Operative Management of Flexor and Peroneal Tendon Injuries
Key Takeaway
Flexor hallucis longus (FHL) tendinitis and peroneal tendon tears present complex challenges in foot and ankle surgery. Often seen in athletes, these pathologies require precise clinical differentiation from posterior impingement syndromes. Surgical management ranges from FHL sheath decompression to complex peroneal tendon tubularization and tenodesis. This guide details the evidence-based diagnostic protocols, biomechanical considerations, and step-by-step surgical techniques necessary for optimal functional restoration.
INJURIES OF THE FLEXOR AND PERONEAL TENDONS
Injuries to the flexor tendons of the foot and ankle, while historically considered less common than disorders of the posterior tibial and peroneal tendons, are increasingly recognized as significant sources of hindfoot and midfoot morbidity. The intricate biomechanical interplay of the hindfoot requires a high index of suspicion to accurately diagnose and treat these pathologies. This masterclass details the pathoanatomy, clinical evaluation, and operative management of Flexor Hallucis Longus (FHL) tendinitis, posterior impingement syndromes, and complex peroneal tendon tears requiring reconstruction.
FLEXOR HALLUCIS LONGUS TENDINITIS AND IMPINGEMENT
Pathoanatomy and Biomechanics
The flexor hallucis longus (FHL) muscle originates from the posterior aspect of the fibula and interosseous membrane. Its tendon courses distally through a critical fibro-osseous tunnel located between the medial and lateral tubercles of the posterior talus, passing beneath the sustentaculum tali, and crossing dorsal to the flexor digitorum longus (FDL) at the knot of Henry before inserting at the base of the distal phalanx of the hallux.
FHL tendinitis has classically been described as "dancer’s tendinitis," occurring primarily in ballet dancers and athletes whose disciplines demand repetitive forefoot push-off and extreme plantar flexion (en pointe positioning). However, contemporary literature suggests that FHL tendinopathy is not exclusive to athletes and must be a primary differential diagnosis for any patient presenting with posteromedial ankle pain. The repetitive excursion of the tendon through its constrained fibro-osseous sheath leads to mechanical tenosynovitis, nodule formation, and eventual stenosis, severely limiting tendon glide.
Clinical Presentation and Diagnosis
Michelson and Dunn’s landmark evaluation of 81 patients with FHL pathological processes highlighted the varied clinical presentations of this disorder.
- Primary Symptoms: The most common presenting symptom is activity-related pain, specifically posterior ankle pain (reported in 50% of patients). Heel pain and midfoot pain are also prevalent, reported in 28% and 27% of cases, respectively.
- Palpation: Tenderness is typically elicited at the musculotendinous junction posterior to the medial malleolus (approximately 60% of cases) or distally where the FHL crosses the FDL at the knot of Henry (approximately 40%).
- The FHL Stretch Test: Restriction of FHL excursion is a hallmark sign, demonstrated in 37% of patients. This is clinically evaluated by assessing first metatarsophalangeal (MTP) joint dorsiflexion. A positive test occurs when first MTP dorsiflexion is significantly limited or painful while the ankle is held in maximal dorsiflexion, compared to when the ankle is plantarflexed.
Clinical Pearl: FHL tendinitis is frequently misdiagnosed as posterior tibial tendinitis. Careful palpation posterior to the medial malleolus, combined with a positive FHL stretch test, is critical for differentiation.
Differentiating Posterior Compression Syndrome
On physical examination, meticulous differentiation must be made between FHL tendinitis, compression tendinopathy with stenosis of the FHL sheath, and posterior ankle compression syndrome (posterior impingement).
Posterior impingement typically involves an elongated posterolateral talar process (Stieda process) or an enlarged os trigonum.
* Provocative Testing: Reproduction of deep posterior pain with forced, passive ankle plantar flexion strongly suggests posterior ankle compression syndrome rather than isolated FHL tendinitis.
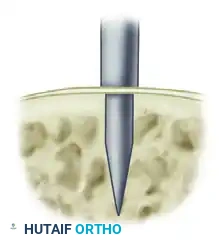
* Diagnostic Injection: The diagnosis of posterior compression syndrome is definitively confirmed by injecting a local anesthetic (e.g., 1% lidocaine) through a posterolateral approach directly into the region of the posterior process of the talus/calcaneus. Complete relief of pain upon forced plantar flexion confirms the osseous impingement.
Imaging Modalities
- Radiographs: Plain lateral standing radiographs are essential. In Michelson and Dunn's series, 70% of radiographs were normal, 14% demonstrated an os trigonum, and 8% showed mild degenerative changes in the first MTP joint. Radiographs are highly effective in differentiating a painful os trigonum from isolated soft-tissue FHL tendinitis.
- Bone Scan (Scintigraphy): Occasionally utilized to differentiate an acute fracture of the trigonal process or a highly symptomatic os trigonum (which will show focal uptake) from tendinopathy.
- Magnetic Resonance Imaging (MRI): MRI is the gold standard for soft tissue evaluation. Approximately 82% of MR images in symptomatic patients demonstrate tenosynovitis (fluid surrounding the FHL tendon) and occasionally reveal intratendinous degenerative changes, partial tears, or nodular thickening.
Conservative Management
Initial management should always be nonoperative, consisting of:
1. Strict rest and immobilization (CAM boot or short-leg cast).
2. Modification of dance technique or offending sporting activities.
3. Aggressive physical therapy focusing on FHL stretching programs.
4. Oral nonsteroidal anti-inflammatory drugs (NSAIDs).
5. Judicious use of localized corticosteroid injections (avoiding intratendinous injection to prevent rupture).
While some authors report high failure rates with conservative care, structured stretching programs combined with short-term immobilization have yielded successful outcomes in up to 64% of patients.
Operative Treatment: FHL Decompression
Operative intervention is indicated for patients who fail 3 to 6 months of conservative management. Surgical decompression and synovectomy yield good to excellent results in 82% to 100% of patients.
Surgical Approaches (Hamilton et al.):
* Medial Approach: Recommended when both FHL tendinitis and posterior osseous impingement are present. This allows for direct visualization and release of the FHL retinaculum, thorough synovectomy, and excision of a prominent posterior talar process if necessary.
* Lateral Approach: Strictly utilized for the treatment of isolated posterior impingement (os trigonum excision) without concurrent FHL tendinopathy.
PERONEAL TENDON REPAIR AND RECONSTRUCTION
While FHL injuries dominate the medial and deep posterior ankle, peroneal tendon injuries are the primary flexor/evertor pathologies of the lateral hindfoot. The peroneus brevis (PB) and peroneus longus (PL) tendons share a common synovial sheath behind the lateral malleolus, constrained by the superior peroneal retinaculum (SPR).
Longitudinal split tears of the peroneus brevis are common, often resulting from mechanical attrition as the tendon is compressed between the fibula and the overlying peroneus longus tendon during repetitive dorsiflexion and eversion.
Indications for Surgery
Surgical exploration and repair are indicated for symptomatic peroneal tendon tears, subluxation, or severe tendinosis that has failed conservative management (immobilization, physical therapy, bracing).
Surgical Warning: Preoperative MRI is highly sensitive for fluid in the peroneal sheath but may underestimate the longitudinal extent of a peroneus brevis split tear. The surgeon must be prepared for extensive debridement, tubularization, or tenodesis based on intraoperative findings.
🔪 Surgical Technique: Peroneal Tendon Reconstruction
Step 1: Positioning and Exposure
The patient is placed in the lateral decubitus position with a beanbag, ensuring the operative leg is uppermost. A well-padded thigh tourniquet is applied.
A longitudinal incision is made along the posterior ridge of the fibula, extending distally toward the base of the fifth metatarsal, following the course of the peroneal tendons. Care is taken to identify and protect the sural nerve, which crosses the operative field distally.
The subcutaneous tissues are sharply dissected to expose the superior peroneal retinaculum (SPR). The SPR is carefully incised longitudinally, leaving a small cuff of tissue attached to the fibula for later repair.
Step 2: Tendon Assessment and Debridement
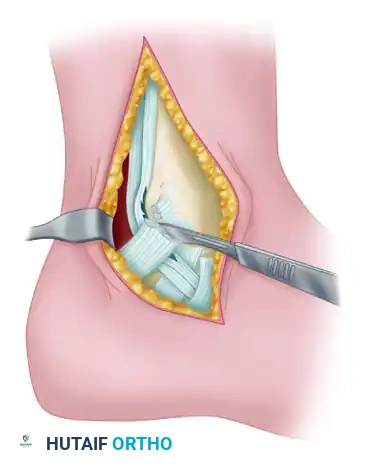
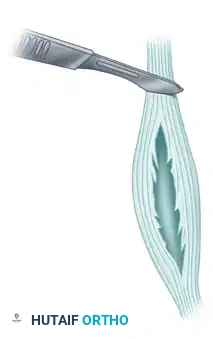
Once the retinaculum is opened, the peroneal tendons are luxated from the retromalleolar groove and inspected. The peroneus brevis is flattened and closely applied to the fibula, making it highly susceptible to longitudinal split tears with fraying.
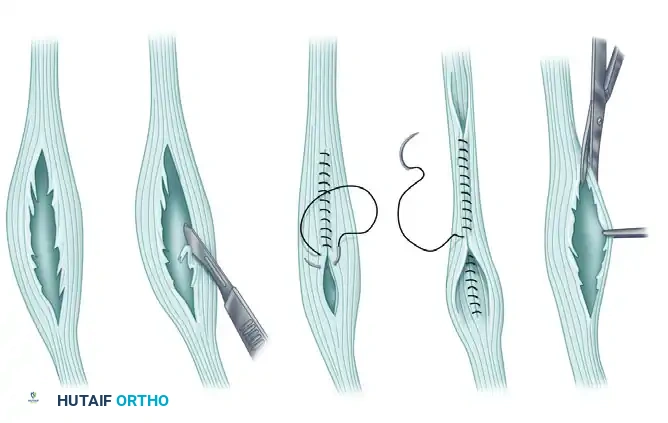
If the peroneus brevis split involves less than 50% of the tendon's cross-sectional area, the degenerative margins of the split are meticulously debrided.
Following debridement, the remaining healthy tendon edges are sutured together using a running, locking non-absorbable suture (e.g., 2-0 FiberWire or Prolene) to tubularize the tendon. This restores the tendon's cylindrical architecture, allowing it to glide smoothly within the retromalleolar groove. Alternatively, if the split is very anterior and superficial within the tendon, the degenerative flap can simply be excised without formal tubularization.
Step 3: Tenodesis for Severe Degeneration
If the peroneus brevis is severely degenerated, flattened, and comprises less than 50% viable tendinous tissue, primary repair and tubularization will fail. In these advanced cases, the diseased segment of the peroneus brevis must be completely resected.
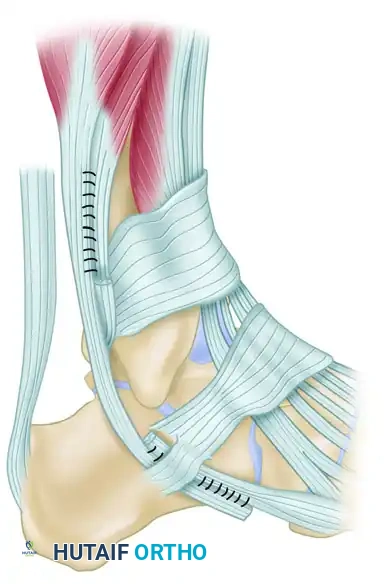
The remaining healthy proximal and distal stumps of the peroneus brevis are then tenodesed (sutured) directly to the adjacent, intact peroneus longus tendon. This side-to-side tenodesis is performed using a robust Krackow or Pulvertaft weave technique with heavy non-absorbable sutures, ensuring appropriate resting tension is maintained to preserve eversion strength.
Step 4: Retromalleolar Groove Deepening (Optional but Recommended)
Before repairing the retinaculum, the posterior fibular groove is palpated. If the groove is shallow or convex, a fibular groove deepening procedure is performed. A cortical flap is elevated, the underlying cancellous bone is impacted or curetted, and the cortical flap is tamped back into place, creating a deep, concave sulcus for the tendons.
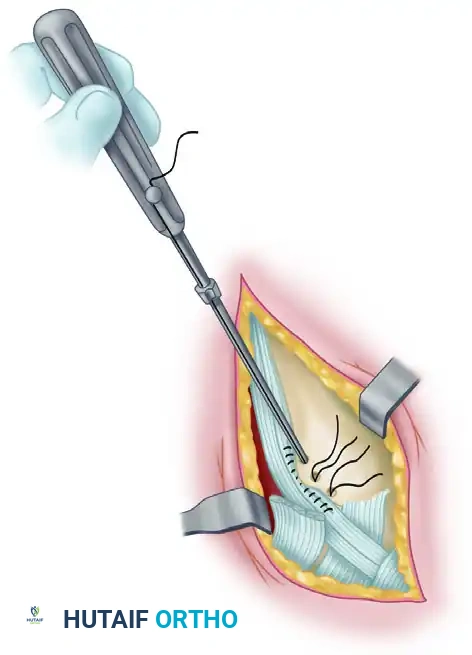
Step 5: Superior Peroneal Retinaculum Repair
The final, critical step is the robust repair of the superior peroneal retinaculum to prevent postoperative tendon subluxation. If the native tissue is attenuated or pulled off the fibular ridge, suture anchors are utilized to secure the SPR directly to the bone.

A drill guide is used to prepare the pilot holes along the posterolateral ridge of the fibula.

Small-diameter (e.g., 2.5mm or 3.0mm) titanium or biocomposite suture anchors are selected for the repair.
The anchors are inserted into the prepared fibular holes. Care must be taken to angle the drill and anchors slightly anteriorly to avoid penetrating the articular surface of the distal tibiofibular syndesmosis or the ankle joint.
The sutures from the anchors are passed through the edge of the superior peroneal retinaculum. The tendons are reduced into the groove, the ankle is held in slight eversion and plantar flexion, and the sutures are tied, securely imbricating the retinaculum over the tendons. The stability of the tendons is dynamically tested by taking the ankle through a full range of motion.
Postoperative Protocol
- Phase I (0-2 Weeks): The patient is placed in a non-weight-bearing short leg splint with the ankle in slight plantar flexion and eversion to remove tension from the repaired retinaculum and tendons.
- Phase II (2-6 Weeks): Sutures are removed at 2 weeks. The patient is transitioned to a controlled ankle motion (CAM) boot. Weight-bearing is gradually advanced. Gentle active range of motion (dorsiflexion and plantar flexion) is initiated, but active eversion and passive inversion are strictly avoided to protect the repair.
- Phase III (6-12 Weeks): The CAM boot is weaned. Formal physical therapy begins, focusing on peroneal strengthening, proprioception, and progressive resistance exercises.
- Phase IV (3-6 Months): Return to sport-specific activities and high-impact loading is permitted once symmetric strength and pain-free range of motion are achieved, typically around 4 to 6 months postoperatively.
You Might Also Like


