Greater Tuberosity Displaced: ORIF Techniques to Prevent Impingement

Key Takeaway
Here are the crucial details you must know about Greater Tuberosity Displaced: ORIF Techniques to Prevent Impingement. A **greater tuberosity displaced** fracture involves humeral head displacement impacting the coraco-acromial arch, causing pain and reduced motion. Treatment typically requires Open Reduction and Internal Fixation (ORIF), especially with displacement exceeding 5 mm. Fixation methods include screw fixation for single large fragments or tension band sutures, often anchored through tendons, for comminuted fractures or poor bone quality.
Introduction and Epidemiology
Fractures of the greater tuberosity (GT) are common injuries, particularly in the elderly population, often resulting from low-energy falls. While frequently seen in conjunction with anterior shoulder dislocations or as part of more complex proximal humerus fracture patterns, isolated greater tuberosity fractures represent a distinct clinical entity requiring specific consideration. These extraarticular, two-part fractures of the proximal humerus account for approximately 15-20% of all proximal humeral fractures. The significance of an isolated GT fracture lies in its critical role as the insertion site for the supraspinatus, infraspinatus, and teres minor components of the rotator cuff. Displacement of the GT fragment, therefore, directly compromises rotator cuff function and can lead to mechanical impingement against the coraco-acromial arch, causing persistent pain and significant limitation of shoulder abduction and external rotation.
Non-operative management, while considered for minimally displaced fractures, is largely inadequate for significantly displaced greater tuberosity fractures. Displacement exceeding 5 mm is widely accepted as the primary indication for surgical intervention due to the high likelihood of developing subacromial impingement and rotator cuff dysfunction. The powerful pull of the rotator cuff muscles, particularly the supraspinatus, tends to proximally and posteriorly retract the fracture fragment, exacerbating displacement and making spontaneous reduction improbable. Open reduction and internal fixation (ORIF) offers a reliable method to anatomically restore the GT position, facilitate rotator cuff healing, and prevent symptomatic impingement, thereby preserving shoulder kinematics and optimizing functional outcomes. This academic review delineates the critical aspects of ORIF for displaced greater tuberosity fractures, emphasizing techniques to mitigate postoperative impingement.
Surgical Anatomy and Biomechanics
Greater Tuberosity Anatomy
The greater tuberosity is a prominent bony landmark on the lateral aspect of the humeral head, serving as the primary attachment site for the majority of the rotator cuff musculature. Its superior facet provides insertion for the supraspinatus tendon, the middle facet for the infraspinatus, and the inferior facet for the teres minor. The subscapularis tendon inserts onto the lesser tuberosity, which is separated from the greater tuberosity by the bicipital groove. The height and contour of the greater tuberosity are crucial for normal glenohumeral articulation and unimpeded rotator cuff function. Proximally, the greater tuberosity sits beneath the coraco-acromial arch, a fibrous-osseous structure formed by the coracoid process, the coraco-acromial ligament, and the acromion. Any superior migration or malreduction of the GT fragment can directly impinge upon this arch, leading to subacromial pathology.
The blood supply to the greater tuberosity primarily originates from the ascending branch of the anterior circumflex humeral artery and the posterior circumflex humeral artery, forming a rich anastomotic network. Despite this, fracture patterns can disrupt local vascularity, potentially affecting bone healing, although avascular necrosis is rare for isolated GT fragments due to their typically robust soft tissue attachments.
Rotator Cuff Attachments and Biomechanical Implications
The rotator cuff muscles exert significant forces on the greater tuberosity. The supraspinatus, originating from the supraspinous fossa, inserts onto the most superior aspect of the GT. The infraspinatus and teres minor, arising from the infraspinous fossa, insert more posteriorly. In the event of a fracture, the unopposed pull of these muscles, particularly the supraspinatus, typically leads to superior and posterior displacement of the GT fragment. This displacement not only creates a mechanical obstacle beneath the acromion, causing impingement, but also disrupts the functional lever arm of the rotator cuff, thereby impairing active elevation and external rotation of the shoulder. The biceps tendon, residing within the bicipital groove, may occasionally become incarcerated in the fracture site, further complicating reduction and contributing to pain.
Biomechanically, precise anatomical reduction of the greater tuberosity is paramount. A malreduced fragment, particularly one that is superiorly or laterally prominent, will invariably lead to chronic impingement, pain, and functional deficits. The goal of ORIF is to restore the normal anatomical height and rotation of the tuberosity, thereby recreating a smooth articular surface and restoring the functional insertion of the rotator cuff to prevent impingement throughout the full range of shoulder motion.
Indications and Contraindications
Operative Indications
Surgical intervention for displaced greater tuberosity fractures is primarily driven by the risk of chronic subacromial impingement, rotator cuff dysfunction, and persistent pain. The most widely accepted criterion for operative management is a fracture displacement of 5 mm or more. However, other factors also influence the decision-making process:
- Displacement greater than 5 mm: This measurement is typically assessed on plain radiographs (AP, scapular Y, axillary views) or, more accurately, on computed tomography (CT) scans. Displaced fragments are prone to nonunion or malunion if not surgically corrected.
- Angulation of the fragment: Significant angulation can also lead to impingement, even if absolute displacement is less than 5 mm.
- Incarceration of the biceps tendon: The long head of the biceps tendon can be trapped within the fracture site, preventing reduction and requiring surgical intervention for release and repair.
- Associated injuries: Concomitant anterior shoulder dislocations, while often reducing the GT fracture spontaneously, may sometimes necessitate surgical intervention if reduction is incomplete or redisplacement occurs.
- Younger, active patients: Patients with high functional demands are generally better candidates for ORIF to ensure optimal restoration of shoulder mechanics.
- Significant functional deficit: Even with borderline displacement, if the patient exhibits a substantial loss of active shoulder motion, especially abduction or external rotation, ORIF may be indicated.
- Open fractures: Mandate surgical debridement and fixation.
Contraindications for Operative Management
While ORIF is generally recommended for significantly displaced GT fractures, certain patient and fracture characteristics may contraindicate surgical intervention:
- Severe comorbidities: Patients with American Society of Anesthesiologists (ASA) class III or IV scores or other significant medical comorbidities that preclude safe anesthesia and surgery.
- Non-ambulatory or low-demand patients: In individuals with limited functional expectations, the risks of surgery may outweigh the potential benefits.
- Severe osteoporosis: Extremely osteoporotic bone may not provide adequate purchase for implants, increasing the risk of hardware failure and comminution during fixation.
- Active infection: Local or systemic infection must be treated prior to elective orthopedic surgery.
- Pre-existing significant glenohumeral arthritis or rotator cuff arthropathy: In such cases, the underlying pathology may dominate the clinical picture, and a more comprehensive reconstructive procedure, such as arthroplasty, might be considered, or non-operative management for the GT fracture may be chosen if it's not the primary source of symptoms.
Operative versus Non-Operative Indications
The decision-making process for managing greater tuberosity fractures requires careful consideration of patient factors, fracture characteristics, and functional goals.
| Feature | Operative Management | Non-Operative Management |
|---|---|---|
| Fracture Displacement | Greater than 5 mm displacement or significant angulation on plain radiographs or CT scan. | Less than 5 mm displacement or minimal angulation. |
| Patient Age/Activity | Younger, active patients with high functional demands. Patients seeking full restoration of shoulder function. | Elderly, low-demand patients with significant comorbidities. Patients with limited functional goals. |
| Biceps Tendon Status | Biceps tendon incarceration within the fracture site. | Biceps tendon intact and not incarcerated. |
| Associated Injuries | Irreducible fracture-dislocations. Complex fracture patterns requiring anatomical restoration. | Isolated GT fracture without significant associated injuries. |
| Comorbidities | Acceptable surgical risk profile (ASA I or II, well-controlled chronic conditions). | Unacceptably high surgical risk (ASA III or IV, severe uncontrolled medical conditions). |
| Bone Quality | Adequate bone stock for implant purchase. | Severe osteoporosis precluding stable fixation. |
| Functional Impairment | Significant acute loss of active abduction/external rotation, indicating rotator cuff dysfunction due to displacement. | Minimal acute functional impairment, good passive range of motion. |
| Risk of Impingement | High risk of symptomatic subacromial impingement and rotator cuff impingement due to uncorrected displacement. | Low risk of impingement due to minimal displacement or fragment migration. |
| Healing Potential | Aims to achieve anatomical reduction and stable fixation, promoting primary bone healing and functional rotator cuff repair. | Relies on spontaneous healing, with acceptance of potential malunion or nonunion in low-demand individuals, provided function is not severely compromised or pain is manageable. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential to ensure a successful outcome and prevent complications. This involves comprehensive imaging review, surgical approach selection, and meticulous patient preparation.
Diagnostic Imaging and Assessment
- Plain Radiographs: Standard anteroposterior (AP), scapular Y, and axillary views are initial requirements. These help assess the fracture pattern, degree of displacement, and angulation. Specific views such as the true AP (Grashey) view are crucial for evaluating the glenohumeral joint space.
- Computed Tomography (CT) Scan: A CT scan with 3D reconstructions is often indispensable, especially for complex or multi-fragmentary GT fractures. It provides detailed information on the exact displacement (superior, posterior, medial), fragment size, comminution, and any potential intra-articular extension, which may not be evident on plain films. It also helps identify biceps tendon incarceration or associated glenoid rim fractures.
- Magnetic Resonance Imaging (MRI): While not routinely required for all GT fractures, an MRI can be useful if there is suspicion of concomitant rotator cuff tears, labral injuries, or biceps tendon pathology that might influence the surgical plan. It can confirm biceps incarceration.
Patient Preparation
- Anesthesia: General anesthesia is typically employed. Regional nerve blocks, such as an interscalene block, can be a valuable adjunct for both intraoperative and postoperative pain management, reducing opioid requirements.
-
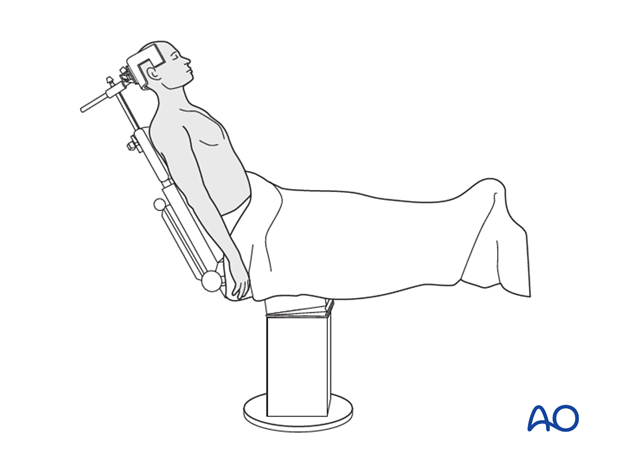
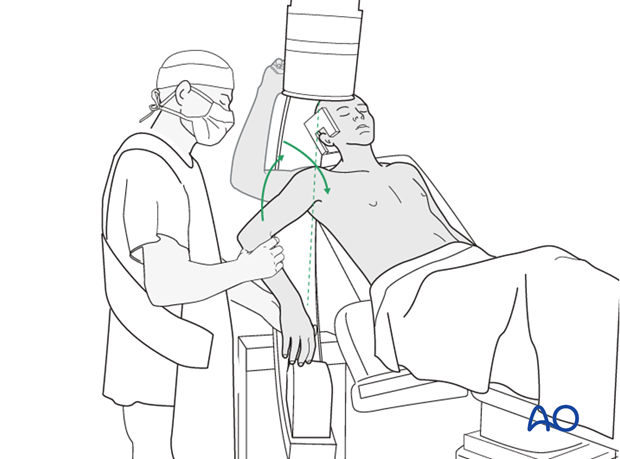
Patient Positioning: The beach chair position is the preferred setup for most shoulder procedures, including ORIF of the greater tuberosity. This position allows for excellent access to the shoulder, facilitates assessment of range of motion, and permits easy conversion to arthroscopic techniques if needed.
- The patient is positioned semi-recumbent, with the head supported by a headrest and the torso elevated 30-70 degrees.
- The operative arm should be draped free to allow for full manipulation during reduction and assessment of range of motion.
- The surgeon and assistant typically stand on the side of the operative shoulder.
- Adequate padding must be used to protect pressure points (occiput, sacrum, heels) and prevent ulnar nerve compression at the elbow.
- Consideration should be given to potential cerebral hypoperfusion in steeply elevated positions, especially in patients with cerebrovascular disease.
As an alternative, the supine position can be utilized, particularly for patients who cannot tolerate the beach chair position or for surgeons who prefer this setup. In the supine position, a padded bolster may be placed beneath the ipsilateral scapula to protract the shoulder and provide better access. The arm is again draped free.
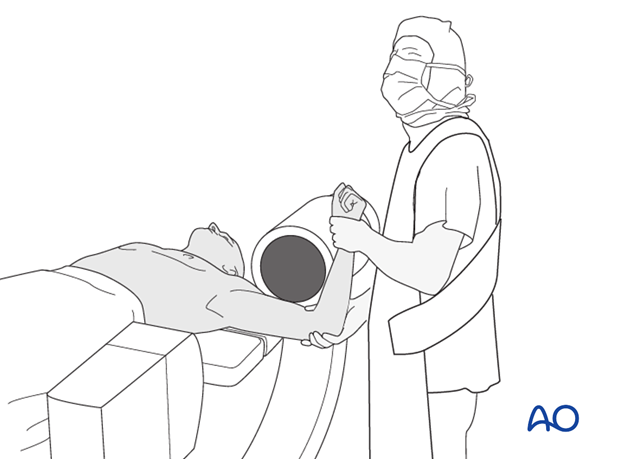
* C-arm Positioning: The fluoroscopy unit (C-arm) should be positioned to allow for unobstructed anteroposterior (AP) and axillary lateral views of the shoulder without repositioning the patient or the arm. This typically involves placing the C-arm on the contralateral side of the patient, allowing it to swing freely.
Detailed Surgical Approach and Technique
The goal of ORIF for a displaced greater tuberosity fracture is anatomical reduction and stable fixation to restore rotator cuff function and prevent impingement.
Surgical Approaches
The choice of surgical approach depends on the precise location and displacement of the greater tuberosity fragment. The aim is to choose the least invasive approach that provides adequate exposure for reduction and fixation.
-
Anterolateral Approach (Deltoid Split Approach): This is often the preferred approach for isolated greater tuberosity fractures, particularly those with superior or posterior displacement.
- A skin incision, typically 4-6 cm, is made longitudinally from the acromion distally, centered over the greater tuberosity.
- The deltoid fibers are split in line with their fibers, usually between the anterior and middle heads. Care must be taken to stay within 5 cm distal to the acromion to avoid injury to the axillary nerve, which typically crosses the deltoid approximately 5-7 cm distal to the acromial border.
- This approach provides direct access to the greater tuberosity and the rotator cuff insertion.
- Disadvantage: Limited exposure if the fracture extends significantly medially or anteriorly.
-
Transdeltoid Lateral Approach: Similar to the anterolateral approach in principle, offering direct access to the lateral aspect of the greater tuberosity. It is essentially a variation of the deltoid split.
- The incision is made more laterally, over the lateral aspect of the acromion, extending distally.
- The deltoid is split as described for the anterolateral approach.
- This approach is particularly useful for fragments that are primarily laterally or superiorly displaced.
-
Deltopectoral Approach: While more commonly used for complex proximal humerus fractures, the deltopectoral approach offers a wide exposure of the anterior aspect of the humerus and glenohumeral joint.
- An incision is made along the deltopectoral groove.
- The cephalic vein is identified and typically retracted laterally with the deltoid.
- This approach provides excellent visualization of the bicipital groove and lesser tuberosity, and can be extended distally if needed.
- It is less direct for purely superiorly displaced GT fractures but can be advantageous if there is concern for biceps tendon pathology, anterior extension of the fracture, or if a plate fixation strategy is anticipated.
- Care must be taken to protect the axillary nerve superiorly and the musculocutaneous nerve more medially.
Soft Tissue Dissection and Fracture Exposure
Once the chosen approach has been performed, the underlying tissues are carefully dissected.
- The subacromial bursa is opened and excised or retracted to expose the rotator cuff tendons and the fracture site.
-
Hematoma and any interposed soft tissue (e.g., biceps tendon, periosteum) must be thoroughly cleared from the fracture bed to allow for anatomical reduction and promote bone-to-bone healing. This step is critical.
-
Reflect the periosteum 2-3 mm back from the fracture line if necessary, to ensure a clean margin for reduction.
- Inspect the biceps tendon within the bicipital groove. If incarcerated, it must be gently extracted and protected. In cases of significant fraying or instability, a biceps tenodesis or tenotomy may be considered, although this is less common for isolated GT fractures.
Reduction and Preliminary Fixation
Anatomical reduction is the cornerstone of preventing impingement and ensuring successful rotator cuff repair.
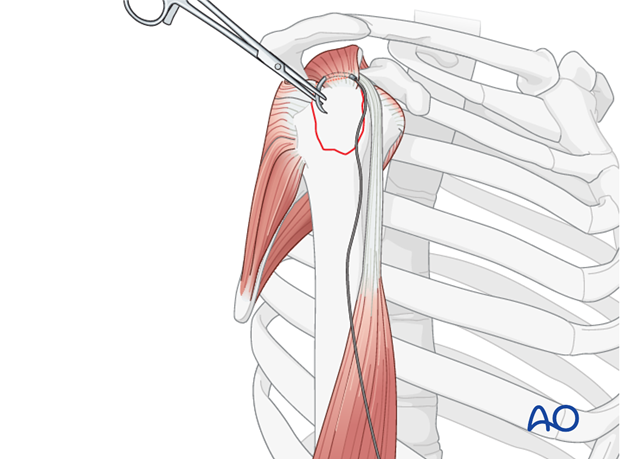
-
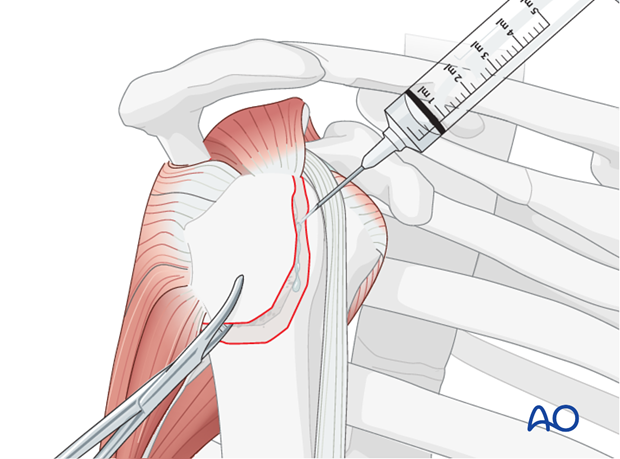
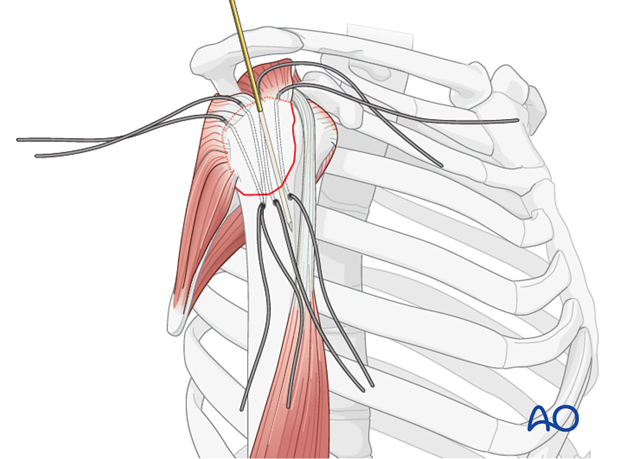
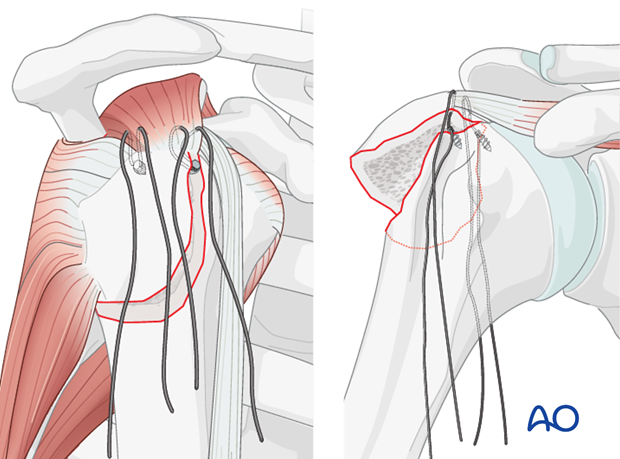
Stay Sutures: Place strong, non-absorbable stay sutures (e.g., #2 or #5 FiberWire) through the substance of the rotator cuff tendons attached to the greater tuberosity fragment, typically the supraspinatus and infraspinatus. These sutures act as "joysticks" to manipulate the fragment.
-
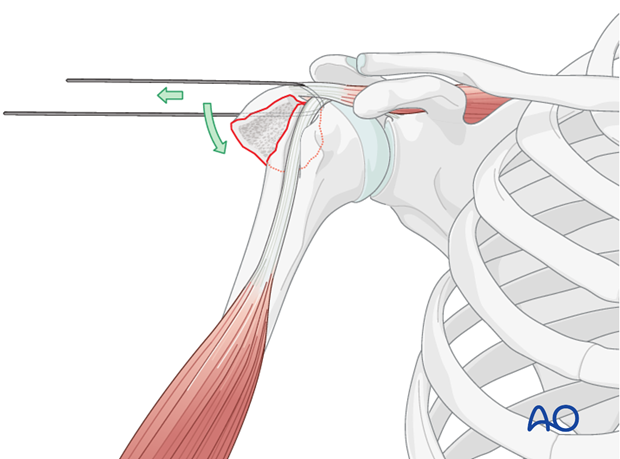
Direct Reduction: Using the stay sutures and a blunt instrument (e.g., periosteal elevator or a Freer elevator), gently pull and push the greater tuberosity fragment into its anatomical position on the humeral head. Ensure that the fracture margins are flush and that the articular surface of the humeral head is smooth. Avoid forceful manipulation that could fragment the tuberosity.
- Indirect Reduction: If direct visualization is challenging, external rotation and slight abduction of the arm can sometimes aid in bringing the fragment into better alignment.
-
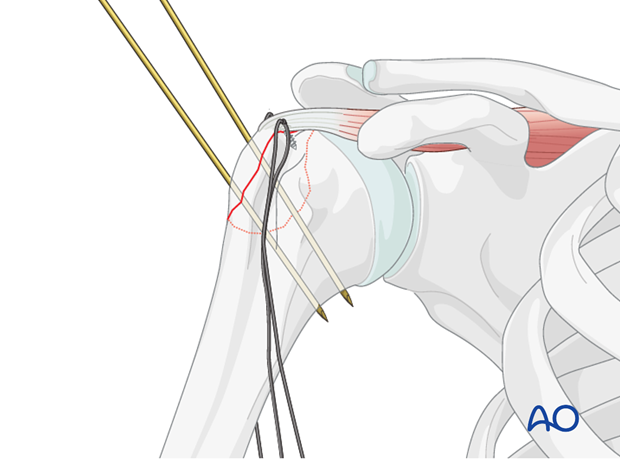
Preliminary Fixation: Once anatomical reduction is achieved, maintain it with temporary K-wires. These wires can be placed obliquely across the fracture line, taking care to avoid the articular surface. Intraoperative fluoroscopy is essential to confirm anatomical reduction in multiple planes (AP and axillary views) before definitive fixation.
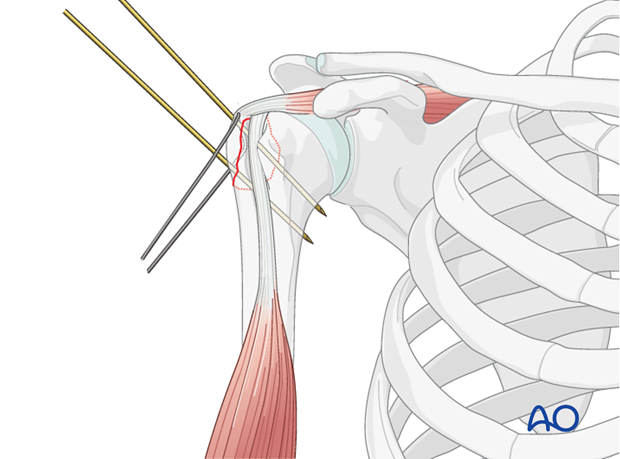
The K-wires provide stability while the definitive fixation method is prepared.
Definitive Fixation Techniques
Several methods can be employed for definitive fixation, each with its advantages and biomechanical considerations. The choice depends on fragment size, bone quality, and surgeon preference.
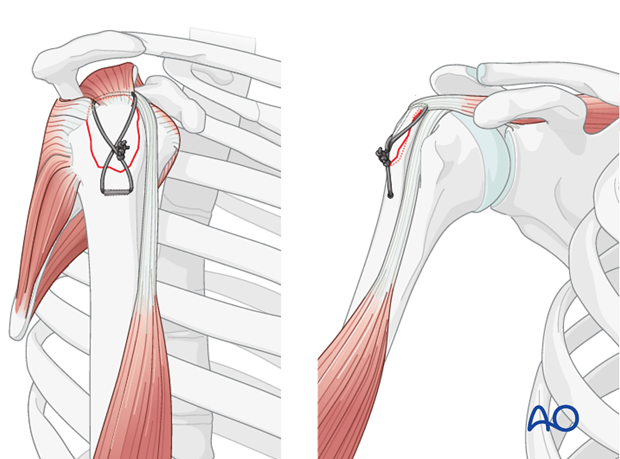
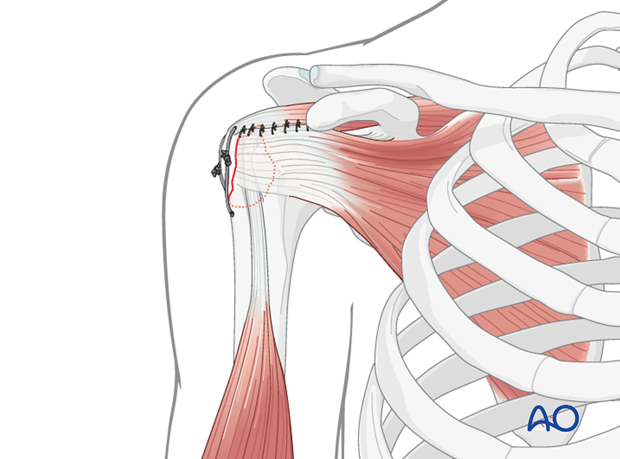
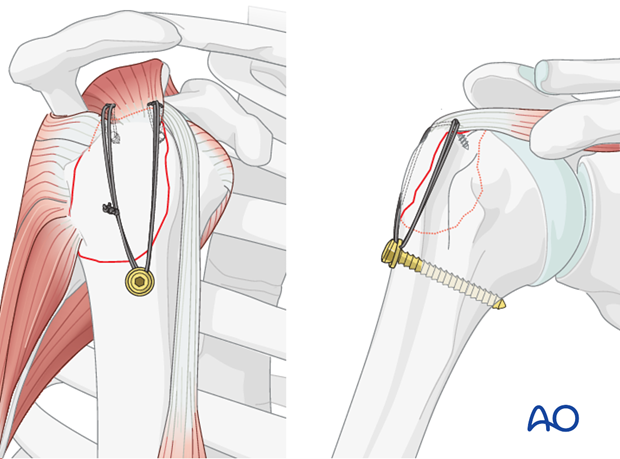
1. Suture Fixation
Suture fixation is a robust and commonly used technique, particularly for larger fragments with good bone quality, and integrates well with rotator cuff repair principles.
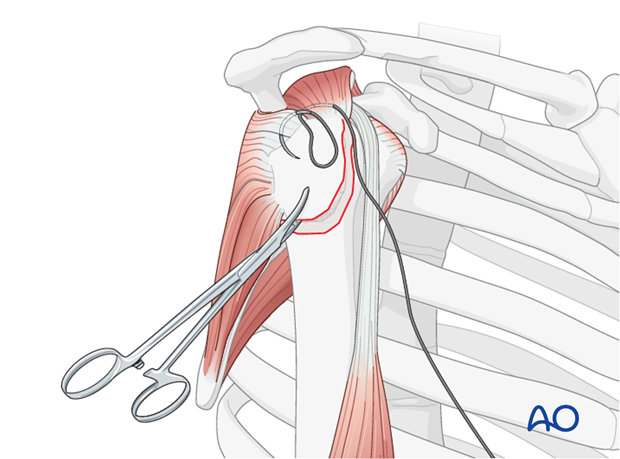
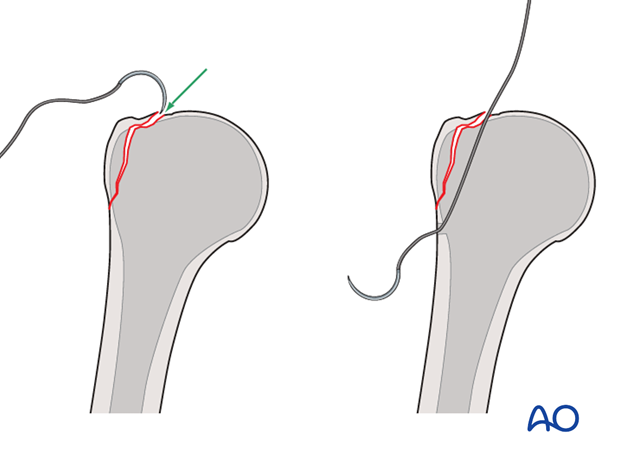
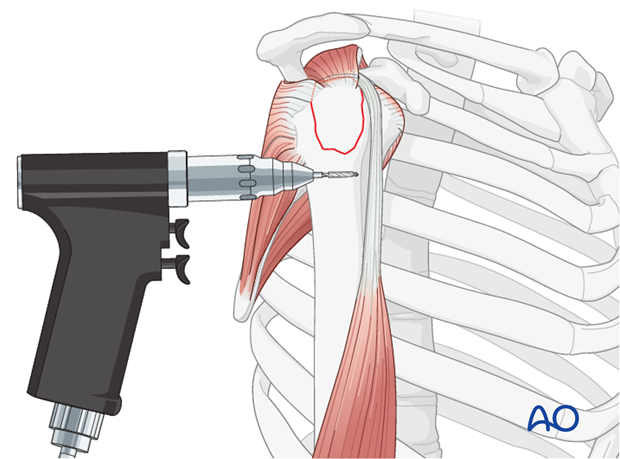
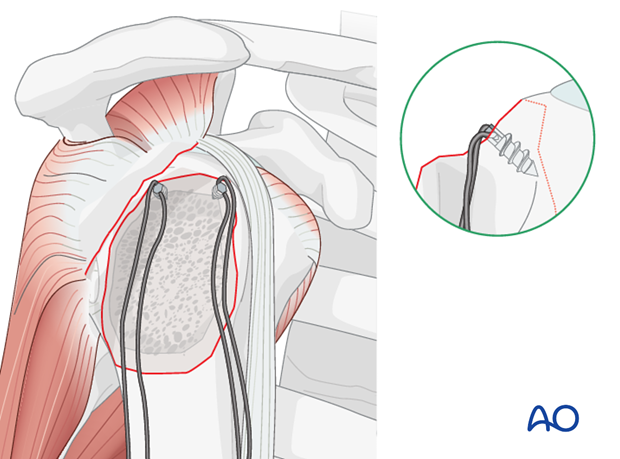
- Transosseous Sutures: After provisional K-wire fixation, drill two or more transosseous tunnels (1.5-2.0 mm) from the lateral cortex of the humeral shaft, distal to the fracture, exiting just medial to the fracture line on the humeral head.
-
Pass the previously placed stay sutures (or new sutures) from the rotator cuff through these tunnels and tie them over the lateral cortex or through a bone bridge. The sutures should provide firm compression of the fragment against the humeral head.
-
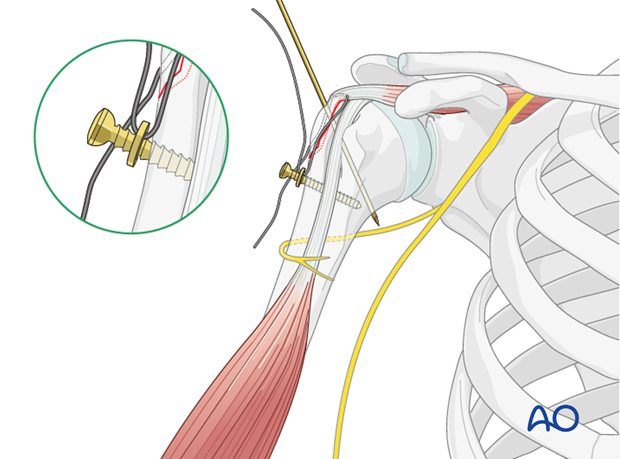
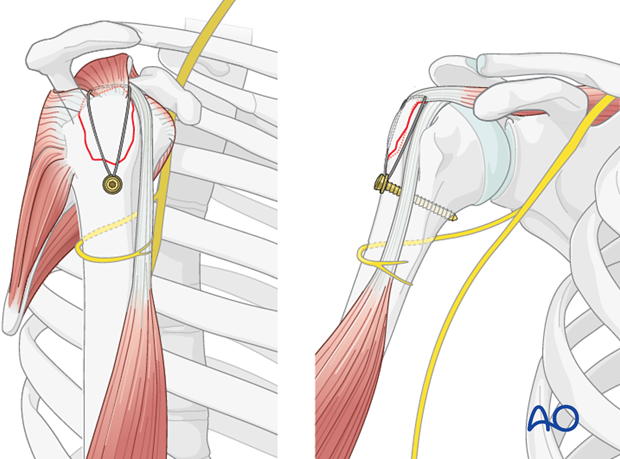
Suture Anchors: Suture anchors can be used as an alternative or adjunct. One or more anchors are placed into the humeral head just medial to the fracture bed. The sutures from the anchors are then passed through the rotator cuff substance and tied, compressing the fragment.
-
Suture Bridge Technique: This technique, commonly used in rotator cuff repair, can be adapted for GT fractures, especially if there's significant associated cuff injury. Medial anchors are placed, sutures are passed through the fragment, and then tied down to lateral cortical buttons or additional anchors more distally on the humeral shaft, creating a "suture bridge" that compresses the fragment.
Suture fixation offers the advantage of being biological, providing a broad area of compression, and facilitating rotator cuff healing. It is less prone to hardware prominence compared to screws.
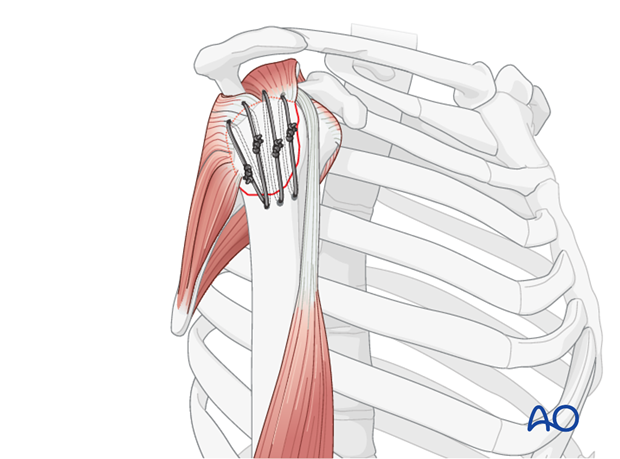
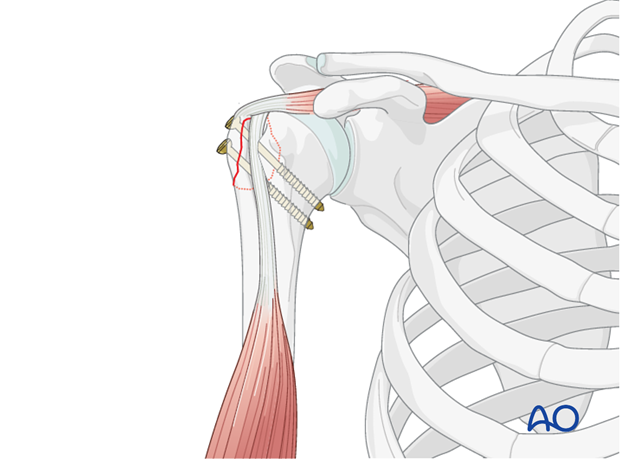
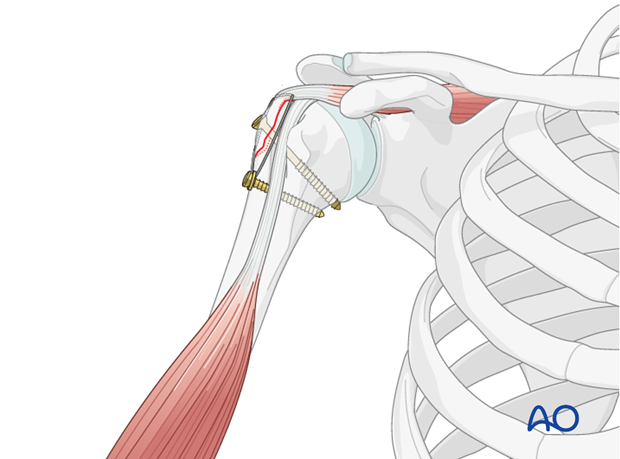
2. Screw Fixation
Screw fixation is another viable option, particularly for larger, stable fragments with good bone quality.
-
Cannulated Screws (Partially Threaded): Two or more cannulated, partially threaded screws (e.g., 4.0 mm or 4.5 mm) can be used to achieve lag screw effect, providing interfragmentary compression.
- The screws are inserted percutaneously or through the open incision, aiming from the lateral cortex of the humerus across the fracture line into the humeral head.
- Careful trajectory planning is crucial to avoid hardware prominence subacromially or intra-articularly.
- The screw heads should be flush with the lateral cortex.
- Fluoroscopy guidance is critical during insertion to confirm screw length and position.
-
Headless Compression Screws: These screws offer the advantage of being buried beneath the articular surface or within the bone, reducing the risk of impingement. They are particularly useful for smaller fragments or when minimal hardware prominence is desired.
- They are typically inserted from the superior aspect of the GT fragment, directed inferomedially into the humeral head.
- The use of headless screws requires meticulous drilling and countersinking to ensure proper seating.
Screw fixation provides rigid interfragmentary compression, which can promote primary bone healing. However, screws can become prominent, especially in cases of inadequate countersinking or if the fragment shifts, leading to secondary impingement.
3. Plate Fixation
While less commonly used for isolated two-part greater tuberosity fractures, plate fixation may be considered in specific scenarios:
- Small, comminuted fragments: If the GT fragment is comminuted or too small for adequate screw purchase, a small fragment plate or a specific GT plate may be used as an adjunct.
-
Associated shaft fractures: In more complex proximal humerus fractures involving the metaphysis or shaft, a locking plate designed for proximal humerus fractures may be extended to capture the greater tuberosity fragment, effectively treating it as part of a larger fracture pattern.
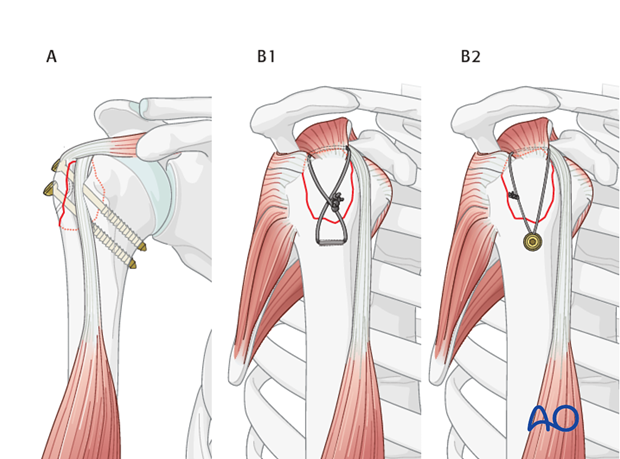
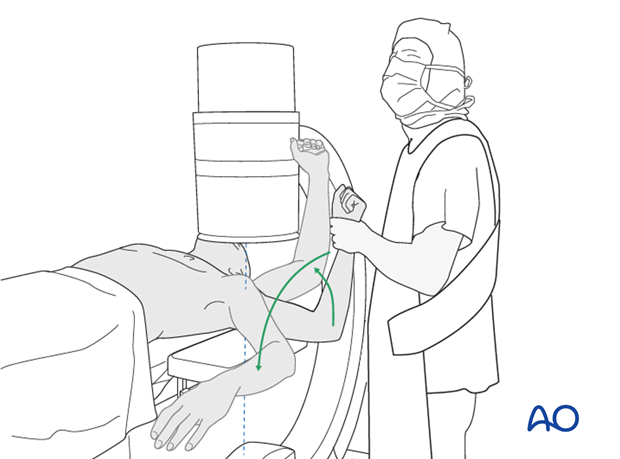
Plate fixation offers angular stability, which can be beneficial in osteoporotic bone. However, hardware prominence is a significant concern with plates in the subacromial space.
Final Assessment and Closure
- Intraoperative Fluoroscopy: After definitive fixation, obtain AP, lateral, and axillary fluoroscopic views to confirm anatomical reduction, proper implant position, and absence of intra-articular or subacromial hardware prominence.
- Range of Motion Assessment: Gently move the shoulder through a full range of passive motion (abduction, rotation). Observe for any signs of impingement or crepitus, which would indicate residual malreduction or prominent hardware. Correct any issues immediately.
- Rotator Cuff Integrity: Confirm the integrity of the rotator cuff repair. If the deltoid was split, repair it meticulously.
- Wound Closure: After thorough irrigation, close the surgical wound in layers. Subcutaneous sutures and skin sutures or staples are used. A drain is usually not necessary but may be considered for extensive hematoma or in patients with coagulopathy.
-
Dressing and Immobilization: Apply a sterile dressing and immobilize the arm in a sling with an abduction pillow, depending on the stability of the fixation and surgeon preference. The abduction pillow helps prevent medial translation of the humeral head, which can stress the repair.
(Note: The imagewas provided without a proper URL. Assuming it was a placeholder or corrupted, it cannot be rendered. If a valid URL becomes available, it should be placed here.)
(Note: The imagewas provided but not given a specific description. It can be interpreted as another intraoperative view related to reduction or cleaning, and thus placed here in the general surgical technique flow.)

Complications and Management
Despite meticulous surgical technique, complications can occur following ORIF of greater tuberosity fractures. Awareness and prompt management are critical for optimizing patient outcomes.
Common Complications
| Complication | Incidence (Approximate) | Description | Salvage Strategies |
|---|---|---|---|
| Malunion | 5-20% | The most significant complication for GT fractures, leading to persistent subacromial impingement, pain, and restricted range of motion (especially abduction and external rotation). Occurs if the fragment heals in a displaced or angulated position (e.g., >5mm superiorly or posteriorly). Rotator cuff dysfunction results from altered lever arm. | Early (within 3-6 months): Revision ORIF with osteotomy and re-fixation if anatomical reduction is still achievable. Late (after 6 months): Debridement of scar tissue, subacromial decompression (arthroscopic or open acromioplasty), possible tuberosity osteotomy with refixation (if viable) or excision of a small, prominent fragment. For significant functional deficit, reverse shoulder arthroplasty might be considered in carefully selected older patients with irreparable cuff. |
| Nonunion | 2-10% | Failure of the fracture fragment to heal, resulting in a fibrous union or pseudarthrosis. Leads to persistent pain, weakness, and rotator cuff dysfunction due to lack of stable attachment. | Symptomatic Nonunion: Revision ORIF with meticulous debridement of the nonunion site, fresh bleeding bone preparation, bone grafting (autograft or allograft), and rigid fixation (screws, sutures, or small plate). Consider biological augmentation (e.g., PRP) in selected cases. Asymptomatic Nonunion: May be observed in very low-demand patients if pain is minimal, but typically warrants intervention. |
| Hardware Prominence | 5-15% | Screws or sutures knots projecting above the cortex, irritating the deltoid, subacromial bursa, or impinging on the acromion. Can lead to pain and necessitate removal. More common with screw fixation than suture fixation. | Symptomatic Hardware: Hardware removal after fracture union (typically 6-12 months post-op). If symptoms are severe and occur early, partial or complete hardware removal may be necessary before complete union, risking loss of reduction. Revision to less prominent fixation (e.g., headless screws, sutures) in rare, early cases. |
| Infection | <1-2% | Superficial or deep surgical site infection. Presents with pain, erythema, swelling, warmth, purulent drainage, and systemic signs (fever, elevated inflammatory markers). | Superficial: Oral antibiotics, local wound care. Deep: Urgent surgical irrigation and debridement, tissue culture-guided intravenous antibiotics (6 weeks), hardware retention if stable and infection is controlled, or removal if infection persists or bone is involved. May require two-stage revision in severe cases. |
| Rotator Cuff Retear | 5-15% | Re-rupture or failure of healing of the rotator cuff insertion to the tuberosity. Can occur due to poor bone quality, excessive early motion, or inadequate fixation. Leads to pain, weakness, and loss of motion. | Symptomatic Retea: Revision rotator cuff repair. May involve augmentation with allograft or autograft. If irreparable, consider superior capsular reconstruction or reverse shoulder arthroplasty in appropriate candidates. |
| Neurovascular Injury | <1% | Injury to the axillary nerve (deltoid innervation) or musculocutaneous nerve, or rarely the posterior circumflex humeral artery. Causes deltoid weakness or paralysis, sensory deficits, or bleeding. | Axillary Nerve Palsy: Observation with electrodiagnostic studies. Surgical exploration and nerve repair/grafting if no recovery after 3-6 months. Vascular Injury: Immediate surgical repair. |
| Stiffness / Arthrofibrosis | 5-10% | Restricted range of motion due to capsular contracture or extensive scarring. Can be exacerbated by prolonged immobilization or inadequate rehabilitation. | Aggressive physical therapy, potentially with supervised manipulation under anesthesia. Arthroscopic capsular release or open release for recalcitrant cases. |
| Biceps Tendon Pathology | Uncommon (post-ORIF) | Persistent pain or symptoms related to the biceps tendon, such as tenosynovitis or rupture, if not addressed during the initial surgery or if the tendon becomes irritated by hardware. | Symptomatic: Biceps tenodesis or tenotomy. |
Post Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is crucial for achieving optimal functional outcomes and preventing complications such as stiffness or retear after greater tuberosity ORIF. The protocol balances protection of the healing fracture and rotator cuff with the need to restore motion and strength.
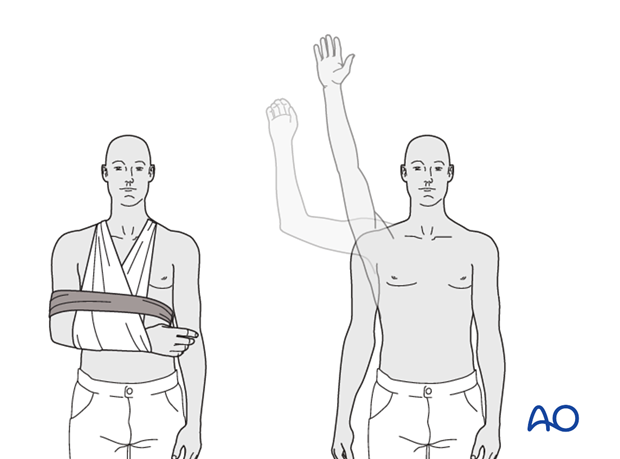
Phase 1: Immobilization and Early Passive Motion (0-6 weeks)
- Goal: Protect the surgical repair, control pain and swelling, prevent stiffness, and initiate early healing.
- Immobilization: The arm is typically placed in a sling, often with an abduction pillow, for 4-6 weeks. The abduction pillow helps offload tension on the supraspinatus repair.
- Pain Management: Analgesics, anti-inflammatory medications, and cryotherapy are used.
- Early Passive Range of Motion (PROM):
- Initiate gentle pendulum exercises as tolerated, usually within the first week.
- Supervised PROM exercises, avoiding active muscle contraction, within protected ranges:
- Forward flexion to 90-120 degrees.
- External rotation to 0-30 degrees (avoiding excessive external rotation that stresses the infraspinatus).
- Internal rotation to the chest.
- Avoid active external rotation and resisted internal rotation for the first 6 weeks to protect the repaired infraspinatus and teres minor.
- Activities of daily living (ADLs) with the affected arm are restricted, emphasizing protection.
- Elbow, Wrist, Hand: Active range of motion exercises for the elbow, wrist, and hand are encouraged immediately to prevent stiffness and maintain circulation.
Phase 2: Active Motion and Early Strengthening (6-12 weeks)
- Goal: Gradually restore active range of motion, begin strengthening, and improve neuromuscular control.
- Discontinue Sling: The sling is typically discontinued around 6 weeks, depending on clinical and radiographic signs of healing.
- Active Range of Motion (AROM):
- Initiate gentle active-assisted range of motion (AAROM) and then AROM exercises, progressing gradually as pain allows.
- Focus on achieving full pain-free forward flexion, abduction, and internal/external rotation.
- Isometrics: Introduce gentle isometric rotator cuff strengthening exercises at various angles, ensuring no pain.
- Scapular Stabilization: Begin exercises to strengthen scapular stabilizers (e.g., serratus anterior, rhomboids, trapezius).
- Proprioception: Initiate light proprioceptive exercises (e.g., wall slides, gentle ball squeezes).
- Restrictions: Continue to avoid heavy lifting, pushing, pulling, and overhead activities. No resistance training against significant loads.
Phase 3: Advanced Strengthening and Functional Return (12-24 weeks)
- Goal: Restore full strength, endurance, and prepare for return to advanced activities or sports.
- Progressive Resistance Exercises:
- Advance rotator cuff strengthening with light weights, resistance bands, or pulleys (e.g., internal/external rotation, abduction, forward flexion).
- Progress strengthening for major shoulder girdle muscles (deltoid, pectoralis, latissimus).
- Focus on eccentric and concentric training.
- Full Range of Motion: The patient should aim to achieve and maintain full, pain-free range of motion.
- Functional Training: Incorporate sport-specific or work-specific activities with gradually increasing intensity and resistance.
- Plyometrics: For athletes, introduce plyometric exercises as appropriate towards the end of this phase.
- Restrictions: Avoid aggressive, uncontrolled, or high-impact activities. Ensure adequate rest and recovery.
Phase 4: Return to Sport/Activity (After 24 weeks)
- Goal: Gradual and safe return to full activity, including overhead sports or heavy manual labor.
- Criteria for Return:
- Full pain-free range of motion.
- Sufficient strength (typically 80-90% of the contralateral side, measured isokinetically if available).
- No signs of impingement or instability.
- Physician and therapist approval.
- Gradual Progression: Return to activity should be gradual, with close monitoring for symptoms.
- Maintenance Program: Continue a home exercise program to maintain strength, flexibility, and prevent recurrence.
Progression through these phases is guided by pain, healing status, and the individual patient's response. Close communication between the surgeon, physical therapist, and patient is essential. Radiographic assessment may be performed at regular intervals to monitor fracture healing.
Summary of Key Literature and Guidelines
The management of displaced greater tuberosity fractures has evolved, with a consensus favoring operative intervention for significant displacement to prevent impingement and restore function. The existing literature, while varied in study design, largely supports anatomical reduction and stable internal fixation.
Displacement Criteria
The 5 mm displacement threshold for operative intervention stems from several anatomical and clinical studies. Flatow et al. (1991) and other anatomical investigations have demonstrated that superior displacement of the greater tuberosity by as little as 5 mm can lead to mechanical abutment against the coraco-acromial arch during shoulder elevation. Clinical series have corroborated these findings, showing higher rates of impingement symptoms and poorer functional outcomes with non-operative management of fractures exceeding this threshold. Further, posterior displacement of the GT fragment greater than 3 mm or angulation greater than 45 degrees can also be critical due to its impact on external rotation and posterior impingement.
Fixation Modalities
Literature comparing different ORIF techniques for greater tuberosity fractures highlights the effectiveness of both suture-based and screw-based methods.
- Suture Fixation: Studies often report good to excellent outcomes with transosseous suture repair or suture anchor constructs. This method is praised for its biological nature, minimal hardware prominence, and ability to reconstruct the rotator cuff footprint. Biomechanical studies suggest that suture bridge techniques provide strong, anatomically favorable fixation, particularly in osteoporotic bone. Authors like Park et al. (2014) demonstrated excellent functional outcomes using suture anchor fixation for greater tuberosity fractures.
- Screw Fixation: Cannulated lag screws and headless compression screws are also widely used. They provide rigid fixation and good interfragmentary compression. However, concern regarding hardware prominence and subsequent impingement or irritation remains. Yoo et al. (2010) reported favorable results with screw fixation but emphasized precise placement to avoid intra-articular violation or subacromial prominence. The choice between headless versus standard cannulated screws often depends on fragment size, bone quality, and surgeon experience, with headless screws generally preferred to minimize hardware-related issues.
- Plate Fixation: While not typically the primary method for isolated GT fractures, small fragment plates or specific greater tuberosity plates can be used in comminuted cases or as part of more complex proximal humeral fracture constructs. Their role in isolated GT fractures is generally limited to adjunctive stabilization.
Outcomes and Complications
Overall, ORIF for displaced greater tuberosity fractures generally yields good to excellent clinical outcomes, with reported rates of successful union exceeding 90%. Key to preventing adverse outcomes is meticulous anatomical reduction. Malunion, particularly superior or posterior displacement, remains the most frequent cause of persistent pain and functional impairment, often necessitating revision surgery for decompression or osteotomy. Hardware prominence, stiffness, and rotator cuff retear are other notable complications, with rates varying depending on the study and fixation method.
The consensus from the literature supports that anatomical reduction and stable internal fixation, whether with sutures or screws, are paramount to restoring glenohumeral kinematics, preserving rotator cuff function, and ultimately preventing subacromial impingement. Early, controlled rehabilitation protocols are also critical for maximizing range of motion and strength while protecting the repair. Adherence to these principles, informed by sound anatomical and biomechanical understanding, underpins the successful management of these challenging injuries.
Clinical & Radiographic Imaging
You Might Also Like


