Mastering Nonoperative Care for Proximal Humeral Fractures Greater

Key Takeaway
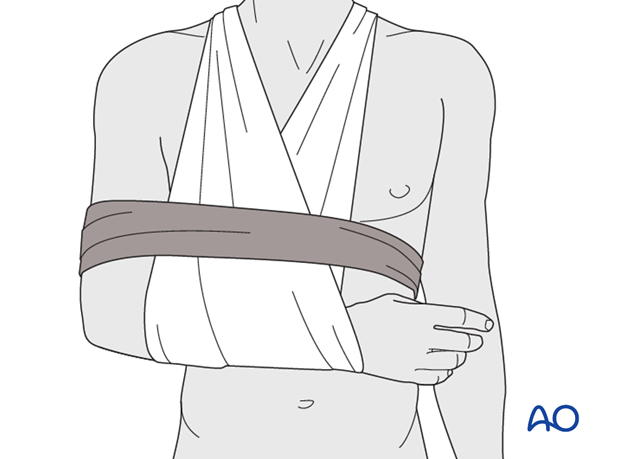
For anyone wondering about Mastering Nonoperative Care for Proximal Humeral Fractures Greater, Nonoperative treatment is primarily used for proximal humeral fractures, especially nondisplaced greater tuberosity types. Most heal without surgery, restoring satisfactory function. Management involves initial immobilization (2-3 weeks using a sling and swath), progressing to passive range of motion, and finally resistance exercises around 6 weeks to regain strength and function.
Introduction and Epidemiology
Proximal humeral fractures represent a significant orthopedic burden, accounting for approximately 5% of all fractures. Their incidence peaks in the elderly population, particularly postmenopausal women, largely attributable to underlying osteoporosis and low-energy falls. However, high-energy trauma can affect younger individuals, resulting in more complex fracture patterns. The management spectrum for these injuries ranges from entirely nonoperative approaches to various surgical interventions, dictated by a complex interplay of fracture morphology, patient demographics, functional demands, bone quality, and surgeon experience.
The focus of this discourse is to provide an exhaustive review of nonoperative management strategies for proximal humeral fractures, with a particular emphasis on those involving the greater tuberosity and other patterns amenable to conservative care. While the vast majority of proximal humerus fractures can heal without surgical intervention, optimizing nonoperative treatment requires a thorough understanding of fracture biology, biomechanics, and rehabilitation principles. The goal of nonoperative treatment is to achieve satisfactory functional outcomes while minimizing complications, often rivaling or even surpassing the results of operative fixation for appropriately selected cases. This review will delve into the nuances of patient selection, detailed nonoperative protocols, and evidence-based guidelines, contextualizing them within a broader discussion that acknowledges the role of surgical management where nonoperative approaches are unsuitable or fail.
Surgical Anatomy and Biomechanics
A comprehensive understanding of the proximal humeral anatomy and its intricate biomechanical relationships is paramount for effective management, irrespective of the chosen treatment modality.
Proximal Humeral Bony Anatomy
The proximal humerus comprises several distinct anatomical landmarks critical for shoulder function and fracture classification. These include the humeral head, anatomical neck, surgical neck, greater tuberosity, lesser tuberosity, and the bicipital groove. The greater tuberosity is particularly significant as it serves as the insertion point for the supraspinatus, infraspinatus, and teres minor tendons—collectively, the posterosuperior rotator cuff. Fractures involving the greater tuberosity often result from avulsion forces from these powerful muscles, or direct impact. The lesser tuberosity, conversely, serves as the insertion for the subscapularis. The surgical neck, located distal to the tuberosities and anatomical neck, is the most common site for fracture, acting as a transition zone between the metaphyseal bone of the humeral head and the diaphyseal shaft. Integrity of the medial calcar and metaphyseal segment below the humeral head is a crucial determinant of fracture stability.
Vascular Supply
The vascularity of the humeral head is primarily derived from branches of the axillary artery, specifically the anterior and posterior humeral circumflex arteries. The arcuate artery, a branch of the anterior humeral circumflex artery, ascends through the bicipital groove and supplies a significant portion of the humeral head, particularly the superior aspect. Damage to this critical blood supply, especially in multi-part fractures involving the anatomical neck or significant displacement, increases the risk of avascular necrosis (AVN) of the humeral head. For isolated greater tuberosity fractures, the risk of AVN to the main humeral head fragment is generally low, but care must be taken to ensure adequate blood flow to the tuberosity fragment itself for healing.
Soft Tissue Attachments and Biomechanics
The rotator cuff muscles exert substantial forces on the proximal humerus. The supraspinatus primarily abducts, while the infraspinatus and teres minor externally rotate. The subscapularis internally rotates. In the event of a greater tuberosity fracture, the superior and posterior displacement of the fragment is often driven by the unopposed pull of the supraspinatus and infraspinatus. Conversely, the pectoralis major, latissimus dorsi, and teres major muscles, inserting more distally, can contribute to adduction and internal rotation deformities of the humeral shaft, particularly in surgical neck fractures. The deltoid also plays a role in abduction. The periosteal sleeve around the surgical neck can provide significant intrinsic stability, especially in less displaced fractures, guiding the type of immobilization and dictating the potential for spontaneous reduction or stability during early motion.
Fracture Classification Systems
The Neer classification system remains widely used for proximal humeral fractures, categorizing them based on the number of displaced anatomical fragments (greater tuberosity, lesser tuberosity, surgical neck, anatomical neck) and the degree of displacement (>1 cm or >45 degrees angulation). This system aids in assessing fracture severity and guiding treatment decisions. The AO/OTA classification provides a more granular description based on location (A for extraarticular unifocal, B for extraarticular bifocal, C for intraarticular), further subdividing based on comminution and displacement. For greater tuberosity fractures, key parameters for displacement include superior migration, posterior migration, and retraction, which are critical for preventing impingement and restoring rotator cuff function.
Indications and Contraindications
The decision to pursue nonoperative or operative management for proximal humeral fractures, particularly those involving the greater tuberosity, is multifactorial and requires careful consideration of fracture characteristics, patient factors, and potential outcomes.
General Principles of Nonoperative Management
The foundational principle for nonoperative management is that the majority of proximal humerus fractures possess sufficient inherent stability or potential for healing with acceptable alignment to yield satisfactory functional outcomes. Critical factors influencing this decision include:
* Fracture Type: Extraarticular, 2-part fractures, especially those involving the greater tuberosity or surgical neck, are most commonly managed nonoperatively.
* Degree of Fragment Displacement: Minimally displaced or nondisplaced fractures are ideal candidates.
* Intrinsic Fracture Stability: Assessed by radiographic features such as impaction, intact medial calcar, and the integrity of the periosteal sleeve. Image intensification during clinical assessment can be helpful, especially in cooperative patients, to dynamically assess fracture stability through a small range of motion, though this is not routine practice.
Specific Indications for Nonoperative Care
Nondisplaced Greater Tuberosity Fractures:
These constitute a significant portion of cases suitable for conservative management. A nondisplaced greater tuberosity fracture typically involves minimal superior migration (<5 mm) and no significant posterior retraction, which would otherwise impede rotator cuff function or lead to impingement. The vast majority of these fractures can be managed nonoperatively. Fixation in situ may be warranted if a high risk of displacement is suspected, such as in active patients with poor bone quality or significant initial comminution.
Minimally Displaced 2-Part Fractures:
* Extraarticular 2-Part, Greater Tuberosity, Nondisplaced: This is the primary target group for nonoperative care.
* Surgical Neck Fractures: Typically, acceptable alignment criteria for nonoperative treatment include angulation less than 45 degrees and displacement less than 1 cm. Impacted surgical neck fractures are inherently stable and usually heal well with nonoperative treatment.
* Anatomical Neck Fractures: While rare, if truly nondisplaced and stable, nonoperative care may be considered, but the risk of AVN is high.
Patient-Specific Factors Favoring Nonoperative Treatment:
* Comorbidities: Patients with significant medical comorbidities (e.g., severe cardiopulmonary disease, uncontrolled diabetes) that increase surgical risk may be better served by nonoperative management, even with some less-than-ideal fracture alignment.
* Low Functional Demand: Elderly, sedentary individuals with low functional expectations may tolerate greater residual deformity without significant functional impairment.
* Poor Bone Quality: In severe osteoporosis, surgical fixation can be challenging and prone to implant loosening or cutout, making nonoperative management a safer choice in select cases.
Contraindications to Nonoperative Care
While nonoperative care is preferred for many patterns, certain situations necessitate operative intervention:
* Significant Displacement:
* Greater tuberosity fractures with >5 mm of superior displacement (due to impingement and rotator cuff dysfunction) or significant retraction.
* Surgical neck fractures with >1 cm displacement or >45 degrees of angulation.
* Displaced articular fragments with a step-off >2 mm.
* Fracture Instability: Unstable fracture patterns that are likely to displace during the healing phase, particularly in active patients. Without fixation, displaced proximal humerus fractures are rarely improved with closed fracture reduction, indicating the need for stabilization if reduction is deemed necessary.
* Open Fractures: Require surgical debridement and stabilization to prevent infection.
* Neurovascular Compromise: Acute nerve or vessel injury requiring surgical exploration and repair.
* Fracture-Dislocations: Require reduction and stabilization.
* Young, Active Patients: Higher functional demands often necessitate more anatomical reduction and stable fixation to ensure optimal long-term outcomes.
* Failure of Nonoperative Management: Persistent pain, progressive displacement, or functional limitations despite appropriate nonoperative care.
Operative versus Non-Operative Indications
The following table summarizes key indicators for choosing between operative and nonoperative management strategies:
| Feature | Non-Operative Management | Operative Management |
|---|---|---|
| Fracture Type | Extraarticular, 2-part (e.g., isolated GT, surgical neck) | 3-part, 4-part, fracture-dislocations, articular split fractures |
| Displacement | Minimally displaced (<5mm GT, <1cm surgical neck) | Significantly displaced (>5mm GT, >1cm surgical neck), unstable |
| Angulation | Minimal (<45 degrees surgical neck) | Significant (>45 degrees surgical neck) |
| Articular Involvement | None or minimally displaced intra-articular component (<2mm) | Significant articular step-off (>2mm), large head split |
| Stability | Stable (e.g., impacted, intact periosteal sleeve, medial calcar) | Unstable (e.g., comminuted, loss of medial support) |
| Patient Factors | Low demand, significant comorbidities, poor bone quality, non-compliant | High demand, active, good bone quality, compliant, young |
| Specifics | Nondisplaced greater tuberosity fractures | Failed nonoperative treatment, open fractures, neurovascular compromise |

Pre Operative Planning and Patient Positioning
While the primary focus of this discussion is nonoperative care, a thorough academic understanding necessitates knowledge of the considerations preceding operative intervention, particularly when nonoperative management is either contraindicated or has failed. This section outlines the essential steps in operative planning and patient positioning.
Imaging Assessment
Detailed preoperative imaging is critical for understanding fracture morphology and guiding surgical strategy.
* Standard Radiographs: Anteroposterior (AP), true AP (Grashey view), axillary, and scapular Y views are indispensable. These provide initial assessment of fracture type, displacement, and articular involvement.
* Computed Tomography (CT) Scans: Highly recommended for complex fracture patterns, especially those with articular extension, comminution, or significant displacement of the tuberosities. Three-dimensional (3D) reconstructions from CT data are invaluable for visualizing fragment orientation, assessing articular step-off, and planning implant placement.
* Magnetic Resonance Imaging (MRI): While not routinely indicated for acute fracture assessment, MRI can be useful in evaluating associated soft tissue injuries, such as rotator cuff tears (especially relevant for greater tuberosity fractures), or for assessing vascular compromise.
Patient Evaluation and Optimization
A comprehensive medical evaluation is crucial to identify and optimize comorbidities. This includes assessing cardiovascular and pulmonary function, managing diabetes, and addressing nutritional status. Anesthesia consultation is vital to discuss potential risks and appropriate anesthetic techniques. Patient functional demands, occupation, and social support network are also key considerations, influencing the ultimate treatment goal and rehabilitation plan.
Timing of Intervention
The timing of surgery is typically within 1-2 weeks of injury to minimize soft tissue swelling and contracture, facilitating reduction. However, emergent surgery is indicated for open fractures or neurovascular compromise. Delayed surgery (beyond 3 weeks) can be more challenging due to early callus formation and soft tissue fibrosis.
OR Setup and Patient Positioning for Operative Cases
For operative fixation of proximal humeral fractures, the patient is typically positioned in either the beach chair or supine position.
* Beach Chair Position: Offers excellent exposure for both anterior (deltopectoral) and lateral (deltoid-splitting) approaches. The head and torso are elevated, and the arm is free-draped to allow for full range of motion during surgery. Image intensifier access is generally good.
* Supine Position: Less commonly used for complex proximal humerus fractures, but can be an option. The arm is often placed on an arm board or free-draped, allowing for traction and manipulation.
Regardless of the position, meticulous sterile draping is essential. The image intensifier is positioned to allow for orthogonal views (AP and axillary) to confirm reduction and implant placement.
Detailed Surgical Approach and Technique
This section outlines the primary surgical approaches and techniques for proximal humeral fractures, acknowledging that these interventions are reserved for cases unsuitable for nonoperative management, or when nonoperative treatment fails. The choice of approach and fixation technique depends heavily on the fracture pattern, bone quality, and surgeon preference.
General Principles of Fixation for Proximal Humerus
The overarching goals of operative fixation are:
1. Anatomical Reduction: Especially critical for articular surfaces and tuberosities to restore rotator cuff mechanics and prevent impingement.
2. Stable Fixation: Sufficient to allow for early, controlled rehabilitation, minimizing the risk of secondary displacement or implant failure.
3. Preservation of Vascularity: Meticulous soft tissue handling to protect the humeral head blood supply.
Deltopectoral Approach
The deltopectoral approach is the most common and versatile for accessing the proximal humerus, particularly for plating techniques.
* Internervous Plane: This approach utilizes the internervous plane between the deltoid muscle (innervated by the axillary nerve) laterally and the pectoralis major muscle (innervated by the medial and lateral pectoral nerves) medially. The cephalic vein typically lies within this groove and can be mobilized laterally or medially.
* Dissection: A skin incision is made from the coracoid process distally along the deltopectoral groove. The cephalic vein is identified and protected, usually retracted medially. The deltoid and pectoralis major are then carefully retracted. The clavipectoral fascia is incised, exposing the underlying conjoined tendon (coracobrachialis and short head of biceps) and the neurovascular structures. The anterior humeral circumflex artery and axillary nerve run transversely approximately 5-7 cm distal to the acromion, requiring careful protection.
* Fracture Exposure and Reduction: The fracture fragments are identified. For surgical neck fractures, gentle traction, manipulation with percutaneous joysticks, or K-wires can be used to achieve reduction. For greater tuberosity fragments, sutures placed through the rotator cuff tendons can be used to pull the fragment into position. Anatomical reduction is confirmed with fluoroscopy.
* Fixation with Locking Plates: Locking plates (e.g., PHILOS plate systems) are the preferred method. The plate is positioned on the lateral aspect of the humerus, ensuring sufficient distal fixation and subchondral support proximally with locking screws. The plate should be placed slightly anterior to the bicipital groove to avoid impingement and facilitate screw placement. Screws are directed into the humeral head to capture the major fragments, including the tuberosities. For greater tuberosity fractures, additional sutures through the rotator cuff and around the plate may augment fixation.
Anterolateral (Deltoid-Splitting) Approach
This approach is less commonly used for complex multi-part fractures but can be advantageous for isolated greater tuberosity fractures or certain 2-part surgical neck fractures, offering more direct access to the lateral aspect of the proximal humerus.
* Dissection: A small longitudinal incision is made over the deltoid, typically 3-5 cm distal to the acromion. The deltoid muscle fibers are split longitudinally, protecting the axillary nerve which wraps around the surgical neck, typically 5-7 cm inferior to the acromial tip.
* Fixation for Greater Tuberosity Fractures: Once the greater tuberosity fragment is identified, it can be reduced using sutures placed through the rotator cuff. Fixation options include tension band wiring, lag screws with or without washers, or suture anchors for pure avulsion injuries. The goal is to restore the anatomical position of the tuberosity to prevent impingement and ensure optimal rotator cuff function.
Intramedullary Nailing
Intramedullary nailing can be an option for select 2-part surgical neck fractures, particularly those with associated diaphyseal extension or in patients with poor bone quality where plate fixation might be less secure. It is generally not preferred for fractures involving significant articular comminution or complex tuberosity patterns due to challenges in achieving anatomical reduction and rotation control.
Arthroplasty
For comminuted 3- or 4-part fractures, particularly in the elderly with poor bone quality or in cases of severe head split or fracture-dislocation with high AVN risk, shoulder arthroplasty (hemiarthroplasty or reverse total shoulder arthroplasty) may be the primary treatment choice. This is also a salvage option for failed open reduction internal fixation (ORIF) or established AVN.
Complications and Management
Both nonoperative and operative treatments for proximal humeral fractures carry potential complications. Understanding these and having strategies for their management is crucial for optimal patient care.
Complications of Nonoperative Treatment
Despite its advantages for appropriate indications, nonoperative management is not without risks:
* Stiffness and Adhesive Capsulitis: This is arguably the most common complication, particularly if immobilization is prolonged or rehabilitation is delayed. It can significantly limit range of motion and functional recovery.
* Malunion: Occurs when the fracture heals in an unacceptable anatomical position.
* Greater Tuberosity Malunion: Superior displacement of the greater tuberosity (>5 mm) can lead to subacromial impingement and impaired rotator cuff function, particularly with overhead activities.
* Surgical Neck Malunion: Excessive angulation or shortening can result in functional limitations, pain, and cosmetic deformity.
* Nonunion: While rare in properly selected cases of nonoperative management, especially for 2-part fractures, it can occur, particularly with significant comminution, inadequate immobilization, or poor biological healing potential.
* Nerve Irritation: Prolonged sling use or specific arm positions can occasionally lead to transient nerve irritation (e.g., ulnar nerve).
Complications of Operative Treatment
Surgical intervention introduces additional risks:
* Infection: A risk with any surgical procedure, ranging from superficial wound infection to deep periprosthetic infection.
* Neurovascular Injury: Iatrogenic damage to the axillary nerve, musculocutaneous nerve, or the axillary artery/vein can occur during surgical exposure or screw placement.
* Implant Failure: Screw cutout, plate pull-out, or hardware breakage can occur, particularly in osteoporotic bone or with premature weight-bearing.
* Avascular Necrosis (AVN): A significant concern in complex fracture patterns (e.g., 4-part fractures) where the blood supply to the humeral head is compromised. This can also be exacerbated by aggressive dissection.
* Glenoid Erosion: A long-term complication associated with hemiarthroplasty.
* Stiffness/Adhesive Capsulitis: Also common after surgery, especially if rehabilitation is not initiated appropriately or if there is significant scarring.
* Heterotopic Ossification: Aberrant bone formation in soft tissues around the joint, limiting motion.
* Secondary Displacement: Loss of reduction post-fixation.
Salvage Strategies
When complications arise, a structured approach to salvage is necessary:
- For Stiffness/Adhesive Capsulitis:
- Intensified physical therapy focusing on stretching and mobilization.
- Manipulation under anesthesia for recalcitrant cases, followed by immediate, aggressive therapy.
- Arthroscopic capsular release or open capsulotomy for severe, persistent stiffness.
- For Malunion:
- Greater Tuberosity Malunion with Impingement: If symptomatic, surgical options include osteotomy to reduce the tuberosity, or in some cases, excision of a non-united fragment. Rotator cuff repair may be needed if chronic impingement has led to tearing.
- Surgical Neck Malunion: For significant functional deficits, corrective osteotomy and revision fixation may be considered, though this is a challenging procedure. In elderly patients with severe malunion, shoulder arthroplasty might be the only viable option.
- For Nonunion:
- Revision surgery with debridement of the nonunion site, stable internal fixation, and bone grafting (autograft or allograft).
- In cases of bone loss or poor bone quality, conversion to shoulder arthroplasty (hemi or reverse TSA) may be necessary.
- For Avascular Necrosis (AVN) of the Humeral Head:
- For early, asymptomatic AVN, observation.
- For symptomatic AVN with collapse, surgical options include hemiarthroplasty or reverse total shoulder arthroplasty, depending on rotator cuff integrity and patient factors.
- For Infection:
- Debridement, irrigation, and intravenous antibiotics.
- Hardware removal may be necessary in chronic infections.
- Staged revision or arthroplasty for persistent infection or failed previous management.
- For Implant Failure:
- Revision surgery with stronger fixation, different implant type, or conversion to arthroplasty if bone stock is insufficient or fracture pattern is no longer amenable to internal fixation.
Common Complications and Salvage Strategies
| Complication | Incidence (General) | Salvage Strategy |
|---|---|---|
| Stiffness/Adhesive Capsulitis | High (nonoperative and operative) | Aggressive PT, manipulation under anesthesia, arthroscopic capsular release |
| Malunion | Moderate (nonoperative) | Corrective osteotomy (especially for GT), revision fixation, arthroplasty for severe deformity |
| Nonunion | Low to moderate | Revision surgery with bone grafting, conversion to arthroplasty |
| Avascular Necrosis (AVN) | Low to moderate (operative for complex fractures) | Observation, hemiarthroplasty, reverse total shoulder arthroplasty |
| Infection | Low (operative) | Debridement, antibiotics, implant removal, staged revision |
| Neurovascular Injury | Low (operative) | Exploration and repair, nerve grafting, tendon transfer for chronic palsy |
| Implant Failure | Low (operative) | Revision surgery with alternative fixation, conversion to arthroplasty |
| Impingement (GT malunion) | Low to moderate (nonoperative) | Surgical reduction of tuberosity, tuberosity excision |
Post Operative Rehabilitation Protocols
Rehabilitation is a cornerstone of successful recovery from proximal humeral fractures, whether managed nonoperatively or operatively. The goal is to restore pain-free range of motion, strength, and function while protecting the healing fracture. The progression must be individualized, considering fracture stability, fixation achieved (if operative), patient bone quality, and compliance. The three phases of nonoperative treatment are thus: 1. Immobilization, 2. Passive/assisted range of motion, and 3. Progressive resistance exercises.
General Principles of Rehabilitation
- Pain Management: Adequate pain control is essential to allow for participation in therapy.
- Early Motion (Controlled): Duration of Immobilization should be as short as possible, and as long as necessary. Early, controlled motion helps prevent stiffness and promotes cartilage nutrition, but must respect fracture stability.
- Gradual Progression: Exercises should progress incrementally, based on pain, healing status, and clinical assessment.
- Patient Education and Compliance: Critical for successful outcomes.
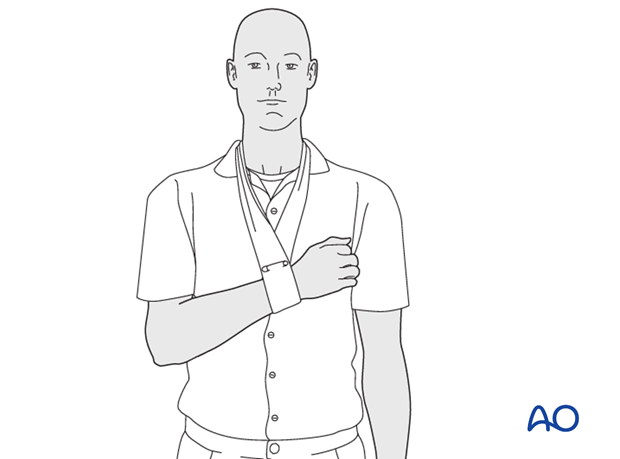
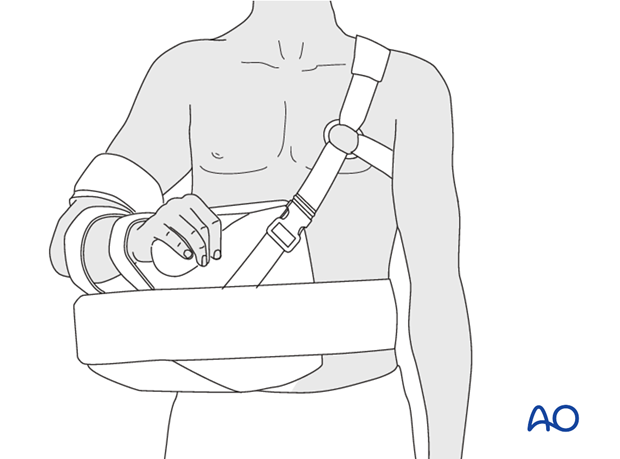
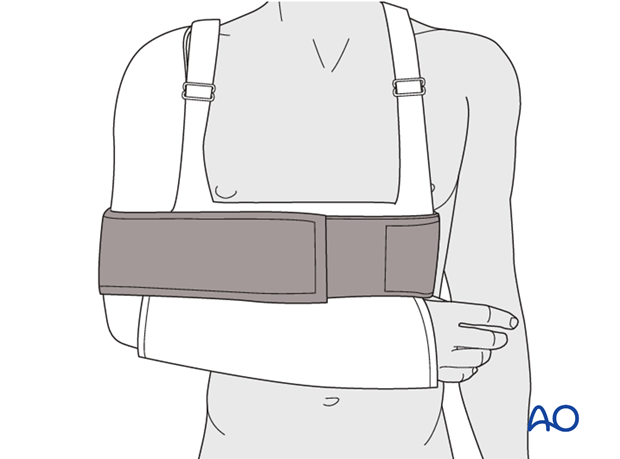
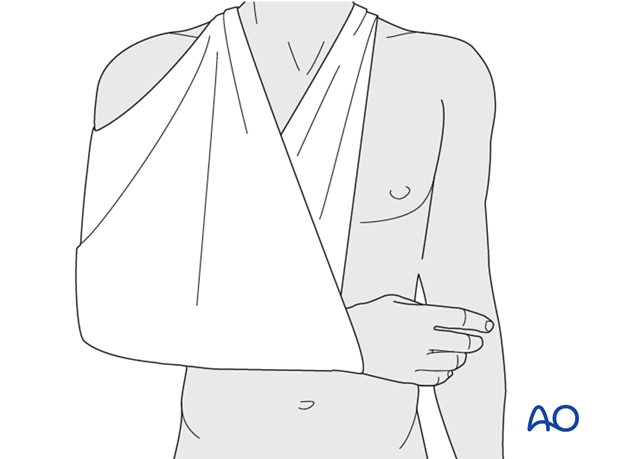
Phase 1: Immobilization and Protection (Weeks 0-3/4)
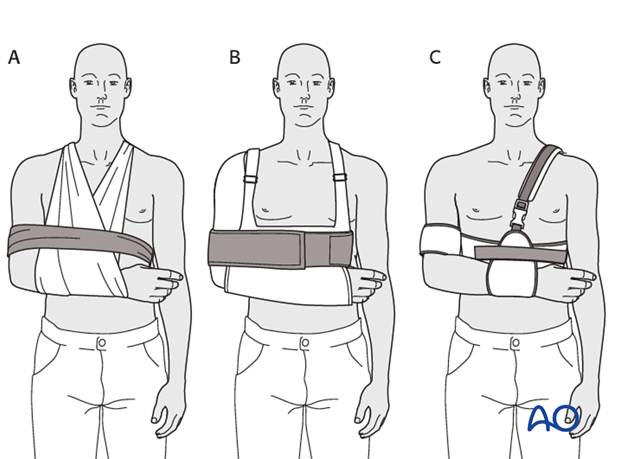
This initial phase focuses on protecting the healing fracture and minimizing pain.
* Immobilization Device: A sling or shoulder immobilizer is typically used. For fractures of the greater tuberosity and/or the surgical neck, the fracture may rest in better reduction if the arm is immobilized in abduction with a cushion (e.g., abduction pillow) to reduce tension on the rotator cuff and facilitate blood supply.
* Duration: Typically, immobilization is recommended for 2-3 weeks, followed by gentle range of motion exercises. Some stable fractures, especially non-displaced greater tuberosity fractures, may allow for earlier pendulum exercises (Codman's) around 7-10 days, provided pain allows.
* Goals: Reduce pain and swelling, protect fracture healing, maintain integrity of reduction, maintain range of motion in unaffected joints (elbow, wrist, hand).
* Activities:
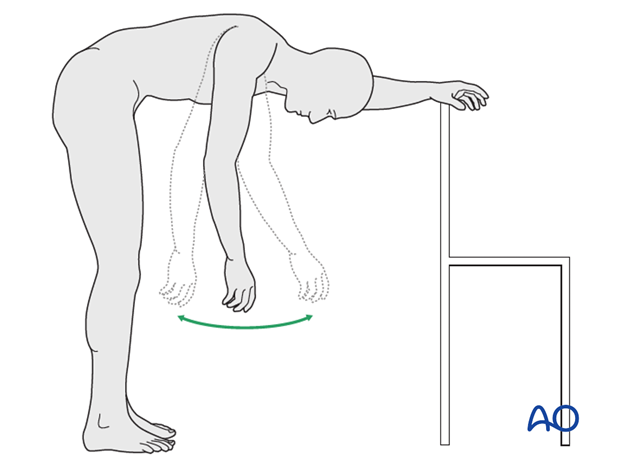
* Codman's Pendulum Exercises: Gentle, gravity-assisted swings of the arm while leaning forward, initiated as pain allows (often within the first 1-2 weeks for stable fractures).
* Isometric Exercises: Isometric exercises may help maintain strength during the first 6 weeks. These involve gentle muscle contractions without joint movement, performed for shoulder external rotators, internal rotators, deltoid, and biceps, taking care not to disrupt the fracture.
* Hand, Wrist, Elbow ROM: Active exercises for these joints are encouraged to prevent stiffness and promote circulation.
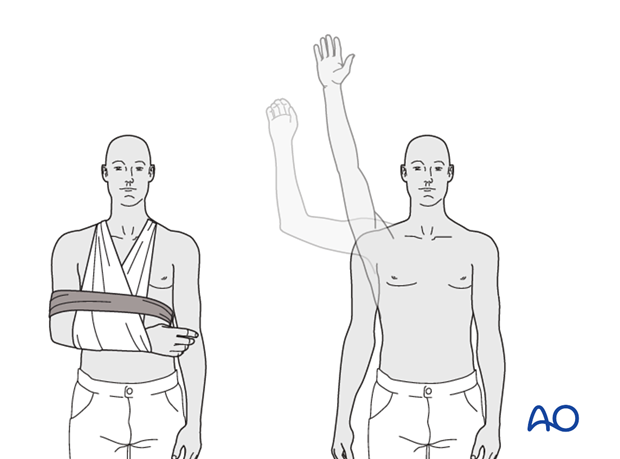
Phase 2: Passive/Assisted Range of Motion (Weeks 3/4-6/8)
Once the acute pain subsides and initial fracture stability is achieved, the focus shifts to restoring range of motion.
* Goals: Restore pain-free passive and assisted range of motion, prevent adhesive capsulitis, begin gentle scapular stabilization.
* Activities:
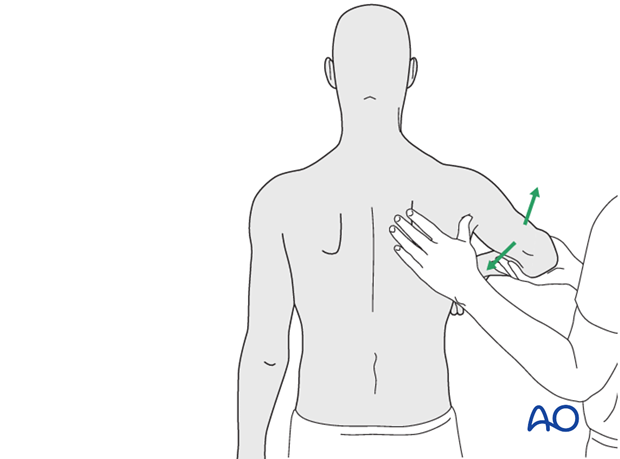
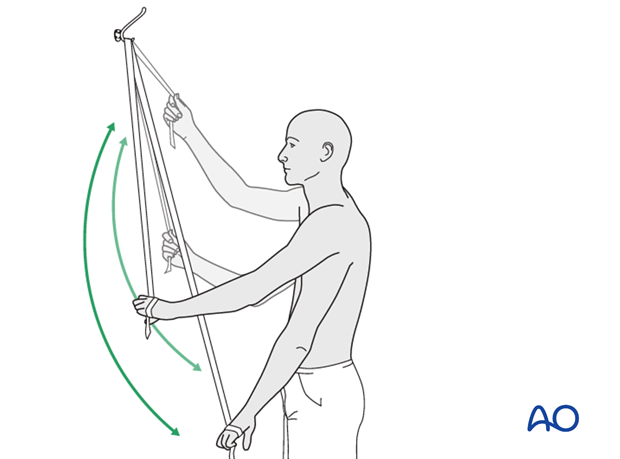
* Passive Range of Motion (PROM): Therapist-assisted or self-assisted (e.g., pulley system) exercises to gently increase flexion, abduction, and rotation. For greater tuberosity fractures, active abduction and external rotation must be carefully protected during this phase to allow for sufficient tendon-bone healing, typically avoiding these motions until 6-8 weeks.
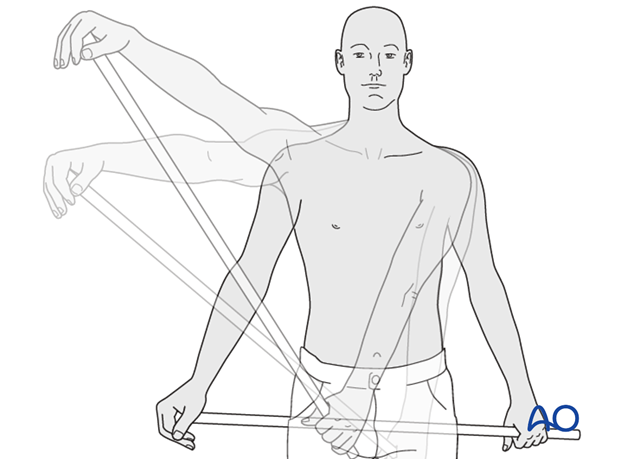
* Assisted Range of Motion (AAROM): Using the unaffected arm to assist the injured arm through movements.
* Scapular Stabilization Exercises: Gentle exercises to activate periscapular muscles (e.g., scapular squeezes) to provide a stable base for humeral movement.
* Progression: Gradual increase in intensity and range, always guided by pain.
Phase 3: Active Range of Motion and Progressive Strengthening (Weeks 6/8-12+)
With evidence of radiographic healing (e.g., callus formation) and good passive motion, active motion and strengthening can begin.
* Goals: Achieve full functional active range of motion, restore strength, improve endurance, prepare for advanced activities.
* Activities:
* Active Range of Motion (AROM): Initiating unassisted movements of the shoulder.
* Progressive Resistance Exercises: Resistance exercises can generally begin at 6 weeks. These include:
* Light Resistance Bands: For internal and external rotation, abduction, flexion.
* Light Weights: Gradually increasing resistance for shoulder muscles.
* Rotator Cuff Strengthening: Specific exercises for supraspinatus, infraspinatus, teres minor, and subscapularis. For greater tuberosity fractures, this component is critical and must be carefully supervised.
* Proprioceptive Exercises: Balance and coordination exercises for the shoulder joint.
Phase 4: Advanced Strengthening and Return to Activity (Weeks 12+)
This phase focuses on maximizing strength, power, and endurance, leading to a safe return to pre-injury activities.
* Goals: Full strength, power, and endurance; return to sport-specific or work-related activities.
* Activities:
* Heavy Resistance Training: Progression to heavier weights and more challenging resistance exercises.
* Plyometrics and Sport-Specific Drills: For athletes or individuals with high-demand occupations.
* Functional Training: Exercises mimicking daily activities or work tasks.
* Return to Activity: Gradual and guided by objective measures of strength, endurance, and pain. Full unrestricted activity, especially overhead, may take 6 months to a year.
Summary of Key Literature and Guidelines
The scientific literature on proximal humeral fractures, particularly regarding nonoperative management, has evolved significantly, emphasizing a personalized, evidence-based approach.
Evidence for Nonoperative Management
Numerous studies, including randomized controlled trials (RCTs) and systematic reviews, support the efficacy of nonoperative management for appropriately selected proximal humeral fractures.
* Two-Part Surgical Neck Fractures: Landmark studies have demonstrated that for nondisplaced or minimally displaced 2-part surgical neck fractures, nonoperative treatment yields outcomes comparable to operative fixation. A systematic review by Handoll et al. (2012) in the Cochrane Database of Systematic Reviews concluded that there is little evidence to support surgery over nonoperative treatment for these stable fracture patterns.
* Greater Tuberosity Fractures: For nondisplaced or minimally displaced greater tuberosity fractures (<5 mm displacement), nonoperative management with early controlled motion is the standard of care. Studies have shown excellent healing rates and functional outcomes, avoiding the risks of surgery. Even for slightly displaced fractures, some literature suggests good outcomes if displacement does not cause impingement or significant rotator cuff dysfunction. However, displacement >5 mm, particularly superiorly, is generally considered an indication for operative reduction and fixation to prevent impingement and restore rotator cuff mechanics.
* Elderly Patients: The pendulum has swung towards nonoperative management for many proximal humeral fractures in the elderly, even for some displaced patterns. Studies like the PROFHER trial (Jameson et al., 2016) found no significant difference in functional outcomes at 2 years between surgical fixation and nonoperative care for displaced proximal humerus fractures in adults, particularly in older patients. This seminal trial spurred a critical re-evaluation of treatment paradigms, underscoring that for many complex fractures, the benefits of surgery may not always outweigh the risks and recovery burden, especially in a population with lower functional demands and higher comorbidity rates.
AO Foundation Principles
The AO Foundation, a leading authority in orthopedic trauma, emphasizes a systematic approach to fracture management. For proximal humeral fractures, their principles advocate:
* Thorough Fracture Assessment: Utilizing Neer and AO/OTA classifications to accurately characterize the fracture.
* Patient-Centered Approach: Considering age, comorbidities, functional demands, and bone quality in decision-making.
* Stability Assessment: Prioritizing fracture stability. Nonoperative treatment is often recommended for stable, nondisplaced, or minimally displaced fractures.
* Early Mobilization: Promoting early, controlled motion whenever possible to prevent stiffness.
Current Consensus and Trends
The prevailing consensus is that nonoperative management remains the preferred option for most nondisplaced or minimally displaced proximal humeral fractures, including isolated greater tuberosity fractures and stable 2-part surgical neck fractures. In the elderly, there is an increasing trend to manage even some moderately displaced or multi-part fractures nonoperatively, especially those with stable fracture configurations or in frail patients. The decision for surgery is increasingly reserved for highly displaced, unstable fractures, fracture-dislocations, or younger, active patients requiring precise anatomical restoration. This paradigm shift is driven by a growing body of evidence questioning the universal superiority of operative intervention in terms of long-term functional outcomes for certain fracture types, particularly when weighed against the associated surgical risks and costs.
Future Directions
Future research will likely focus on:
* Personalized Medicine: Tailoring treatment decisions based on individual patient characteristics, fracture biology, and predictive models for nonunion or malunion.
* Advanced Imaging: Improved 3D imaging and functional imaging to better assess fracture stability and healing potential.
* Biologics: The role of biologics (e.g., PRP, stem cells) in enhancing fracture healing for both operative and nonoperative cases.
* Standardized Outcome Measures: Developing more robust, patient-reported outcome measures to accurately compare treatment efficacy.
Mastering nonoperative care for proximal humeral fractures, especially those involving the greater tuberosity, requires a blend of anatomical knowledge, careful patient selection, meticulous rehabilitation, and an evidence-based understanding of the literature. While surgical options exist for specific indications, a well-executed nonoperative protocol often provides excellent functional outcomes with fewer risks, making it a critical skill for every orthopedic surgeon and medical educator.
You Might Also Like


