Mastering Impaction Treatment MIO for Proximal Humeral Fractures

Key Takeaway
Discover the latest medical recommendations for Mastering Impaction Treatment MIO for Proximal Humeral Fractures. Impaction treatment MIO (Minimally Invasive Plate Osteosynthesis) for proximal humeral fractures involves plate fixation, reasonably considered for impacted surgical neck fractures. This technique offers enhanced stability and less soft-tissue damage than ORIF, facilitating earlier motion. It requires careful reduction, axillary nerve protection, and often additional tension band sutures to manage instability caused by disimpaction.
Introduction and Epidemiology
Proximal humeral fractures represent one of the most common osteoporotic fractures, accounting for approximately five percent of all adult fractures. The incidence follows a bimodal distribution, occurring in younger patients following high-energy trauma and in elderly patients following low-energy falls. Among these injuries, the extra-articular two-part surgical neck fracture is frequently encountered. When these fractures present with impaction, the proximal fragment (humeral head) is driven into the distal metaphyseal shaft, often resulting in a varus or valgus deformity.
While minimally displaced or impacted fractures with acceptable alignment can be managed conservatively, significant displacement or severe angulation necessitates surgical intervention. A significantly displaced greater tuberosity fracture, either in isolation or in conjunction with a surgical neck fracture, will impinge on the coraco-acromial arch. This pathoanatomy causes painful reduction of glenohumeral motion. Nonoperative treatment will not correct this mechanical block and should be strictly reserved for patients with unacceptably high surgical risk or severe medical comorbidities.
Minimally Invasive Osteosynthesis (MIO or MIPO) has emerged as a highly effective surgical strategy for impacted surgical neck fractures. By utilizing advanced angular stable implants and limited approaches, MIO aims to preserve the delicate soft-tissue envelope and periosteal blood supply, theoretically reducing the rates of avascular necrosis and nonunion compared to traditional open reduction and internal fixation (ORIF). However, the technique is technically demanding. Disimpaction of the fracture fragments inherently causes gross instability, which the subsequent plate fixation must biomechanically overcome.
Surgical Anatomy and Biomechanics
Osteology and Deforming Forces
The proximal humerus consists of four distinct anatomic segments: the articular segment (humeral head), the greater tuberosity, the lesser tuberosity, and the humeral shaft. Fractures typically occur along the epiphyseal lines separating these segments. In a two-part surgical neck fracture, the primary deforming force is the pectoralis major, which inserts on the lateral lip of the bicipital groove and pulls the humeral shaft anteromedially. Conversely, the rotator cuff musculature exerts distinct forces on the proximal fragment. The supraspinatus, infraspinatus, and teres minor pull the greater tuberosity superiorly and posteriorly, while the subscapularis pulls the lesser tuberosity medially.
Vascular Anatomy
Preservation of the vascular supply is the fundamental principle of the MIO technique. The primary arterial supply to the humeral head is derived from the anterior circumflex humeral artery (ACHA) and the posterior circumflex humeral artery (PCHA). The anterolateral branch of the ACHA (the arcuate artery of Laing) traditionally provided the major intraosseous supply. However, contemporary anatomic studies emphasize the critical contribution of the PCHA, which supplies the posterior, inferior, and lateral aspects of the humeral head. MIO techniques minimize disruption of the medial calcar periosteum, thereby preserving the terminal branches of the PCHA and reducing the risk of ischemic necrosis.
Neurologic Considerations
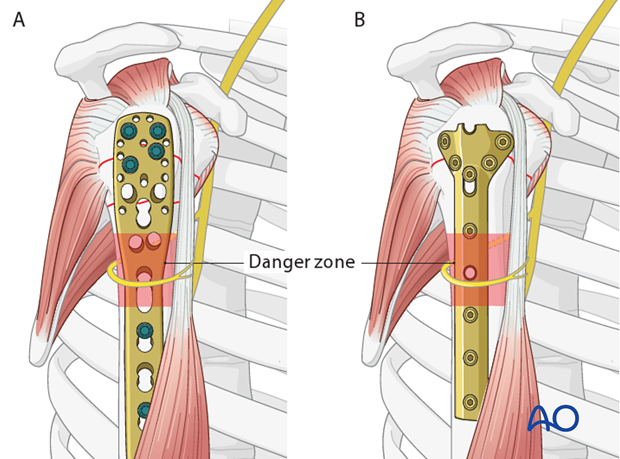
The primary neurologic structure at risk during minimally invasive plating of the proximal humerus is the axillary nerve. Arising from the posterior cord of the brachial plexus, the axillary nerve traverses the quadrangular space and courses circumferentially around the surgical neck from posterior to anterior, supplying the deltoid and teres minor muscles.
The nerve typically lies 5 to 7 centimeters distal to the lateral edge of the acromion. During the anterolateral or transdeltoid MIO approach, the axillary nerve must be meticulously protected. This is achieved by limiting the proximal incision to less than 5 cm distal to the acromial edge, directly palpating the subdeltoid space to identify the nerve's location, and avoiding any aggressive retraction or reduction maneuvers that could stretch or compress the nerve. Furthermore, the course of the nerve must be visualized mentally when placing preliminary K-wires or final locking screws.
Indications and Contraindications
The decision to proceed with MIO for proximal humeral fractures relies on an assessment of fracture morphology, bone density, patient functional demands, and surgical risk. Minimally invasive plate osteosynthesis can be reasonably considered for impacted surgical neck fractures where closed reduction or percutaneous manipulation is feasible.
Primary and Supporting Indications
The main indications for operative intervention include unacceptable deformity (typically defined as greater than 45 degrees of angulation or greater than 1 centimeter of translation) and a high risk of secondary displacement. Supporting indications for the MIO technique specifically include good bone quality, which facilitates percutaneous reduction maneuvers, and the clinical need for enhanced stability to permit earlier mobilization. MIO provides superior biomechanical stability compared to percutaneous pinning or screws alone and induces significantly less soft-tissue damage than standard ORIF.
Disadvantages and Contraindications
The primary disadvantage of surgical intervention in impacted fractures is the loss of inherent stability. Disimpaction causes immediate instability, which the fixation construct must completely overcome. Reduction can be technically difficult without direct visualization, and there is a continuous risk of iatrogenic damage to the axillary nerve. Absolute contraindications include active surgical site infection and unacceptably high anesthetic risk.
| Parameter | Operative Management MIO | Non Operative Management |
|---|---|---|
| Indications | Unacceptable deformity, varus >20 degrees, translation >50%, displaced GT >5mm | Minimally displaced, impacted in acceptable alignment, high surgical risk |
| Advantages | Restores anatomy, earlier mobilization, clears subacromial impingement | Avoids surgical/anesthetic risks, avoids axillary nerve injury |
| Disadvantages | Disimpaction causes instability, risk of nerve injury, hardware complications | Prolonged immobilization, stiffness, malunion, persistent impingement |
| Bone Quality | Ideal in good bone quality; requires angular stable plates in osteoporotic bone | Tolerates osteoporotic bone if inherently stable/impacted |
| Soft Tissue | Preserves periosteum better than ORIF, but requires precise tissue handling | Intact soft tissue envelope |
Pre Operative Planning and Patient Positioning
Imaging Protocol
Comprehensive radiographic evaluation is mandatory. A standard trauma series must include a true anteroposterior (Grashey) view, a scapular Y view, and an axillary lateral view. The axillary view is critical for evaluating glenohumeral dislocation and assessing the exact position of the tuberosities. In cases of complex impaction or suspected multi-part fractures, a non-contrast Computed Tomography (CT) scan with 3D reconstructions is highly recommended to delineate the fracture lines, quantify the degree of tuberosity displacement, and assess the available bone stock in the humeral head for screw purchase.
Patient Positioning and Setup
It is universally recommended to perform this procedure with the patient in a beach chair position.
The patient is positioned with the backrest elevated to approximately 45 to 60 degrees. The ipsilateral hemithorax is bumped to ensure the scapula is free and the shoulder extends completely off the edge of the operating table. This allows for unrestricted extension and rotation of the arm, which are vital maneuvers for closed reduction. A radiolucent arm board or a specialized hydraulic arm positioner can be utilized to maintain reduction during fixation.
The fluoroscopy (C-arm) unit should be brought in from the contralateral side or superiorly, depending on the exact table configuration. Prior to prepping and draping, the surgeon must verify that unhindered AP and axillary fluoroscopic views can be obtained. The entire forequarter, including the axilla, chest wall, and arm down to the fingertips, should be prepped and draped free to allow continuous manipulation.
Detailed Surgical Approach and Technique
Surgical Approaches
The surgeon must choose the approach best suited for the planned reduction maneuvers and the specific plate position. The two primary options for MIO of the proximal humerus are the anterolateral approach and the transdeltoid lateral approach.
The anterolateral approach utilizes the internervous plane between the anterior and middle heads of the deltoid (both innervated by the axillary nerve, but splitting the raphe is generally safe if not extended distally). A 3 to 5 cm incision is made starting at the anterolateral corner of the acromion and extending distally. The deltoid muscle fibers are bluntly split. The subacromial bursa is excised to expose the greater tuberosity and the lateral aspect of the humeral head.
Fracture Reduction Techniques
Because the fracture site is not fully exposed in a minimally invasive approach, the surgeon must be highly skilled at closed reduction maneuvers before considering MIPO.
Distal traction, perhaps augmented with increased angulation, will help to disimpact the fracture. The arm is placed in slight abduction and forward flexion to relax the deltoid and pectoralis major muscles. If closed traction is insufficient to disimpact the head, percutaneous techniques must be employed.
Use of an elevator or a Cobb instrument inserted through the proximal incision can facilitate disimpaction. The instrument is carefully slid between the fracture fragments to lever the humeral head out of varus or valgus impaction. Alternatively, threaded Schanz pins or heavy Kirschner wires (K-wires) can be inserted percutaneously into the humeral head to act as joysticks. Once disimpacted, the shaft is aligned to the head. Provisional fixation is achieved using multiple K-wires. The surgeon must meticulously remember the anatomical course of the axillary nerve when placing these temporary wires to avoid iatrogenic injury. Unless a satisfactory closed or minimally open reduction can be achieved, the surgeon must abandon the MIO technique and employ a standard open reduction (e.g., via a deltopectoral approach).
Plate Insertion and Fixation
Once provisional reduction is confirmed via orthogonal fluoroscopy, the submuscular extra-periosteal tunnel is created. A periosteal elevator is passed distally along the lateral humeral shaft, deep to the deltoid muscle and strictly deep to the axillary nerve.
This procedure typically utilizes an angular stable plate (locking plate).
Sometimes, these modern implants are not available. Standard plates provide an alternative option, for example, the modified cloverleaf plate. Presently, the specific indications, advantages, and disadvantages of angular stable and standard plates are being clarified in the literature. There is substantial biomechanical and clinical evidence that angular stable plates provide better outcomes, particularly in osteoporotic bone, by functioning as a fixed-angle construct that resists varus collapse. However, in addition to the type and technique of fixation, the quality of the anatomic reduction, soft-tissue handling, and the intrinsic characteristics of the injury and patient significantly influence the final results. There is no evidence that the mere use of angular stable plates will overcome poor reduction or rough tissue handling.
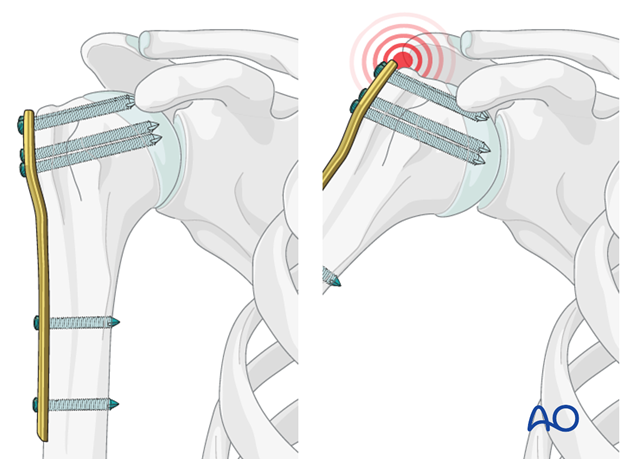
The plate is slid distally through the proximal window. A distal stab incision is made over the distal end of the plate to allow for screw insertion into the humeral shaft. The plate height is adjusted; it should sit approximately 5 to 8 mm distal to the superior tip of the greater tuberosity and slightly posterior to the bicipital groove to avoid impingement on the long head of the biceps tendon.
Proximal locking screws are inserted first. It is critical to place inferomedial screws (calcar screws) into the inferomedial quadrant of the humeral head. These screws provide essential mechanical support against the medial hinge, preventing secondary varus collapse. Following proximal fixation, the distal shaft screws are placed through the distal percutaneous window.
Rotator Cuff Tension Band Suturing
A critical adjunct to plate osteosynthesis in the proximal humerus is the use of tension band sutures. Sutures placed through the insertions of each rotator cuff tendon significantly increase the stability of the construct and should be used in conjunction with the plate and screws, particularly for more comminuted and/or osteoporotic fractures.
With osteoporotic bone, the tendon insertion is often stronger than the underlying cancellous bone itself. Consequently, heavy non-absorbable sutures (e.g., #2 or #5 braided composite sutures) placed through the insertional fibers of the supraspinatus, infraspinatus, and subscapularis tendons will hold better than screws or sutures placed directly through the bone. These sutures are passed through the dedicated suture holes in the proximal aspect of the locking plate and tied down securely. These additional sutures are typically the last step of fixation, effectively neutralizing the deforming forces of the rotator cuff and compressing the tuberosities against the plate and shaft.
Complications and Management
Despite meticulous surgical technique, MIO of the proximal humerus carries a distinct complication profile. The surgeon must be prepared to identify and manage these issues promptly.
Axillary Nerve Injury
The most feared complication specific to the MIO technique is iatrogenic injury to the axillary nerve. This can occur during the initial incision, during the creation of the submuscular tunnel, from aggressive retraction, or from direct trauma via drill bits or screws. Most injuries are neurapraxias resulting from traction and will resolve with conservative management over 3 to 6 months. If clinical and electromyographic (EMG) evidence demonstrates no recovery by 3 to 6 months, surgical exploration and potential nerve grafting or nerve transfer (e.g., medial triceps branch of the radial nerve to the axillary nerve) may be indicated.
Intra-articular Screw Penetration
Primary screw penetration occurs due to inaccurate depth measurement or failure to recognize penetration on intraoperative fluoroscopy. Secondary screw cutout occurs due to varus collapse of the humeral head, driving the fixed-angle screws through the articular cartilage into the glenoid. To prevent this, the surgeon must obtain dynamic intraoperative fluoroscopy, rotating the arm through a full range of motion while visualizing the joint space. If secondary cutout occurs, prompt removal or exchange of the offending screws is mandatory to prevent rapid destruction of the glenoid articular surface.
Avascular Necrosis (AVN)
Ischemic necrosis of the humeral head can occur due to the initial trauma disrupting the vascular supply or iatrogenic stripping during surgery. While MIO theoretically reduces this risk by preserving the medial periosteum, AVN remains a significant concern, particularly in fractures with a short medial calcar segment or disrupted medial hinge. Management depends on patient age and symptoms; young patients may tolerate mild AVN, while elderly or severely symptomatic patients may require conversion to a hemiarthroplasty or reverse total shoulder arthroplasty (RTSA).
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| Axillary Nerve Injury | 2% - 8% | Percutaneous tunneling, aggressive retraction, blind screw placement | Observation/EMG; Nerve transfer if no recovery at 3-6 months |
| Screw Cutout / Penetration | 5% - 15% | Osteoporosis, lack of calcar screws, initial varus malreduction | Hardware removal, exchange, or conversion to arthroplasty |
| Varus Collapse | 10% - 20% | Failure to restore medial hinge, omission of inferomedial calcar screws | Revision ORIF with bone grafting or Reverse Total Shoulder Arthroplasty |
| Avascular Necrosis | 4% - 10% | Disruption of PCHA/ACHA, short calcar segment (<8mm) | Observation if asymptomatic; Arthroplasty if painful and collapsed |
| Nonunion | 1% - 5% | Inadequate fixation, infection, severe soft tissue stripping | Revision ORIF with autologous bone graft, rule out indolent infection |
| Subacromial Impingement | 5% - 10% | Plate placed too high (>5mm above GT), unreduced GT fracture | Arthroscopic or open hardware removal, tuberosity debridement |
Post Operative Rehabilitation Protocols
Successful outcomes following MIO of proximal humeral fractures rely heavily on a structured, phased rehabilitation program. The protocol must balance the need for early mobilization to prevent adhesive capsulitis with the necessity of protecting the fracture fixation.
Phase 1: Maximum Protection (Weeks 0 to 4)
Immediately postoperatively, the patient is placed in a standard shoulder sling or immobilizer. The primary goal during this phase is to protect the surgical construct while minimizing distal edema and stiffness. Active range of motion (ROM) of the elbow, wrist, and hand is initiated on postoperative day one. Pendulum exercises are typically permitted within the first week, depending on bone quality and fixation stability. Passive forward flexion and external rotation in the scapular plane are initiated under the guidance of a physical therapist. Active shoulder motion is strictly prohibited to prevent displacement of the tuberosities or hardware failure.
Phase 2: Active-Assisted Motion (Weeks 4 to 8)
Once clinical and radiographic evidence of early callus formation is observed (usually around 4 weeks), the patient transitions to active-assisted range of motion (AAROM). The sling is gradually weaned and discontinued. Exercises such as pulley systems, wand exercises, and wall-walks are introduced. The focus is on restoring functional forward elevation and external rotation. Isometric strengthening of the deltoid and rotator cuff may begin late in this phase, provided there is no pain at the fracture site.
Phase 3: Active Motion and Strengthening (Weeks 8 to 12+)
At 8 weeks, assuming radiographic union is progressing satisfactorily, full active range of motion (AROM) is permitted. Progressive resistance exercises using elastic bands and light weights are incorporated to rebuild the strength of the rotator cuff and periscapular stabilizers. Advanced functional and sport-specific training is delayed until full clinical and radiographic union is achieved, typically between 3 and 6 months postoperatively.
Summary of Key Literature and Guidelines
The surgical management of proximal humeral fractures has been extensively debated in the orthopedic literature. The evolution from traditional ORIF to MIO reflects a broader trend toward biology-preserving techniques in fracture care.
Biomechanical studies have consistently demonstrated the superiority of angular stable (locking) plates over standard non-locking plates (such as the modified cloverleaf plate) in osteoporotic bone models. Locking plates function as a single biomechanical construct, converting shear forces into compressive forces at the bone-implant interface. Furthermore, the addition of inferomedial calcar screws has been biomechanically proven to significantly increase the load to failure and prevent varus collapse.
Clinical literature comparing MIO to standard deltopectoral ORIF suggests that MIO results in reduced intraoperative blood loss, shorter operative times, and potentially lower rates of avascular necrosis due to the preservation of the anterior circumflex humeral artery and the delicate soft-tissue attachments to the tuberosities. However, MIO is associated with a steep learning curve and a higher risk of radiation exposure to the surgeon due to the reliance on continuous fluoroscopy.
The incorporation of tension band sutures through the rotator cuff insertions is strongly supported by clinical guidelines. Studies indicate that in osteopenic models, suture fixation of the tuberosities to the plate provides superior resistance to displacement compared to screw fixation alone.
Ultimately, while the MIO technique utilizing angular stable plates offers distinct advantages in preserving biology and providing rigid fixation, the paramount determinants of clinical success remain the accurate restoration of anatomic alignment—particularly the medial hinge—and meticulous respect for the surrounding neurovascular structures.
Clinical & Radiographic Imaging
You Might Also Like