, typically 12-24 months post-operatively. |
| Complex Regional Pain Syndrome (CRPS) | < 5% |
Definition:
Chronic neuropathic pain syndrome characterized by pain, swelling, and autonomic dysfunction disproportionate to the injury.
Management: Multidisciplinary approach involving pharmacotherapy (gabapentin, tricyclics), physical therapy, nerve blocks, and psychological support. Early diagnosis and intervention are key. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a crucial determinant of functional outcome following distal femoral fracture fixation. Protocols are individualized based on fracture stability, bone quality, type of fixation, and patient-specific factors. The goal is to maximize joint range of motion, restore muscle strength, and facilitate safe return to activity while protecting the healing fracture.
Phase 1: Early Post-Operative (Weeks 0-6)
- Goals: Control pain and swelling, protect fracture fixation, initiate early range of motion (ROM), prevent stiffness, and maintain muscle tone in surrounding unaffected areas.
-
Weight Bearing (WB):
- NWB (Non-Weight Bearing) or TDWB (Touch-Down Weight Bearing, <10-15 kg): For unstable fractures, highly comminuted fractures, or those with tenuous fixation, and for most articular fractures.
- PWB (Partial Weight Bearing): For stable, well-fixed extra-articular fractures in good bone quality.
- Guidance: Patients are educated on protected weight bearing using crutches or a walker.
-
Range of Motion (ROM):
- CPM Machine: May be used to facilitate gentle, controlled ROM.
- Active-Assisted & Gentle Active ROM: Initiate within a pain-free arc, typically aiming for 0-90 degrees knee flexion by 6 weeks post-op. Avoid forced ROM.
- Patellar Mobilization: Gentle patellar glides to prevent infrapatellar contracture.
-
Muscle Strengthening:
- Isometric Exercises: Quadriceps sets, gluteal sets, hamstring sets, ankle pumps (to prevent DVT).
- Avoid: Active knee extension against resistance or straight leg raises if quadriceps pull might stress the fracture.
- Wound Care: Monitor for signs of infection, regular dressing changes.
- Edema Control: Elevation, compression stockings.
Phase 2: Intermediate Post-Operative (Weeks 6-12)
- Goals: Gradually increase weight bearing, improve ROM, restore muscle strength, and enhance proprioception.
-
Weight Bearing (WB):
- Progressive Weight Bearing (PWB to FWB): Gradual progression to full weight bearing as radiographic signs of healing appear and pain tolerance allows. Typically starts around 6-8 weeks for stable fractures, potentially later for more complex cases.
- Guidance: Wean off assistive devices as strength and balance improve.
-
Range of Motion (ROM):
- Continue to increase knee flexion and extension. Aim for functional ROM (0-120 degrees) by 12 weeks.
- Gentle stretching for hamstring and quadriceps flexibility.
-
Muscle Strengthening:
- Isotonic Exercises: Leg presses, hamstring curls, knee extensions with light resistance (progress cautiously), calf raises.
- Closed-Chain Exercises: Partial squats, mini-lunges (as tolerated, once PWB is established).
- Proprioception: Balance exercises (single-leg stance, wobble board).
- Aerobic Conditioning: Stationary cycling (high seat, low resistance) can begin as ROM permits.
Phase 3: Late Post-Operative (Beyond 12 Weeks)
- Goals: Achieve full functional ROM and strength, return to pre-injury activity levels, prevent re-injury.
- Weight Bearing (WB): Full weight bearing, no restrictions.
- Range of Motion (ROM): Should be near-normal, if not full. Continue stretching to maintain flexibility.
-
Muscle Strengthening:
- Advanced Strengthening: Progressive resistance exercises, plyometrics, sport-specific training.
- Endurance: Increase duration and intensity of aerobic activities.
-
Return to Activity:
- Gradual return to recreational and occupational activities.
- High-impact activities and contact sports are typically delayed until 6-12 months post-operatively, after complete radiographic union and full strength recovery are confirmed.
- Hardware removal may be considered for symptomatic implants after complete union, typically around 12-24 months. This necessitates another brief period of protected weight bearing.
Important Considerations
- Individualization: Protocols must be tailored. Elderly patients with osteoporotic bone or complex medical comorbidities may have slower progression.
- Pain Management: Effective pain control is essential for participation in rehabilitation.
- Radiographic Monitoring: Serial radiographs guide weight-bearing progression.
- Patient Compliance: Education and motivation are key to adherence to the rehabilitation program.
- Complications: Be vigilant for signs of stiffness, non-union, or infection, which may require modification of the rehabilitation plan.
Summary of Key Literature / Guidelines
The management of distal femoral fractures has evolved significantly with advancements in implant technology and surgical techniques. Several key principles and evidence-based findings guide current practice.
AO Principles
The AO Foundation's long-standing principles for fracture management remain fundamental:
*
Anatomical Reduction:
Especially crucial for articular surfaces to restore joint congruity and kinematics.
*
Stable Fixation:
To allow for early, pain-free mobilization.
*
Preservation of Blood Supply:
Achieved through careful soft tissue handling, indirect reduction techniques (MIPO), and biologic plating strategies.
*
Early, Safe Mobilization:
To prevent joint stiffness, muscle atrophy, and systemic complications.
Locking Plate Technology
Modern lateral locking compression plates (LCP DFF) have become the workhorse for distal femoral fracture fixation.
*
Advantages:
Fixed-angle construct provides angular stability independent of plate-to-bone compression, making them highly effective in osteoporotic bone and comminuted fractures where traditional lag screws and compression plates may fail. The submuscular application (MIPO) technique preserves periosteal blood supply, enhancing biologic healing.
*
Evidence:
Numerous studies support the use of locking plates, demonstrating improved outcomes and lower failure rates compared to conventional plates, particularly in geriatric and highly comminuted fractures. However, technical errors in plate positioning or screw placement can still lead to complications.
Retrograde Intramedullary Nailing (RIMN) vs. Plating
- RIMN: Often preferred for extra-articular supracondylar fractures (AO/OTA Type A) due to its load-sharing nature, less soft tissue disruption, and potential for faster union. It is less suitable for complex articular fractures (Type B, C) where precise articular reduction is paramount, as the nail cannot directly control small articular fragments. Potential complications include patellar pain, avascular necrosis of the patella (with intercondylar entry), and malalignment (valgus, apex anterior) if not precisely inserted.
- Plating: Generally preferred for intra-articular fractures (Type B, C) where anatomical reduction of the joint surface requires direct visualization and precise screw placement. Plating also allows for better control of rotation and coronal/sagittal plane alignment in complex comminuted fractures.
- Comparative Studies: Meta-analyses show generally comparable outcomes between RIMN and locking plates for specific Type A fractures, but plates tend to be superior for articular involvement. The choice often hinges on fracture morphology, surgeon preference, and patient factors.
Management of Geriatric Fractures
- Challenges: Elderly patients with DFX often present with osteoporotic bone, multiple comorbidities, and limited physiologic reserve. This leads to higher rates of non-union, malunion, and systemic complications.
- Guidelines: Emphasize early surgical intervention (within 24-48 hours if medically optimized) to facilitate early mobilization and reduce complications. Multidisciplinary co-management with geriatric medicine specialists is increasingly recommended to optimize medical status pre- and post-operatively.
- Primary Arthroplasty: In select elderly patients with severely comminuted intra-articular fractures and pre-existing arthritis where stable fixation is unlikely or joint reconstruction is deemed futile, primary total knee arthroplasty (TKA) or distal femoral replacement (DFR) may be considered as a salvage or definitive procedure, though this remains a niche indication.
Open Fractures
- Gustilo-Anderson Classification: Guides the management of open DFX, emphasizing urgent debridement and irrigation within 6-8 hours, appropriate broad-spectrum intravenous antibiotics, and tetanus prophylaxis.
- Fixation: Stable internal fixation is usually preferred after adequate debridement, possibly with a staged approach (external fixator first, then definitive internal fixation).
Current Trends and Future Directions
- Enhanced Recovery After Surgery (ERAS) Protocols: Integrating multimodal pain management, early mobilization, and optimized nutrition to accelerate recovery and reduce hospital stays.
- Biologic Augmentation: The use of bone morphogenetic proteins (BMPs) or platelet-rich plasma (PRP) is being explored to enhance healing, particularly in high-risk fractures or non-unions, though robust evidence for routine use in acute DFX is still evolving.
- Patient-Specific Implants: Custom-designed implants based on pre-operative CT scans may offer superior fit and fixation in complex cases, but are not yet standard practice.
- Navigation and Robotics: Increasingly being investigated for precision in implant placement and alignment, especially for articular reconstructions.
In summary, the optimal management of distal femoral fractures relies on a comprehensive understanding of anatomy, biomechanics, meticulous pre-operative planning, precise surgical execution using modern implants and techniques, and an aggressive, yet protected, post-operative rehabilitation protocol. Continuous evaluation of outcomes and adaptation to evolving evidence are essential to achieve the best possible results for patients with these challenging injuries.
You Might Also Like