Mastering the Treatment of Forearm Compartment Syndrome
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Mastering the Treatment of Forearm Compartment Syndrome. The treatment of forearm compartment syndrome involves prompt surgical decompression, or fasciotomy. This procedure divides the tight fascia constraining the affected muscle compartments—typically the anterior/flexor and posterior/extensor—to relieve pressure. Decompressing all affected areas restores blood flow, preventing permanent muscle necrosis, nerve damage, and severe complications like Volkmann ischemic contracture or gangrene.
Mastering the Treatment of Forearm Compartment Syndrome
Introduction & Epidemiology
Acute forearm compartment syndrome is a surgical emergency requiring immediate recognition and intervention to prevent irreversible ischemic injury and devastating functional deficits. The forearm is anatomically complex, comprising multiple distinct osseo-fascial compartments, each containing specific muscle groups, nerves, and vascular structures. Traumatic incidents, particularly high-energy fractures (e.g., forearm diaphyseal fractures, supracondylar humerus fractures in children), severe soft tissue crush injuries, burns, vascular compromise (e.g., reperfusion injury, arterial occlusion), and even iatrogenic causes (e.g., tight casts, prolonged tourniquet use) can lead to hemorrhage and edema within these confined spaces.
The resultant increase in interstitial pressure within these compartments compromises microvascular perfusion. As hydrostatic pressure surpasses capillary perfusion pressure, venous outflow is initially impeded. This further exacerbates edema and increases pressure in a vicious cycle. If untreated, arterial inflow eventually becomes compromised, leading to profound muscle ischemia and necrosis, as well as neuropraxia or neurotmesis of the contained nerves. The clinical sequelae, collectively known as Volkmann ischemic contracture, can range from mild functional impairment to a severely contracted, insensate, and non-functional limb. While relatively rare, with an incidence estimated at 0.7 to 2.8% in all extremity trauma, the consequences of missed diagnosis or delayed treatment are catastrophic, underscoring the imperative for timely and accurate management. Compartment syndrome can occur even in the absence of a fracture, as seen with crushing injuries or reperfusion injury, highlighting the need for a high index of suspicion based on clinical signs rather than radiographic findings alone.
Surgical Anatomy & Biomechanics
A thorough understanding of forearm anatomy is paramount for safe and effective fasciotomy. The forearm is typically divided into four primary osseo-fascial compartments, although some classifications may describe five:
- Superficial Volar (Flexor) Compartment: Contains pronator teres, flexor carpi radialis (FCR), palmaris longus, flexor carpi ulnaris (FCU), and flexor digitorum superficialis (FDS). The median nerve and ulnar artery course deep to this compartment, but their branches may be superficial. The fascia overlying this compartment is robust.
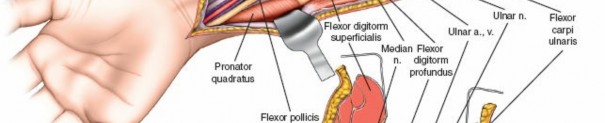
- Deep Volar (Flexor) Compartment: Deep to the FDS, this compartment houses flexor digitorum profundus (FDP), flexor pollicis longus (FPL), and pronator quadratus (PQ). The anterior interosseous nerve (AIN), a branch of the median nerve, and the anterior interosseous artery (AIA), a branch of the ulnar artery, are key structures here. The median nerve, deep to the FDS, is a critical structure that requires protection. The ulnar nerve and artery run along the ulnar border.
- Dorsal (Extensor) Compartment: Contains the extensor carpi ulnaris (ECU), extensor digiti minimi (EDM), extensor digitorum communis (EDC), and supinator. The posterior interosseous nerve (PIN), a branch of the radial nerve, courses through the supinator and then becomes the primary innervation for the dorsal compartment musculature.
- Lateral (Mobile Wad) Compartment: Also known as the mobile wad of Henry, this compartment contains the brachioradialis (BR), extensor carpi radialis longus (ECRL), and extensor carpi radialis brevis (ECRB). The superficial radial nerve runs deep to the brachioradialis in its distal third.
The investing fascia surrounding these compartments is relatively inelastic. This inelasticity, combined with the presence of multiple muscles and neurovascular structures, predisposes the forearm to compartment syndrome when intrafascial pressures rise. The biomechanical consequence of increased pressure is a cascade of events:
* Venous collapse leading to increased capillary pressure.
* Transudation of fluid into the interstitial space, further increasing compartmental pressure.
* Reduced arteriolar flow, causing muscle ischemia.
* Cellular damage and release of inflammatory mediators, increasing capillary permeability and further exacerbating edema.
* Irreversible myoneural necrosis within 4-8 hours if pressure is not relieved.
Indications & Contraindications
The decision for forearm fasciotomy is primarily guided by clinical assessment, often supported by objective compartment pressure measurements. Time is of the essence; the adage "the sun should not set or rise on a suspected compartment syndrome" underscores the urgency.
Indications for Forearm Fasciotomy:
- Clinical Suspicion: The cardinal symptom is pain disproportionate to the injury, unrelieved by analgesia, and exacerbated by passive stretching of the involved muscles. Other signs include paresthesias, tenseness of the compartment, and motor weakness. Importantly, normal distal pulses and capillary refill can be present in early to mid-stage compartment syndrome, and their presence should never delay intervention.
-
Objective Pressure Measurements:
While clinical findings remain paramount, direct intracompartmental pressure (ICP) measurement can aid in diagnosis, particularly in obtunded, uncooperative, or pediatric patients.
- Absolute Indication: ICP > 30 mmHg or a delta pressure (diastolic blood pressure - ICP) ≤ 20-30 mmHg. A delta pressure of 30 mmHg is often used as a threshold for fasciotomy.
- Relative Indication: In cases of equivocal clinical findings, serial ICP measurements can monitor trends.
- High-Risk Injuries: Prophylactic fasciotomy may be considered in specific high-risk scenarios, such as prolonged ischemia/reperfusion injury (e.g., embolectomy for acute arterial occlusion), severe crush injuries, or extensive forearm burns, even in the absence of definitive compartment syndrome, due to the high likelihood of its development.
- Chronic Exertional Compartment Syndrome: While rare in the forearm, this condition typically presents with exercise-induced pain and can be diagnosed by pre- and post-exercise compartment pressure measurements. Fasciotomy is indicated if conservative measures fail.
Contraindications:
- Established Irreversible Necrosis (Late Presentation): If significant time has passed (typically >12-24 hours) and clinical signs suggest irreversible muscle necrosis (e.g., fixed contracture, absent motor function, woody compartments), fasciotomy may increase the risk of infection and wound complications without functional benefit. In such cases, debridement and delayed reconstruction or amputation may be more appropriate.
- Resolved Compartment Syndrome: Documented resolution of symptoms and normalization of compartment pressures without surgical intervention.
| Indication Type | Criteria / Description |
|---|---|
| Operative | |
| Acute Confirmed | Unrelenting pain disproportionate to injury, pain on passive stretch, paresthesias, tense compartment(s). Elevated intracompartmental pressure (ICP) > 30 mmHg or Delta P (DBP - ICP) ≤ 20-30 mmHg. |
| Acute Suspected | Equivocal clinical signs in obtunded/unreliable patient, high-risk injury (e.g., prolonged ischemia, crush injury) with rising ICP, even if below absolute threshold, or in a rapid upward trend. Prophylactic fasciotomy in anticipated reperfusion injury. |
| Chronic Exertional | Persistent, debilitating, exercise-induced forearm pain refractory to conservative management, confirmed by pre- and post-exercise ICP measurements showing elevated pressures at symptom onset or post-exercise. |
| Non-Operative | |
| Equivocal/Early | Mild symptoms, normal or slightly elevated ICP, and a low suspicion of progression. Requires strict observation, serial clinical assessments, and serial ICP measurements. Cast/dressing removal, limb elevation to heart level. |
| Resolved Spontaneously | Symptoms resolve, and ICP normalizes without intervention. Requires continued close monitoring. |
| Irreversible Necrosis | Very late presentation (>12-24 hours) with signs of established muscle necrosis (e.g., fixed contracture, skin changes, absent pulses, woody compartments). Fasciotomy may offer no benefit and increase risk of infection. Often managed with serial debridement. |
Pre-Operative Planning & Patient Positioning
Once the decision for forearm fasciotomy is made, preparation should be swift.
- Patient Resuscitation: Ensure hemodynamic stability. Address any concurrent life-threatening injuries.
- Informed Consent: Discuss the procedure, potential complications (nerve injury, infection, stiffness, cosmetic deformity, need for skin grafting), and the possibility of Volkmann's contracture if not performed.
- Anesthesia: General anesthesia is typically preferred. A regional block (e.g., interscalene) can provide excellent post-operative analgesia but should be administered cautiously to avoid masking clinical signs of persistent compartment syndrome.
-
Operating Room Setup:
- Tourniquet: A pneumatic tourniquet should be applied to the arm. While the limb is exsanguinated prior to inflation, the fasciotomy itself should always be performed without the tourniquet inflated to assess muscle viability and control bleeding. The tourniquet serves as an emergency backup.
- Arm Table: A sterile hand table or arm board is essential for optimal exposure.
- Lighting and Magnification: Adequate lighting and loupe magnification are beneficial for precise dissection and nerve identification.
- Patient Positioning: The patient is typically supine with the affected arm abducted on a hand table. This allows for full access to both volar and dorsal aspects of the forearm. The elbow should be slightly flexed. The entire arm, including the shoulder and hand, should be prepped and draped to allow full range of motion if needed during the procedure, and for access to potential skin graft donor sites.
Detailed Surgical Approach / Technique
The goal of forearm fasciotomy is complete decompression of all affected compartments. This typically requires both volar and dorsal approaches. In cases of isolated compartment involvement, a single approach may suffice, but this is less common for acute traumatic compartment syndrome involving the entire forearm. The principle is meticulous, longitudinal fasciotomy to relieve pressure without causing further neurovascular injury.
I. Volar (Anterior) Approach
The volar approach addresses the superficial and deep volar compartments, which are most commonly involved and contain the majority of the forearm musculature and critical neurovascular structures.
-
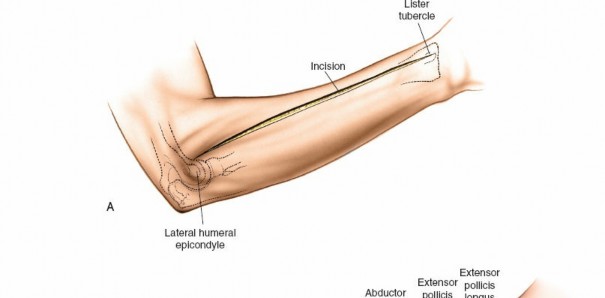
Incision: A curvilinear incision is made from the medial epicondyle, across the antecubital fossa, extending obliquely to the mid-volar aspect of the forearm, and then longitudinally down to the wrist crease, potentially extending into the palm to release the carpal tunnel. The incision should be generous, allowing for wide exposure.
-
Key points:
The proximal portion of the incision should curve gently to avoid crossing the elbow flexion crease at a right angle, which could lead to contracture. Distally, it should avoid cutting directly over the median nerve at the wrist.

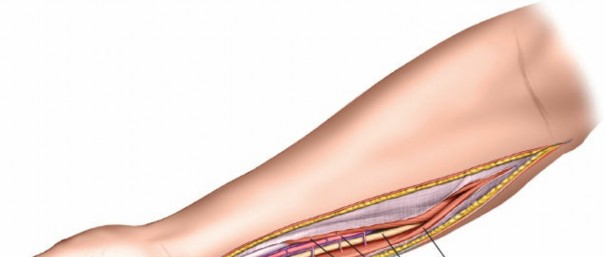
This image shows the standard curvilinear incision for the volar approach, extending proximally from the medial epicondyle, gently crossing the antecubital fossa, and proceeding distally across the mid-forearm to the wrist.
-
Key points:
The proximal portion of the incision should curve gently to avoid crossing the elbow flexion crease at a right angle, which could lead to contracture. Distally, it should avoid cutting directly over the median nerve at the wrist.
-
Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue. The superficial fascia is then identified.
This image depicts the initial incision through the skin and subcutaneous tissue, exposing the underlying superficial fascia. -
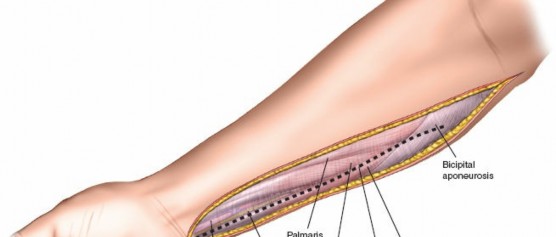
Release of Superficial Volar Compartment: The superficial investing fascia of the forearm is carefully incised longitudinally throughout the length of the exposure. This releases the pronator teres, FCR, palmaris longus, FCU, and FDS.
- Proximally: Identify and protect the median nerve as it passes between the two heads of the pronator teres. The superficial head of the pronator teres can be released to facilitate access to the deep compartment. The Lacertus Fibrosus (bicipital aponeurosis) should also be released as it can be a source of compression.
-
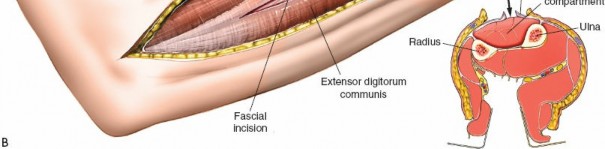
Mid-forearm:
The FDS muscle bellies are prominent. Ensure the fasciotomy extends across the full width of the compartment.

Here, the superficial volar fascia has been incised, demonstrating decompression of the superficial flexor muscles. Note the muscle bulging as pressure is released.
-
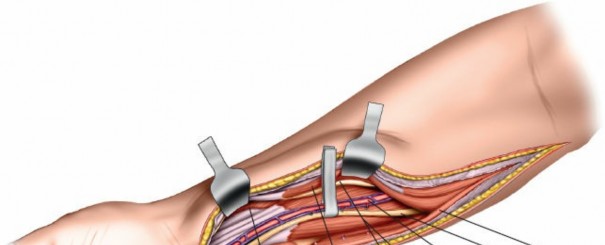
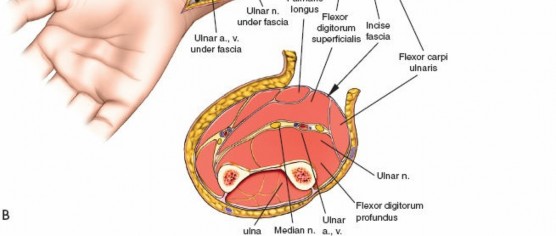
Exposure and Release of Deep Volar Compartment: This is the most critical and potentially challenging step. The median nerve and ulnar artery lie deep to the superficial flexor muscles.
- Median Nerve Protection: Retract the FDS radially. The median nerve typically lies beneath the FDS. It must be carefully identified and protected.
- Ulnar Nerve and Artery Protection: The ulnar nerve and artery run along the ulnar border, deep to the FCU. They are usually not directly in the field of the primary fasciotomy, but their fascial envelopes should also be released.
-
Accessing the Deep Compartment:
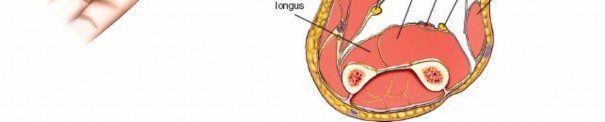
Separate the FDS radially from the FCU. Retract the FDS radially and the FCU ulnarly. The deep volar compartment, containing FDP, FPL, and PQ, is now accessible. The fascia overlying the FDP and FPL must be meticulously incised longitudinally. This deep release is crucial for adequate decompression.
This image illustrates the deeper dissection. The superficial flexor muscles (FDS) are retracted, exposing the median nerve and the underlying deep volar compartment. Note the care taken to protect the median nerve.
The median nerve and ulnar artery/nerve must be completely unroofed to ensure adequate decompression. This often requires releasing the entire carpal tunnel proximally to ensure distal decompression of the median nerve.
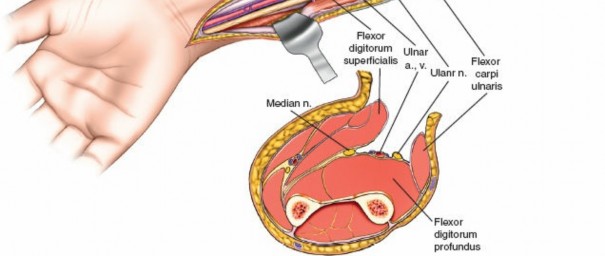
This detailed view highlights the median nerve (retracted by the yellow vessel loop) and the extensive release required, extending distally to encompass the carpal tunnel, ensuring complete decompression.Ensure that the deep fascia separating the FDS from the FDP and FPL is completely released. The anterior interosseous nerve and artery lie on the interosseous membrane and should also be decompressed by releasing the fascia overlying the deep flexors.
Further meticulous dissection showing the complete release of the deep volar compartment, with all muscle bellies visibly decompressing. Neurovascular structures are clearly identified and protected.
II. Dorsal (Posterior) Approach
The dorsal approach addresses the dorsal and mobile wad compartments.
-
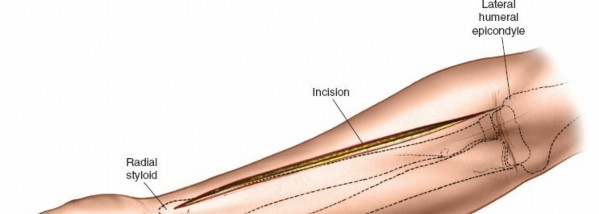
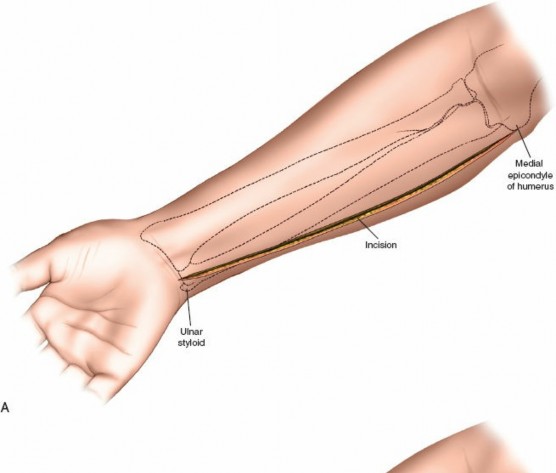
Incision: A separate straight longitudinal incision is made over the dorsal aspect of the forearm, centered approximately between the ulna and radius, extending from just distal to the lateral epicondyle to the wrist.
This image shows the dorsal longitudinal incision, made directly over the extensor compartment, providing access for decompression. -
Skin and Subcutaneous Tissue: Incise the skin and subcutaneous tissue.
-
Release of Dorsal Compartment: Identify the investing fascia over the extensor muscle group (ECU, EDM, EDC, supinator). This fascia is incised longitudinally throughout the length of the incision. Ensure full decompression of all muscle bellies.
-
Proximal Consideration:
The supinator tunnel, through which the posterior interosseous nerve (PIN) passes, should be carefully inspected and released if necessary, though it is less commonly a primary compression site in acute compartment syndrome.
The dorsal fascia is incised here, allowing the extensor muscles to expand. The extensor digitorum communis and other dorsal muscles are visible.
-
Proximal Consideration:
The supinator tunnel, through which the posterior interosseous nerve (PIN) passes, should be carefully inspected and released if necessary, though it is less commonly a primary compression site in acute compartment syndrome.
-
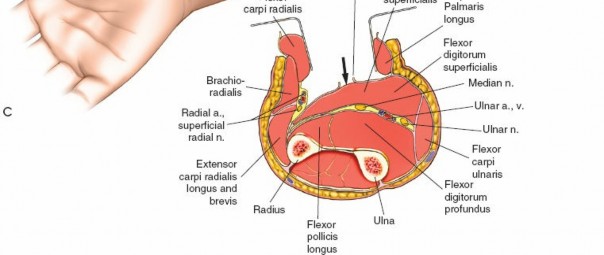
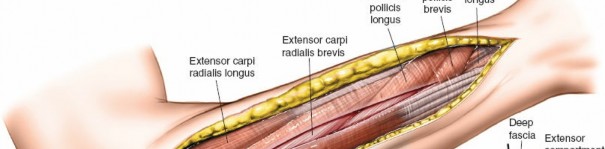
Release of Mobile Wad (Lateral) Compartment: This compartment contains the brachioradialis, ECRL, and ECRB. The fascia overlying these muscles should also be released through the dorsal incision, often by extending the fascial release more radially. The superficial radial nerve runs deep to the brachioradialis in its distal third; care must be taken to avoid injury during distal extension of the fascial release.
This image illustrates the release of the mobile wad, specifically showing the decompression of the brachioradialis. The full extent of the fascial release should be visualized.
III. Wound Management
After complete fasciotomy, the incisions are left open. The wounds should be thoroughly irrigated, and any visibly necrotic or non-viable muscle should be sharply debrided. The tourniquet should be deflated to confirm hemostasis. The limb should be dressed with a moist, non-adherent dressing, typically incorporating a bulky soft dressing.
Post-fasciotomy, showing the wounds left open. The muscles are visibly decompressed and bulging slightly through the incision. Necrotic tissue, if present, would be debrided at this stage.
A second-look procedure within 24-48 hours is standard practice to assess muscle viability, perform further debridement if necessary, and potentially attempt delayed primary closure.
A post-fasciotomy dressing, indicating that the wounds are kept open and protected, awaiting a second look or closure. Note the presence of the open wound indicating effective decompression.
If delayed primary closure is not feasible due to persistent edema or skin tension, various closure techniques can be employed:
*
V-Y plasty:
For small gaps, using local tissue.
*
Skin Grafting:
Split-thickness skin grafts (STSG) are commonly used for larger defects.
This image depicts the wound approximately 5 days post-fasciotomy, showing a reduction in edema and granulation tissue formation, making it amenable to closure.

An example of successful delayed wound closure, potentially using skin grafting or secondary intention if primary closure was not possible. This demonstrates the final appearance of a closed fasciotomy wound.
Vacuum-assisted closure (VAC) devices can be highly beneficial in reducing edema, promoting granulation tissue formation, and facilitating eventual wound closure.
Complications & Management
Despite prompt and technically proficient fasciotomy, several complications can arise, ranging from minor to devastating. Understanding these and having a management strategy is crucial.
| Complication | Incidence / Description | Salvage / Management Strategies |
|---|---|---|
| Persistent Compartment Syndrome | Rare if adequate fasciotomy performed, but can occur due to incomplete release of all involved compartments, especially the deep volar or mobile wad. Signs include ongoing pain, paresthesias, and muscle tenseness despite initial fasciotomy. | Immediate re-exploration: Re-open the fasciotomy wounds. Systematically check each compartment, ensuring complete release of all fascial layers. Re-evaluate clinical signs and consider repeat compartment pressure measurements in OR. Identify and release any remaining constricting bands or unreleased fascia. |
| Infection | Variable (5-20%) depending on wound contamination, patient factors (e.g., open fracture), and duration of open wound. Can lead to osteomyelitis or systemic sepsis. | Aggressive wound care: Serial debridement of necrotic tissue, thorough irrigation. Broad-spectrum antibiotics: Initiated empirically, then tailored to culture results. Wound closure: Delayed closure or skin grafting once infection is controlled. Negative Pressure Wound Therapy (NPWT): May aid in managing contaminated wounds and promoting granulation. Osteomyelitis: Requires prolonged antibiotic therapy, potentially surgical debridement of bone, and reconstruction. |
| Nerve Injury (Iatrogenic) | Rare (<5%) with careful technique, but potential for injury to median, ulnar, radial, or their branches (AIN, PIN, superficial radial nerve). Can occur during initial incision, fascial release, or retraction. | Prevention: Meticulous surgical technique, clear anatomical understanding, loupe magnification. Intraoperative identification: If nerve transection suspected, primary repair may be attempted. Postoperative: Early nerve conduction studies and EMG if neurological deficit persists. Rehabilitation: Nerve gliding exercises. Secondary intervention: Nerve grafting or transfer for complete transections if primary repair fails or is not feasible. Neurolysis for entrapment. |
| Stiffness / Contracture | Common (20-40%) affecting wrist, finger, or elbow motion due to scar formation, muscle fibrosis, or untreated Volkmann's contracture. | Early and aggressive rehabilitation: Hand therapy, passive and active range of motion exercises, splinting. Scar management: Massage, silicone sheeting, stretching. Secondary surgical procedures: Tenolysis, capsulotomy, arthrolysis, contracture release (e.g., Z-plasty for skin, muscle slide, or free functional muscle transfer for Volkmann's contracture). |
| Volkmann Ischemic Contracture | The most devastating long-term complication if compartment syndrome is missed or inadequately treated. Ranges from mild (affecting one or two muscles) to severe (involving all forearm muscles, nerves, and vessels, leading to a useless, insensate hand). | Prevention: Timely fasciotomy. Early recognition: Assessment for persistent deficits post-fasciotomy. Mild/Moderate: Aggressive physical therapy, stretching, dynamic splinting. Severe: Secondary reconstructive procedures – muscle slide, tendon transfers, free functional muscle transfer, neurolysis/nerve grafting. Amputation in extreme, non-functional cases. |
| Cosmetic Deformity / Scarring | Inevitable, given the large incisions required. Can be prominent, hypertrophic, or keloidal. | Wound closure: Judicious use of skin grafting to minimize tension. Scar management: Massage, silicone gel sheets, pressure garments, corticosteroid injections for hypertrophic scars/keloids. Secondary procedures: Scar revision, Z-plasties to break up linear contractures. |
| Skin Graft Complications | (If performed) Graft failure, infection, donor site morbidity (pain, scarring). | Careful surgical technique: Ensure good graft take. Post-operative care: Immobilization, wound dressing changes, infection prevention. Donor site care: Proper dressing, pain management. |
| Chronic Pain / Neuropathic Pain | Can result from nerve injury, persistent muscle ischemia, or scar tissue impingement. | Multimodal pain management: Pharmacological (neuropathic agents), physical therapy, nerve blocks, psychological support. Surgical neurolysis: If clear evidence of nerve entrapment by scar tissue. |
Post-Operative Rehabilitation Protocols
Post-fasciotomy rehabilitation is a critical component of treatment, aiming to maximize functional recovery and mitigate long-term complications. The protocol varies based on the severity of the initial injury, the extent of muscle damage, and the method of wound closure.
Immediate Post-Operative Phase (Days 0-7):
- Wound Care: Meticulous wound care is paramount. Initial dressings should be moist and non-adherent, followed by serial dressing changes, typically daily. Negative pressure wound therapy (NPWT) may be utilized to reduce edema and promote wound bed preparation if wounds are large.
- Elevation: The limb should be elevated above the level of the heart to reduce edema.
- Second-Look Surgery: Usually performed within 24-48 hours. At this stage, muscle viability is assessed, non-viable tissue is debrided, and decisions regarding wound closure (delayed primary, STSG, or further delayed closure) are made.
- Early Motion: As soon as feasible and medically appropriate, gentle, protected active and passive range of motion (ROM) exercises for the hand, wrist, and elbow should commence. The goal is to prevent joint stiffness and muscle contracture without compromising wound integrity. This often begins within the first 24-48 hours, especially after a second look.
- Pain Management: Adequate analgesia is essential to facilitate early motion and patient cooperation.
Intermediate Phase (Weeks 1-6, Post-Closure):
- Wound Healing: Continue meticulous wound care until closure is achieved and stable. If skin grafting was performed, protect the graft.
- Edema Control: Continue elevation, consider light compression garments or wraps if tolerated and indicated.
- Active and Passive ROM: Progressively increase the intensity and duration of ROM exercises for all joints of the wrist, hand, and elbow. This includes specific exercises for finger flexors and extensors.
- Gentle Strengthening: Once wounds are stable and pain allows, begin isometric exercises and very light resistance, gradually progressing to isotonic exercises. Focus on restoring balance between flexor and extensor groups.
- Scar Management: Initiate scar massage, silicone sheeting, and gentle stretching to prevent hypertrophic scarring and contractures once wounds are healed.
- Splinting: Dynamic or static progressive splinting may be indicated to address specific joint stiffness or developing contractures, particularly for wrist flexion or extension, and finger flexion.
Advanced Phase (Weeks 6+, Return to Function):
- Progressive Strengthening: Advance resistance exercises, incorporating functional movements. Focus on grip strength, pinch strength, and forearm pronation/supination.
- Endurance Training: Incorporate repetitive tasks to improve muscle endurance.
- Proprioception and Coordination: Exercises to improve fine motor skills and hand-eye coordination.
- Return to Activity: Gradually introduce activity-specific training for work, sports, or hobbies, ensuring the limb can tolerate the demands without exacerbation of symptoms.
- Long-term Monitoring: Continued surveillance for late-onset contractures, neuropathic pain, or functional deficits. Referrals to pain management, neurology, or hand surgery may be necessary for recalcitrant issues.
- Psychological Support: A significant injury and lengthy recovery can impact mental health. Provide support and resources as needed.
Summary of Key Literature / Guidelines
The management of forearm compartment syndrome is guided by established principles, though nuances continue to be refined by ongoing research.
-
Diagnostic Criteria:
- Clinical Suspicion: Remains the cornerstone. The 5 P's (Pain, Pallor, Paresthesia, Paralysis, Pulselessness) are classic but often late signs. Pain out of proportion and pain on passive stretch are the most reliable early indicators.
- Intracompartmental Pressure (ICP) Measurement: While not a substitute for clinical judgment, ICP is invaluable, especially in obtunded or non-communicative patients. Most literature supports a threshold of ICP > 30 mmHg or a Delta P (DBP - ICP) ≤ 20-30 mmHg as an indication for fasciotomy. McQueen and Court-Brown (1996) famously advocated for the Delta P criterion, showing it to be a more reliable indicator than absolute ICP, particularly in hypotensive patients.
- Timing: The "golden period" for fasciotomy is generally considered to be within 4-6 hours of ischemia onset, with irreversible damage rapidly accumulating thereafter. Delayed fasciotomy beyond 8-12 hours significantly increases the risk of irreversible damage and infection.
-
Surgical Technique:
- Comprehensive Decompression: Consensus strongly supports complete decompression of all involved compartments. For the forearm, this almost universally necessitates both volar and dorsal approaches. The dual incision approach is preferred over a single incision to minimize iatrogenic neurovascular injury and ensure full release.
- Volar Approach: The curvilinear incision (Henry approach modification) allows for broad access. Key steps include releasing the superficial volar fascia, identifying and protecting the median nerve, and meticulously releasing the deep volar compartment fascia (FDP, FPL). Complete carpal tunnel release is often a critical distal extension of the volar fasciotomy.
- Dorsal Approach: A straight longitudinal incision is standard for dorsal and mobile wad compartment release. Care must be taken to ensure the full length of the extensor fascia and mobile wad fascia is released.
- Wound Management: Leaving wounds open for 24-48 hours with a second look is standard. Delayed primary closure is ideal, but split-thickness skin grafting is a common and accepted method for definitive closure of extensive defects.
-
Prophylactic Fasciotomy:
- Considered in high-risk scenarios such as prolonged ischemia (>6 hours), severe crush injuries, or anticipated reperfusion injury (e.g., following revascularization of an acutely ischemic limb). This remains a clinical judgment call based on individual patient factors and injury characteristics.
-
Outcomes and Prognosis:
- The primary determinant of outcome is the time to fasciotomy . Delayed diagnosis and treatment lead to higher rates of Volkmann ischemic contracture, nerve palsy, and functional deficits.
- Even with timely intervention, patients may experience residual weakness, sensory deficits, and stiffness. Aggressive rehabilitation is paramount for maximizing functional recovery.
- Studies (e.g., Gelberman et al., 1981; Matsen et al., 1980) have highlighted the devastating functional loss associated with missed or delayed diagnosis, emphasizing the importance of a high index of suspicion.
-
Recent Advances and Controversies:
- Continuous ICP Monitoring: While intermittent measurements are common, continuous monitoring devices offer real-time data, which may be beneficial in complex cases or unreliable patients. However, placement technique and calibration remain critical.
- Imaging: While typically not diagnostic for acute compartment syndrome, advanced imaging (e.g., MRI) can delineate muscle edema and necrosis in subacute or chronic cases, aiding in planning reconstructive surgery for Volkmann's contracture.
- Fasciotomy vs. Percutaneous Release: Percutaneous fasciotomy is generally contraindicated for acute traumatic compartment syndrome in the forearm due to the risk of incomplete release and iatrogenic neurovascular injury. It may have a limited role in very select cases of chronic exertional compartment syndrome, but open techniques offer superior visualization and completeness of release.
In conclusion, mastering the treatment of forearm compartment syndrome demands a profound understanding of surgical anatomy, a high index of clinical suspicion, rapid diagnostic acumen, decisive operative intervention, and comprehensive post-operative management. Adherence to established surgical principles and a multidisciplinary rehabilitation approach are essential to optimize outcomes and mitigate the devastating long-term consequences of this limb-threatening condition.
Clinical & Radiographic Imaging