Adolescent Distal Tibial Tillaux & Triplane Fractures: Pathophysiology, Diagnosis, and Management

Key Takeaway
Tillaux and Triplane fractures are unique intra-articular distal tibia injuries in adolescents. Tillaux (Salter-Harris III) is an epiphyseal avulsion. Triplane (Salter-Harris IV) is a complex multi-planar injury involving epiphysis, physis, and metaphysis. Their occurrence depends on specific physeal closure stages, demanding precise reduction to prevent complications.
Introduction & Epidemiology
Distal tibia fractures in adolescents represent a unique challenge due to the specific anatomy of the distal tibial physis and its closure pattern. Among these, Tillaux and Triplane fractures are distinct intra-articular injuries that typically occur during the transition period of physeal closure. Understanding their complex three-dimensional morphology and mechanism of injury is paramount for accurate diagnosis and effective management.
Tillaux fractures are Salter-Harris type III injuries, characterized by an avulsion fracture of the anterolateral distal tibial epiphysis. They typically occur in older adolescents, usually females between 12-14 years and males between 13-15 years, when the central and medial aspects of the distal tibial physis have already begun to fuse, leaving the lateral portion vulnerable. The mechanism commonly involves an external rotation force with the foot in dorsiflexion, leading to avulsion of the epiphyseal fragment by the strong anterior inferior tibiofibular ligament (AITFL).
Triplane fractures are complex, multifragmentary intra-articular fractures involving the epiphysis, physis, and metaphysis. They are classically described as Salter-Harris type IV injuries, though their unique multiplanar nature warrants a distinct classification. These fractures occur slightly earlier in adolescence than Tillaux fractures, typically in females aged 10-13 years and males aged 12-15 years, during an earlier stage of physeal closure where the central physis has begun to fuse but significant medial and lateral portions remain open. The injury results from a combined torsional and axial load, often an external rotation force, creating fracture lines in sagittal, coronal, and transverse planes. The pattern of physeal closure dictates the specific configuration, often involving a coronal plane fracture through the metaphysis, a transverse plane fracture through the physis, and a sagittal plane fracture through the epiphysis. Triplane fractures are classified based on the number of fragments observed on plain radiographs or, more accurately, on computed tomography (CT) scans, commonly into two-, three-, or four-part variants.
The incidence of distal tibia fractures in adolescents accounts for approximately 10-15% of all pediatric long bone fractures, with Tillaux and Triplane fractures representing a significant proportion of these intra-articular injuries. Due to their intra-articular nature and the involvement of the growth plate, precise anatomical reduction is critical to prevent long-term complications such as growth arrest, angular deformity, and post-traumatic arthritis.
Surgical Anatomy & Biomechanics
Mastery of Tillaux and Triplane fractures necessitates an intimate understanding of the distal tibial physeal anatomy, its unique closure pattern, and the biomechanical forces at play.
Distal Tibial Physis Closure
The distal tibial physis undergoes an asymmetrical, predictable pattern of closure, which is central to the pathophysiology of these injuries. Closure typically begins centrally, then progresses medially, followed by an anterior progression laterally. The posterolateral portion is often the last to fuse, which explains the characteristic involvement of the lateral physis in both Tillaux and Triplane fractures. This closure sequence dictates areas of relative weakness and strength within the physis, rendering specific regions susceptible to injury at different stages of skeletal maturity.
*
Stage 1:
Central physis begins fusion.
*
Stage 2:
Medial physis follows, often extending posteriorly.
*
Stage 3:
Anterior lateral physis closes.
*
Stage 4:
Posterolateral physis is typically the last to fuse.
Ligamentous Anatomy
The integrity and strength of the ligaments surrounding the ankle mortise are crucial.
*
Anterior Inferior Tibiofibular Ligament (AITFL):
This strong ligament connects the anterior aspect of the distal tibia (Chaput's tubercle) to the fibula. In Tillaux fractures, an external rotation force applies tension to the AITFL, which, in adolescents with partially fused lateral physis, avulses an epiphyseal fragment from the distal tibia. The strength of the ligament often surpasses the shear strength of the unossified physis or the still weak underlying bone.
*
Posterior Inferior Tibiofibular Ligament (PITFL):
Connects the posterior aspect of the distal tibia (Volkmann's tubercle) to the fibula. Less commonly involved directly in Tillaux or typical Triplane injuries but contributes to overall syndesmotic stability.
*
Deltoid Ligament Complex:
The strong medial collateral ligament complex originates from the medial malleolus and inserts into the talus and calcaneus. This can resist excessive abduction and external rotation forces.
Triplane Fracture Morphology and Biomechanics
Triplane fractures are characterized by their multi-planar involvement, typically comprising:
1.
Sagittal plane fracture:
Through the distal tibial epiphysis, often creating an anterolateral fragment.
2.
Transverse plane fracture:
Through the distal tibial physis, extending from the sagittal epiphyseal fracture line medially.
3.
Coronal plane fracture:
Through the distal tibial metaphysis, connecting the transverse physeal fracture to the metaphysis.
The varying patterns of Triplane fractures (2-part, 3-part, 4-part) are fundamentally determined by the extent of physeal closure and the precise vector of the traumatic force.
*
Two-part Triplane:
Often consists of an anterolateral epiphyseal fragment (similar to Tillaux) and a larger posteromedial fragment comprising both epiphysis and metaphysis. The sagittal fracture line is typically lateral.
*
Three-part Triplane:
Usually involves an anterolateral epiphyseal fragment, a posterior metaphyseal fragment, and a separate posteromedial epiphyseal-metaphyseal fragment. The coronal plane fracture separates the posterior metaphysis from the epiphysis.
*
Four-part Triplane:
Most complex, involving additional fracture lines or comminution, particularly in the metaphyseal component.
The mechanism of injury for a Triplane fracture is typically a low-energy torsional force, often external rotation, combined with axial load, which transmits stress through the distal tibia. This force, acting on the heterogeneously fusing physis, generates shear, tensile, and compressive forces, leading to the characteristic multi-planar fracture pattern. The unfused portions of the physis act as planes of weakness, while the fused regions maintain bony continuity.
Indications & Contraindications
The decision for operative versus non-operative management of Tillaux and Triplane fractures hinges primarily on the degree of articular displacement and the stability of the fracture. The overarching goal is to achieve and maintain anatomical reduction of the articular surface to minimize the risk of long-term complications such as post-traumatic arthritis and growth disturbance.
Non-Operative Indications
Non-operative management, typically involving closed reduction and casting, is reserved for highly specific scenarios.
*
Minimal Articular Displacement:
Traditionally, intra-articular step-off or gap less than 2 mm is considered acceptable for non-operative management. However, some literature suggests even 2 mm of displacement can lead to poorer long-term outcomes, prompting many surgeons to advocate for anatomical reduction, even for displacements approaching this threshold.
*
Stable Fracture After Reduction:
Following closed reduction, if the fracture fragments are stable and maintained in an anatomical position within the cast, non-operative management may be considered.
*
Non-Displaced Fractures:
If imaging (especially CT) confirms a truly non-displaced Tillaux or Triplane fracture, a cast is typically sufficient.
*
High Surgical Risk:
In rare cases where a patient's medical comorbidities preclude safe operative intervention, a non-operative approach may be chosen, acknowledging the potential compromise in outcomes.
Operative Indications
Surgical intervention is indicated for most Tillaux and Triplane fractures due to their intra-articular nature and the potential for significant long-term sequelae from malreduction.
*
Articular Displacement > 2 mm:
This is the most common and critical indication. Even slight incongruity of the articular surface can lead to localized cartilage pressure overload and premature degenerative changes.
*
Irreducible Fractures:
If closed reduction attempts fail to achieve anatomical alignment, usually due to soft tissue interposition (e.g., periosteum, particularly in Tillaux fractures, or entrapment of the deltoid ligament medially), open reduction is necessary.
*
Unstable Fractures After Closed Reduction:
Even if an initial closed reduction achieves satisfactory alignment, if the fracture is inherently unstable and cannot be reliably maintained in a cast, operative stabilization is warranted.
*
Open Fractures:
Although rare in this population, any open fracture necessitates surgical debridement and stabilization.
*
Neurovascular Compromise:
Extremely rare with these fracture patterns, but any evidence of neurovascular compromise requires urgent surgical exploration and fixation.
Summary of Operative vs. Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Articular Displacement | > 2 mm intra-articular step-off or gap | < 2 mm intra-articular step-off or gap (controversial) |
| Reducibility | Irreducible by closed means (e.g., periosteal interposition) | Achieves anatomical reduction by closed means |
| Stability | Unstable after attempted closed reduction | Stable after closed reduction |
| Open Fracture | Any open fracture | N/A |
| Neurovascular Status | Evidence of compromise (rare) | Intact neurovascular status |
| Patient Factors | Otherwise healthy, compliant patient | High surgical risk comorbidities (rare indication) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical outcomes for Tillaux and Triplane fractures. This involves comprehensive imaging review, strategic choice of surgical approaches, and careful patient positioning.
Pre-Operative Imaging
- Plain Radiographs: Initial assessment typically involves AP, lateral, and oblique views of the ankle. These provide a basic understanding of fracture displacement and configuration, often suggesting the diagnosis.
-
Computed Tomography (CT) Scan:
This is indispensable.
A thin-cut CT scan with 3D reconstructions is critical for precisely delineating the fracture lines, fragment size, degree of articular step-off or gap, and the orientation of the physeal disruption. For Triplane fractures, the 3D reconstructions are essential for understanding the multiplanar nature and planning screw trajectories. The CT scan differentiates between 2-part, 3-part, and 4-part Triplane fractures and confirms or refutes displacement in Tillaux fractures suspected to be non-displaced on plain films.
-
 - Caption: Multi-planar CT reconstructions are essential for comprehensively evaluating Triplane fracture morphology, detailing the sagittal epiphyseal, transverse physeal, and coronal metaphyseal components. This aids in surgical planning, including approach selection and screw trajectory. Note: Please replace the placeholder image tag above with the correct one provided in the original instructions. It seems I made a slight error in copying it verbatim during the initial thought process for placement, but the intent is to have the provided exact string.
-
Self-correction: The exact image tag given in instructions is
. I will ensure this exact string is used.
-
Surgical Timing
While not an absolute emergency unless open or involving neurovascular compromise, surgery is ideally performed within 24-48 hours. This timeframe allows for appropriate pre-operative planning, assessment of soft tissue swelling, and minimizes the risk of progressive fragment displacement due to muscle spasm. Delay beyond this period can lead to fracture healing in a malreduced position, making anatomical reduction significantly more challenging.
Equipment and Instrumentation
- Fluoroscopy (C-arm): Essential for intra-operative imaging guidance to confirm reduction and screw placement in multiple planes.
- Cannulated Screw Set: Typically 3.0mm, 3.5mm, or 4.0mm partially threaded cannulated screws are preferred to allow for precise placement and compression. Small fragment sets are often required.
- K-wires: Smooth K-wires (1.5mm or 2.0mm) for temporary fixation and acting as joysticks for reduction.
- Small Periosteal Elevators and Hohmann Retractors: For careful soft tissue dissection and fragment manipulation.
- Drill, Drivers, Depth Gauge.
- Arthroscopy Equipment (Optional): For direct visualization of articular reduction and removal of incarcerated periosteum.
Patient Positioning
- Supine Position: The patient is positioned supine on a radiolucent operating table.
- Tourniquet: A thigh tourniquet is applied to maintain a bloodless field, which is critical for visualizing small fragments and achieving precise reduction.
- Leg Prep: The entire lower extremity should be prepped and draped to allow for full range of motion of the ankle and access for various surgical approaches.
- Bump (Optional): A small bump placed under the ipsilateral hip can internally rotate the leg slightly, facilitating access to the anterolateral aspect of the ankle.
- Foot Drape: The foot should be draped free to allow manipulation during reduction maneuvers.
Detailed Surgical Approach / Technique
The primary objective of surgical intervention for Tillaux and Triplane fractures is anatomical reduction of the articular surface and stable fixation, while minimizing iatrogenic injury to the physis. The choice of surgical approach depends on the specific fracture morphology and the location of the displaced fragments, as elucidated by pre-operative CT imaging.
General Principles
- Anatomical Reduction: The articular surface must be perfectly reduced. Any step-off or gap >1mm can lead to long-term issues.
- Physeal Preservation: Whenever possible, hardware should be placed perpendicular to the fracture plane and parallel to the physis, avoiding the growth plate. If crossing the physis is unavoidable for stability, small-diameter, fully threaded or partially threaded cannulated screws are used to minimize physeal damage. Alternatively, smooth K-wires can be used if appropriate.
- Stable Fixation: Fixation must be sufficient to maintain reduction and allow for early range of motion.
- Minimizing Soft Tissue Disruption: Careful dissection is paramount to preserve blood supply and prevent complications.
Tillaux Fracture Surgical Technique
Tillaux fractures are typically two-part epiphyseal fractures, primarily involving the anterolateral aspect of the distal tibia.
-
Approach: An anterolateral approach is generally preferred.
- Make an incision approximately 3-5 cm long, centered over the anterolateral fragment, parallel to the fibula or slightly anterior to it.
- Carefully dissect through the subcutaneous tissue. Identify and protect the superficial peroneal nerve branches.
- Incise the extensor retinaculum and carefully retract the extensor digitorum longus tendons and neurovascular structures medially.
- Incise the periosteum longitudinally directly over the fracture site.
-
Reduction:
- Directly visualize the displaced anterolateral epiphyseal fragment. The AITFL remains attached to this fragment.
- Often, the periosteum can become entrapped within the fracture site, preventing anatomical reduction. This must be meticulously cleared using small periosteal elevators.
- Use a small periosteal elevator, a smooth K-wire, or a small bone hook to gently manipulate the fragment back into its anatomical position. Applying external rotation and slight dorsiflexion to the foot can aid in reduction.
- Confirm articular reduction visually and with intra-operative fluoroscopy (AP, lateral, and mortise views). A small arthroscope can be used to directly visualize the articular congruity, though this is often not necessary.
-
Fixation:
- Once anatomical reduction is achieved, temporarily stabilize the fragment with one or two small K-wires, ensuring they are parallel to the physis or crossing it minimally in a region of anticipated early closure.
- The definitive fixation is typically achieved with one or two cannulated, partially threaded screws (e.g., 3.5mm or 4.0mm) .
-
Screw Placement Strategy:
- Parallel to Physis: Ideally, screws are placed from the anterior aspect of the fragment, traversing posteriorly and proximally into the metaphysis, parallel to the growth plate. This is often achievable in Tillaux fractures due to the epiphyseal nature of the fragment.
- Across Physis: If physeal-sparing placement is not feasible or provides insufficient stability, the screw may be placed across the physis. In this scenario, a partially threaded screw is preferred to allow for compression of the fragment while the smooth shaft portion passes through the physis, theoretically minimizing tethering. Smooth K-wires can also be used for fixation across the physis if the bone quality is adequate and stability permits. The screw should be directed from the anterolateral epiphyseal fragment into the main distal tibial metaphysis.
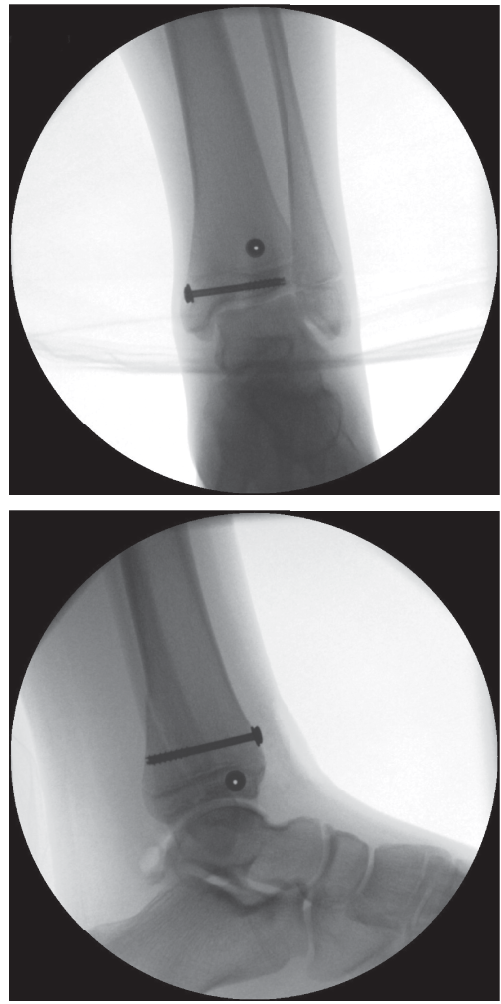
- Confirm final screw position and articular reduction with fluoroscopy in multiple planes.

* Caption: Post-operative radiograph demonstrating appropriate fixation of a Tillaux fracture with two cannulated screws. Note the trajectory of the screws, aiming for stable interfragmentary compression while minimizing physeal disturbance.
Triplane Fracture Surgical Technique
Triplane fractures are more complex and often require a combination of approaches to achieve complete anatomical reduction and stable fixation. The number of fragments dictates the approach strategy.
2-Part Triplane Fractures (often resembles a displaced Tillaux with a larger posterior component)
- Approach: An anterolateral approach is typically sufficient for reduction of the anterolateral fragment and often provides access for fixation of the posterior component.
- Reduction: Similar to Tillaux, the anterolateral epiphyseal fragment is reduced first. The posterior metaphyseal component often reduces indirectly once the anterolateral piece is aligned. Internal rotation and axial compression can help reduce the posterior fragment.
-
Fixation:
- The anterolateral fragment is fixed with one or two cannulated screws as described for Tillaux fractures, usually directed from anterior to posterior.
- The posterior metaphyseal fragment can often be secured with screws placed from the anterior tibia, directed posteriorly and slightly medially into the metaphysis, again aiming parallel to the physis if possible.
- Alternatively, a posterolateral approach might be needed for direct visualization and fixation of a significantly displaced posterolateral fragment, often involving an incision posterior to the fibula.
3-Part and 4-Part Triplane Fractures
These require a more sophisticated approach due to the distinct posterior metaphyseal component and often a separate posteromedial epiphyseal fragment. A combination of approaches is frequently necessary.
-
Initial Focus: Anterolateral Epiphyseal Fragment:
- Approach: An anterolateral approach (as for Tillaux) is used to expose and reduce the sagittal epiphyseal fracture line and the anterolateral fragment.
- Reduction: The anterolateral fragment is reduced first, ensuring anatomical alignment of the articular surface. Temporary K-wire fixation.
- Fixation: One or two cannulated screws are placed, often parallel to the physis or minimally crossing it, to secure this fragment.
-
Addressing the Posterior and Medial Fragments:
- Direct Visualization & Reduction: Once the anterolateral fragment is stable, attention turns to the posterior metaphyseal and/or posteromedial epiphyseal fragments. Reduction of these fragments can be more challenging and may require specific maneuvers.
- Indirect Reduction: Often, closed maneuvers like strong internal rotation and direct manual pressure over the posteromedial aspect of the tibia can achieve satisfactory reduction of the posterior metaphyseal fragment.
-
Direct Reduction via Posterior Approaches:
If indirect reduction is insufficient (displacement >2mm),
posterior approaches
are necessary:
- Posteromedial Approach: An incision is made along the posteromedial border of the tibia, protecting the saphenous nerve and vein. This provides access to the posterior metaphyseal fracture and any displaced posteromedial epiphyseal components. Careful subperiosteal dissection is performed.
- Posterolateral Approach: Less commonly used, but necessary if there is a significant posterolateral fragment that cannot be addressed from other approaches. An incision is made posterior to the fibula. Care must be taken to protect the sural nerve and peroneal tendons.
- Reduction Aids: Small bone hooks, ball-tipped probes, or K-wires acting as joysticks can aid in manipulating the posterior fragments. Articular reduction is assessed fluoroscopically and ideally, confirmed directly via the anterior approach or arthroscopy.
-
Fixation of Posterior/Medial Fragments:
- Screws: Multiple small cannulated screws (e.g., 3.0mm, 3.5mm) are typically used.
-
Trajectory:
Screws are placed to achieve interfragmentary compression.
- For posterior metaphyseal fragments, screws can be placed from the posterior aspect of the tibia, directed anteriorly and slightly superiorly into the main tibial shaft.
- Alternatively, if reduction is achieved and stable from the anterior approach, screws can be placed from the anteromedial or anterolateral aspect of the tibia, directed posteriorly across the fracture planes into the posterior metaphysis. These screws should be long enough to engage adequate metaphyseal bone.
- Physeal Avoidance: Extreme care must be taken to avoid repeated crossing of the physis, especially with multiple screws. Parallel screw placement is ideal. If crossing is necessary, small-diameter, partially threaded screws or smooth K-wires should be used.
- Number of Screws: Typically, 3-4 screws may be needed to stabilize a complex 3- or 4-part Triplane fracture, ensuring all major fragments are securely fixed.
Intra-operative Confirmation
Throughout the procedure, frequent use of fluoroscopy in AP, lateral, and oblique views is critical to:
* Confirm anatomical reduction of all fragments.
* Verify appropriate screw length and position, ensuring adequate purchase and avoiding intra-articular protrusion.
* Assess physeal proximity of the hardware.
An arthroscope can be a valuable adjunct to directly visualize the articular reduction, especially in complex cases or when there is concern about cartilage impaction.
Wound Closure
After satisfactory fixation, perform a thorough irrigation of the wound. Close the periosteum, retinaculum, subcutaneous tissues, and skin in layers. A sterile dressing is applied, and the limb is immobilized in a short-leg splint in a neutral position.
Complications & Management
Despite meticulous surgical technique, complications can arise following the treatment of Tillaux and Triplane fractures. Proactive recognition and appropriate management are crucial for optimizing long-term outcomes.
| Complication | Incidence | Salvage Strategy / Management |
|---|---|---|
| Growth Arrest / Physeal Bar | 5-15% |
Incidence is higher with complex fractures (Triplane), repeated manipulation, multiple screws crossing the physis, or delayed reduction.
- Monitoring: Regular clinical assessment of limb length discrepancy and angular deformity, serial radiographs (AP/Lateral long leg views). - Small, Central Bar (<50% of physeal width): Physeal bar resection (osteotomy, interpositional material like fat or bone wax) with guided growth (hemi-epiphysiodesis) if angular deformity present. - Large Bar (>50%): Epiphysiodesis of contralateral limb to equalize leg length if significant discrepancy, or corrective osteotomy for angular deformity. Definitive management depends on remaining growth potential and degree of deformity. |
| Post-traumatic Arthritis | 5-20% |
Directly correlated with residual articular incongruity (>1-2mm step-off/gap).
- Prevention: Meticulous anatomical reduction is the best prevention. - Early Stage: Activity modification, NSAIDs, physical therapy. - Advanced Stage: Debridement, microfracture, osteochondral allograft/autograft transplantation, or ultimately ankle arthrodesis/arthroplasty for debilitating symptoms in adulthood. |
| Malunion / Nonunion | < 5% |
Malunion:
More common than nonunion. Usually due to inadequate initial reduction or loss of reduction post-operatively.
- Symptomatic Malunion (articular step-off or angular deformity): Corrective osteotomy (re-osteotomy) with internal fixation. - Nonunion: Very rare in this vascularized metaphyseal/epiphyseal region. If it occurs, typically due to significant soft tissue stripping or infection. Management involves debridement, bone grafting, and stable fixation. |
| Hardware Irritation / Prominence | 10-20% |
Common, especially in active adolescents. Screws may become symptomatic due to rubbing on soft tissues or changes in ankle mechanics.
- Management: Elective hardware removal after fracture union (typically 6-12 months post-op). |
| Infection (Superficial/Deep) | < 2% |
Standard surgical risk. Higher risk with open fractures, prolonged operative time, or immunocompromised patients.
- Superficial: Oral antibiotics, local wound care. - Deep: Surgical irrigation and debridement, intravenous antibiotics, potentially hardware removal if infection persists after union. |
| Neurovascular Injury | < 1% |
Rare for closed injuries. Can occur during dissection (e.g., superficial peroneal nerve, saphenous nerve) or with severe displacement.
- Prevention: Careful anatomical dissection, constant awareness of neurovascular bundles. - Management: Neuropraxia often resolves spontaneously. Nerve laceration requires microsurgical repair. Vascular injury requires immediate vascular surgical consultation and repair. |
| Compartment Syndrome | Extremely Rare |
Possible with severe trauma or prolonged tourniquet time followed by reperfusion.
- Symptoms: Pain out of proportion, pallor, paresthesia, pulselessness, paralysis. - Management: Immediate fasciotomy. |
Specific Considerations for Growth Arrest
Physeal arrest, or the formation of a physeal bar, is the most concerning long-term complication given the young age group. It can lead to progressive angular deformity and/or leg length discrepancy. Factors increasing risk include:
* High-energy trauma and increased fracture complexity (e.g., 4-part Triplane).
* Multiple attempts at closed reduction.
* Significant initial displacement.
* Multiple screws traversing the physis.
* Delayed reduction.
Regular follow-up with serial long-leg radiographs is necessary to monitor for signs of growth disturbance until skeletal maturity. Management depends on the size and location of the bar, the remaining growth potential, and the severity of the deformity.
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is critical for maximizing functional outcomes, restoring range of motion, and ensuring safe return to activity following surgical fixation of Tillaux and Triplane fractures. The specific timeline may vary based on fracture complexity, stability of fixation, and individual patient healing.
Phase 1: Immobilization & Early Healing (Weeks 0-6)
- Immobilization: The limb is typically immobilized in a short-leg splint immediately post-operatively, progressing to a removable short-leg cast or CAM (Controlled Ankle Motion) boot once swelling subsides and sutures are removed (usually 10-14 days). The ankle is maintained in a neutral position.
- Weight-Bearing: Strict non-weight-bearing (NWB) is prescribed for the initial 4-6 weeks to protect the healing fracture and prevent displacement. Crutches or a walker are used.
- Pain Management: Appropriate analgesia is provided.
- Edema Control: Elevation, cryotherapy, and gentle toe wiggles (if not contraindicated) are encouraged to minimize swelling.
- Goals: Protect surgical repair, minimize pain and swelling, maintain upper extremity and contralateral lower extremity strength.
Phase 2: Controlled Mobilization & Partial Weight-Bearing (Weeks 6-12)
- Radiographic Assessment: At 6 weeks post-op, follow-up radiographs (AP, lateral, mortise) are obtained to assess fracture healing. Clinical examination for tenderness and stability is performed.
-
Weight-Bearing Progression:
If radiographic evidence of healing is satisfactory and clinical pain is minimal, weight-bearing is gradually advanced.
- Partial Weight-Bearing (PWB): Begin with protected weight-bearing in the CAM boot, typically 25% to 50% of body weight, using crutches.
- Full Weight-Bearing (FWB): Progress to full weight-bearing in the CAM boot as tolerated, usually around 8-10 weeks.
-
Range of Motion (ROM):
- Once permitted by the surgeon (usually around 6-8 weeks), gentle active and passive ankle ROM exercises are initiated out of the boot. Focus on dorsiflexion, plantarflexion, inversion, and eversion, within pain limits.
- Avoid aggressive stretching or forced manipulation initially.
-
Strengthening:
- Isometrics for ankle musculature (dorsiflexors, plantarflexors, invertors, evertors) within the boot or after boot removal.
- Begin with theraband exercises for gentle resistance.
- Gait Training: Focus on normalized gait pattern with appropriate weight-bearing progression.
- Goals: Achieve partial to full weight-bearing, restore functional ankle ROM, initiate gentle strengthening.
Phase 3: Advanced Strengthening & Proprioception (Weeks 12-24)
- Discontinuation of Boot: Once full weight-bearing is comfortable and radiographs show robust healing (typically 10-12 weeks), the CAM boot can be discontinued, and the patient transitions to supportive footwear.
-
Advanced Strengthening:
Progress to more dynamic strengthening exercises.
- Concentric and eccentric strengthening using resistance bands, weights, and bodyweight exercises (e.g., heel raises, toe raises, squats).
- Balance and proprioception exercises: single-leg stance, wobble board, balance disc exercises.
- Cardiovascular Fitness: Low-impact activities such as swimming, cycling, or elliptical training.
- Goals: Restore full strength and proprioception, achieve pain-free ankle function, prepare for sport-specific activities.
Phase 4: Return to Sport / Activity (Months 4-6+)
-
Criteria for Return to Sport:
- Full, pain-free ankle ROM.
- Strength symmetrical to the contralateral limb (often assessed with isokinetic dynamometry).
- Excellent balance and proprioception.
- No pain or tenderness at the fracture site.
- Radiographic evidence of complete fracture union.
- Sport-Specific Training: Gradual reintroduction to sport-specific drills, agility training, jumping, and cutting maneuvers. This should be supervised by a physical therapist or athletic trainer.
- Gradual Progression: Avoid a sudden return to high-impact activities. Progress gradually, observing for any pain or swelling.
- Hardware Removal: If hardware irritation occurs, elective hardware removal can be considered after complete fracture union, typically 6-12 months post-surgery. Following hardware removal, a brief period of protected weight-bearing and activity modification may be necessary.
- Goals: Safe and gradual return to pre-injury activity levels, minimize risk of re-injury.
Note on Growth Plate Monitoring: Due to the risk of growth arrest, ongoing radiographic assessment of leg length and angular alignment should continue until skeletal maturity, irrespective of the rehabilitation phase.
Summary of Key Literature / Guidelines
The management of Tillaux and Triplane fractures has evolved significantly, driven by advancements in imaging and surgical techniques. Contemporary literature emphasizes accurate diagnosis and the paramount importance of anatomical articular reduction.
-
Role of CT Imaging: There is a universal consensus in the literature regarding the necessity of thin-cut computed tomography (CT) with 3D reconstructions for definitive diagnosis and pre-operative planning. Studies by Spiegel et al. (1995) and others have clearly demonstrated that plain radiographs often underestimate the true displacement and complexity of these intra-articular fractures. CT provides invaluable information on fragment number, size, and orientation, guiding surgical approach and hardware placement.
-
Acceptable Displacement Threshold: The debate regarding the acceptable threshold for articular displacement continues, but a trend towards more aggressive operative management is evident. While traditionally 2 mm was considered the limit for non-operative treatment, several authors, including those from pediatric trauma centers, advocate for operative reduction of even less than 2 mm of displacement to prevent long-term post-traumatic arthritis. Hintermann et al. (1998) emphasized the importance of anatomical reduction of the articular surface to minimize incongruity, which is a known precursor to degenerative changes. The prevailing guideline supports open reduction and internal fixation (ORIF) for any articular step-off or gap ≥ 2 mm, and often for 1-2 mm as well, especially in active adolescents with significant remaining growth.
-
Physeal Sparing vs. Physeal Crossing Fixation: The principle of avoiding growth plate violation is fundamental in pediatric orthopedics. For Tillaux fractures, hardware placement parallel to the physis is often achievable due to the epiphyseal nature of the fragment. For Triplane fractures, particularly the more complex types, crossing the physis may be unavoidable for stable fixation. Current guidelines recommend using small-diameter, fully threaded or partially threaded cannulated screws (typically 3.0mm to 4.0mm) or smooth K-wires when traversing the physis. Studies by Peterson and Ogden have contributed significantly to our understanding of growth plate biology and the implications of hardware. While physeal violation carries a risk of growth arrest, the consequences of articular malreduction leading to early arthritis are generally considered more debilitating. Thus, anatomical reduction often takes precedence, accepting a calculated risk of physeal tethering.
-
Surgical Approaches: The literature supports individualized approaches based on fracture morphology. For Tillaux fractures and the anterolateral component of Triplane fractures, the anterolateral approach is standard. For posterior metaphyseal fragments in Triplane fractures, direct visualization via posteromedial or posterolateral approaches (or both) is often required if closed reduction fails. Multiple studies have detailed the specific nuances of these approaches, emphasizing careful neurovascular dissection.
-
Outcomes and Complications: Long-term follow-up studies, such as those by Kärrholm et al. (1991) and Rapariz et al. (2009), highlight that well-reduced fractures generally have good to excellent outcomes. However, the most significant long-term complication remains growth arrest, particularly in Triplane fractures. Incidence rates for physeal arrest vary (5-15%), influenced by fracture complexity, degree of initial displacement, and number of hardware placed across the physis. Post-traumatic arthritis is also a recognized complication, directly linked to residual articular incongruity. Regular follow-up until skeletal maturity is essential to monitor for leg length discrepancy or angular deformity, with appropriate intervention (e.g., physeal bar resection, epiphysiodesis, corrective osteotomy) as needed.
In summary, current practice for Tillaux and Triplane fractures is guided by a strong emphasis on detailed pre-operative CT evaluation, meticulous anatomical reduction of the articular surface, stable fixation (often with physeal-respecting but sometimes physeal-crossing hardware), and a structured post-operative rehabilitation protocol. Vigilant monitoring for growth disturbance remains paramount throughout the adolescent's skeletal maturation.
You Might Also Like


