Muscle Hernias & Peroneal Tendon Displacement: Surgical Guide
Key Takeaway
Muscle herniation and peroneal tendon displacement present unique challenges in orthopedic surgery. While asymptomatic muscle hernias require conservative management, symptomatic peroneal tendon instability often necessitates surgical intervention. This guide details the pathophysiology, clinical evaluation, and step-by-step operative techniques—including superior peroneal retinaculum reconstruction, fibular groove deepening, and bone block procedures—to restore lateral ankle stability and prevent chronic dysfunction.
HERNIAS OF THE MUSCLES
Herniation of muscle tissue through a defect in the overlying fascial sheath is a relatively rare clinical entity, predominantly occurring in the lower extremity below the knee. These hernias vary significantly in size; while some present as large, palpable masses, the vast majority are 1 cm or less in diameter.
Pathophysiology and Etiology
The etiology of muscle herniation is broadly categorized into traumatic and constitutional/exertional causes. Occasionally, a direct blow to the extremity ruptures the fascial sheath, creating an acute defect. More frequently, however, no definitive relationship exists between a single traumatic event and the development of the hernia.
Excessive physical activity is the primary driver for small muscle hernias. They are most frequently observed among mountain climbers, skiers, foot soldiers, and elite athletes. The pathophysiological cascade involves exercise-induced muscle hypertrophy, which distends the rigid fascial compartment. Over time, the fascial sheath becomes attenuated, weak, and ultimately splits. Small herniations often exploit pre-existing anatomical weak points in the fascial sheath, particularly the rings through which small perforating arteries, veins, and cutaneous nerves emerge.
In the lower leg, muscle hernias are most common over the anterior compartment (tibialis anterior muscle) and slightly less common over the lateral compartment (peroneal muscles). The fascial defect is typically oval, featuring sharp, well-defined edges, while the underlying muscle tissue remains histologically normal and unthickened.
Conversely, large hernias occur more frequently in the thigh, usually in the anterolateral aspect. These are almost exclusively iatrogenic or traumatic, caused by a direct high-energy blow or the surgical harvesting of the fascia lata.
Clinical Evaluation and Imaging
The clinical presentation of muscle hernias depends heavily on their size and location:
* Large Hernias (Thigh): These are generally non-reducible. They become less prominent with recumbency and muscle relaxation, but paradoxically become more prominent and bulge outward when the underlying muscle is actively contracted.
* Small Hernias (Below the Knee): These are frequently multiple and often bilateral. They are usually reducible. Unlike large hernias, small hernias typically decrease in size or completely disappear when the muscle contracts, as the fascial defect tightens and the muscle belly elongates.
Diagnosis is primarily clinical, though multiple small hernias are occasionally misdiagnosed as varicose veins, lipomas, or angiomas.
Advanced imaging has revolutionized the evaluation of these lesions. Hereditary hernias of the peroneus longus have been well-documented using MRI. Furthermore, dynamic sonographic examination (ultrasound) is highly efficacious. Sonography allows for real-time, dynamic evaluation of the muscle herniation during active contraction and relaxation, clearly demonstrating the reduction and displacement of the muscle tissue through the fascial defect.
Management Strategies
Treatment is strictly reserved for patients whose symptoms are severe, localized, and functionally disabling. Most patients complain only of mild, generalized aching, increased fatigability, and pain upon strenuous activity.
Conservative Management:
If symptoms are mild, the first line of treatment includes the restriction of offending physical activities and the application of graduated elastic compression supports (e.g., compression stockings).
Operative Management:
Surgical intervention requires meticulous planning due to the risk of iatrogenic complications.
🚨 SURGICAL WARNING: Compartment Syndrome Risk
Primary side-to-side closure of fascial defects over the anterior aspect of the leg is strictly contraindicated. Attempting to pull the fascial edges together decreases the overall volume of the anterior compartment. This can precipitate acute, exercise-induced anterior tibial compartment syndrome.
Symptomatic small hernias should not be repaired primarily. Instead, the surgical approach should involve enlarging the defect via a longitudinal fasciotomy extending proximally and distally to decompress the compartment.
Alternative reconstructive techniques for larger, highly symptomatic defects include:
* Covering the defect with a fascial, periosteal, or dermal autograft.
* Partial excision of the protruding muscle belly (rarely indicated).
* Synthetic patch repair: Successful treatment of anterior tibial muscle hernias has been reported using Mersilene mesh to bridge the defect without compromising compartment volume.
DISPLACEMENT OF TENDONS: PERONEAL TENDONS
Afflictions of the peroneal tendons are among the most common, yet frequently overlooked, causes of chronic lateral ankle pain and instability. The spectrum of pathology includes tendinitis, stenosing peroneal tenosynovitis, tendon rupture, and subluxation or frank dislocation of the tendons from the retromalleolar peroneal groove.
Peroneal Tendinitis and Rupture
Peroneal tendinitis typically responds well to conservative measures, including relative rest, ice massage, and nonsteroidal anti-inflammatory drugs (NSAIDs). Stenosing peroneal tenosynovitis, however, may clinically mimic lateral ankle ligamentous instability. Tenography or MRI is highly beneficial in establishing the diagnosis. Operative decompression via partial excision of the roof of the peroneus brevis tendon sheath distal to the lateral malleolus usually provides excellent pain relief.
The peroneus brevis and longus tendons may rupture singly or in combination.
* Clinical Signs of Rupture: Swelling and point tenderness along the course of the tendon.
* Radiographic Signs: Proximal migration of the os peroneum (a sesamoid bone within the peroneus longus tendon) from its normal anatomical footprint at the cuboid tunnel is pathognomonic for a peroneus longus rupture.
Surgical Repair of Ruptures:
Rupture of the peroneus longus tendon can be addressed via tenodesis. The distal aspect of its musculotendinous junction is sutured to the proximal aspect of the intact peroneus brevis tendon (Thompson and Patterson technique). However, outcomes can be mixed; studies indicate that fewer than half of patients return to competitive sports without residual symptoms, with many experiencing chronic scar tenderness and lateral ankle swelling.
Peroneal Tendon Subluxation and Dislocation
The peroneal tendons may displace within their sheaths, but more commonly, they dislocate entirely outside the sheath and the fibular groove. This occurs when the peroneal musculature contracts violently, overpowering the stabilizing soft tissues (primarily the superior peroneal retinaculum, SPR), causing the tendons to dislocate anteriorly over the distal fibula.
Mechanism of Injury:
The classic mechanism is forced dorsiflexion of the ankle combined with a maximal, sudden peroneal contraction. This is frequently seen in skiing during a forward fall. Other authors attribute the injury to a sudden plantarflexion-eversion stress.
Clinical Diagnosis:
* Patients report a painful "popping" or "clicking" sensation at the lateral ankle, particularly when ascending stairs.
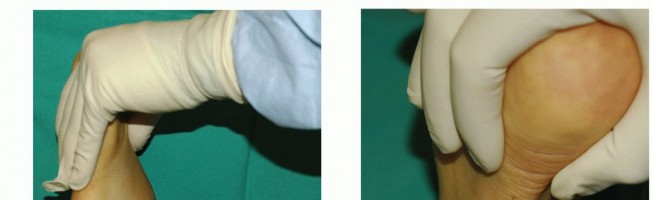
* Provocative Testing: The examiner places the patient's foot in dorsiflexion, eversion, and external rotation. The patient is asked to resist an inversion-plantarflexion force applied by the examiner.
* Dislocation can often be palpated directly by placing a finger over the anterior tip of the peroneal groove during active circumduction of the foot.
If missed in the acute setting, this injury rapidly evolves into a chronic, highly disabling condition.
Management of Peroneal Displacement
Acute Injuries:
Acute avulsions of the superior peroneal retinaculum should be repaired primarily. Postoperatively, the patient is placed in a non-weight-bearing short leg cast for 4 weeks, followed by a weight-bearing cast or boot for an additional 2 to 3 weeks before initiating progressive range-of-motion (ROM) and strengthening protocols.
Chronic/Recurrent Injuries:
Symptomatic chronic or recurrent tendon dislocation necessitates surgical reconstruction. Anatomical predisposing factors must be evaluated preoperatively, including:
1. Incompetence or attenuation of the superior peroneal retinaculum.
2. A shallow or absent fibular retromalleolar sulcus.
3. A convex posterior surface of the distal fibula.
Operative procedures fall into five major categories:
1. Periosteal Attachment / Soft-Tissue Reconstruction: Utilizing local fascia or periosteum to recreate the SPR.
2. Groove Deepening: Excavating the fibula to create a deeper bony trough.
3. Tenoplasty: Using tendon slips (e.g., Achilles) to create a stabilizing sling.
4. Bone Block Procedures: Osteotomies to create a physical bony barrier against anterior translation.
5. Rerouting Procedures: Incising the calcaneofibular ligament (CFL) and routing the tendons deep to it.
SURGICAL TECHNIQUES FOR PERONEAL TENDON DISPLACEMENT
Soft-Tissue Reconstruction (Technique 46-30)
This technique utilizes local deep fascia to reconstruct an incompetent superior peroneal retinaculum.
- Positioning & Incision: Place the patient in the lateral decubitus position. Make a longitudinal incision over the posterior aspect of the distal third of the fibula, extending it distally over the lateral border of the foot toward the cuboid.
- Flap Creation: At the level of the lateral malleolus, elevate the posterior skin flap superficially. From the underlying deep fascia, dissect an ample fascial flap, leaving its base firmly attached to the tip of the lateral malleolus.
- Tendon Retraction: Carefully incise the remaining tendon sheaths and retract the peroneal tendons anteriorly.
- Groove Preparation: Using a sharp osteotome or high-speed burr, create or deepen the groove in the posterior aspect of the lateral malleolus. Seat the peroneal tendons comfortably within this new sulcus.
- Flap Fixation: Bring the mobilized fascial flap posteriorly over the tendons. Suture it securely to the remnants of the retinacula, the local periosteum, or the soft tissue on the lateral aspect of the calcaneus to act as a robust restraining sling.
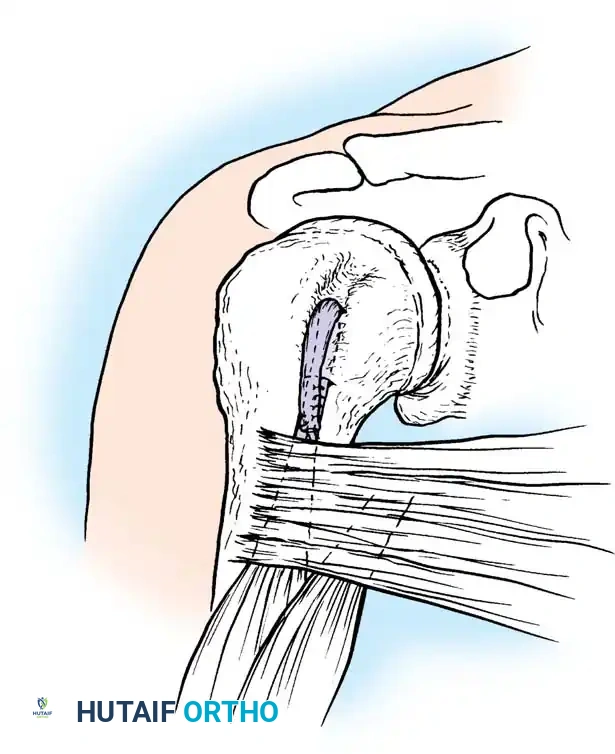
Fibular Groove Deepening (Technique 46-31: Zoellner & Clancy)
This is the gold-standard procedure for patients with a shallow or convex fibular groove. It deepens the sulcus while preserving the smooth cortical gliding surface for the tendons.
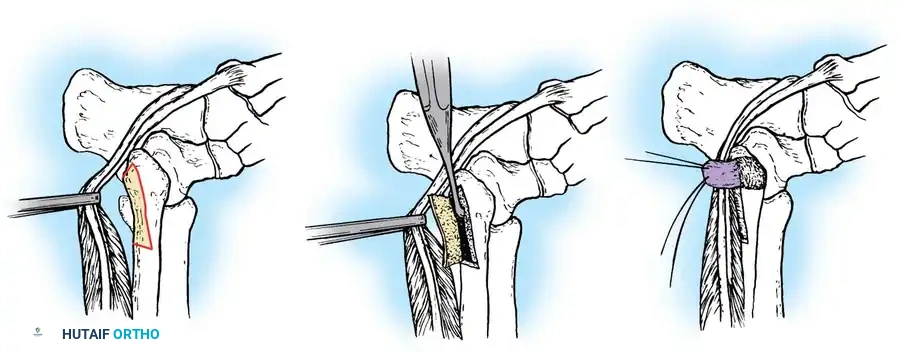
Fig. 46-38 Technique for recurrent dislocation of peroneal tendon. A, With tendons retracted, cortical osteoperiosteal flap is raised along posterolateral aspect of distal fibula, leaving posteromedial border intact as hinge. B, Flap is hinged posteriorly, and cancellous bone is removed from posterior aspect of fibula to deepen groove. C, Periosteal flap is swung posteriorly over tendons in groove.
🔪 Surgical Steps:
* Make a 7-cm J-shaped curvilinear incision posterior to the lateral malleolus, following the anatomical course of the peroneal tendons.
* Free the tendons from their sheath and retract them anteriorly over the malleolus to expose the retromalleolar groove.
* Using a sharp osteotome, raise a cortical osteoperiosteal flap measuring approximately 3 cm × 1 cm along the posteromedial aspect of the distal fibula and lateral malleolus. Crucial Step: Leave the posteromedial border intact to act as a living hinge (Fig. 46-38A).
* Gently swing the cortical flap posteriorly on its hinge. Using a curette or burr, remove the underlying cancellous bone from the posterior aspect of the fibula to deepen the bed by 6 to 9 mm (Fig. 46-38B).
* Tamp the cortical flap back into its original position. This creates a deepened groove 3 to 4 cm long. The floor of the groove now provides a smooth, anatomical cortical gliding surface for the tendons.
* Replace the peroneal tendons into the newly deepened groove. Take the ankle through a full, dynamic range of motion (dorsiflexion and eversion) to ensure the tendons remain well-seated without any tendency to subluxate.
* If the native superior peroneal retinaculum is robust, plicate it over the tendons. If it is tenuous, raise an additional 1 cm square periosteal flap from the lateral surface of the malleolus (hinged posterolaterally), reflect it posteriorly, and suture it to the medial part of the retinaculum (Fig. 46-38C).
* Close the wounds in layers and apply a short leg cast.
Postoperative Protocol:
The foot is immobilized in a cast in slight eversion and neutral dorsiflexion (90 degrees) for 3 weeks. At 3 weeks, transition to a hinged short leg cast or CAM boot that allows controlled dorsiflexion and plantarflexion exercises for an additional 3 weeks. Strenuous athletics are withheld until full ROM and symmetrical strength are achieved (typically 3-4 months).
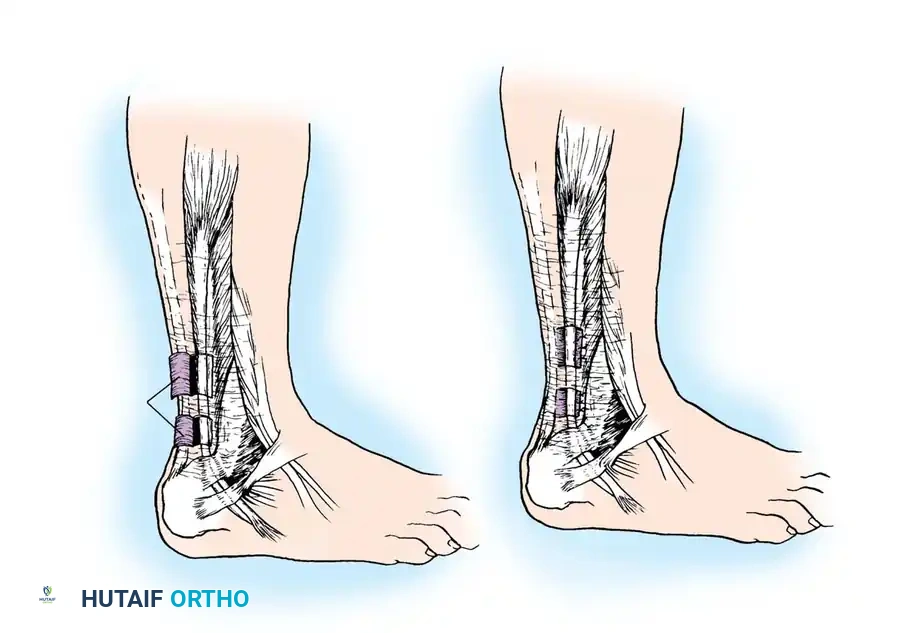
Tenoplasty: Achilles Tendon Flap (Jones Technique 46-32)
When local tissue is insufficient, a slip of the Achilles tendon can be utilized to create a robust restraining ligament.
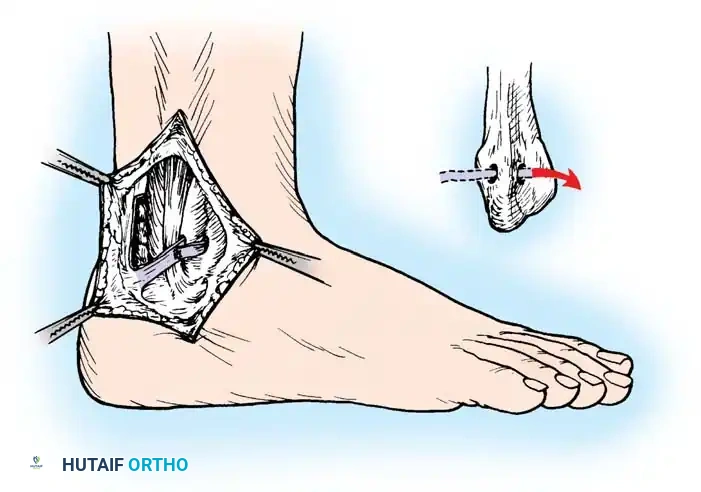
Fig. 46-39 Jones technique for displacement of peroneal tendons. Check that ligament formed by flap of Achilles tendon is inserted through hole drilled in lateral malleolus.
🔪 Surgical Steps:
* Make a 5-cm longitudinal incision posterior to the lateral malleolus.
* Without disturbing their sheaths, reduce the peroneal tendons into their normal anatomical position behind the malleolus.
* Expose the lateral border of the Achilles tendon. Dissect a distally based flap measuring 5 cm long by 0.6 cm wide, leaving its distal insertion firmly attached to the calcaneus (Fig. 46-39).
* Expose the lateral malleolus and drill a transverse hole through it in an anteroposterior direction.
* Draw the free proximal end of the Achilles flap through the fibular drill hole from posterior to anterior.
* Tension the flap appropriately over the peroneal tendons, and suture it to itself and the surrounding periosteum to create a secure sling.
Clinical Pearl: While biomechanically sound, some patients experience persistent Achilles tendinitis following this harvest. It is generally reserved for revision cases.
Bone Block Procedures
Bone block procedures create a rigid, physical barrier to prevent anterior tendon translation.
DuVries Technique:
DuVries described a sliding bone wedge osteotomy of the lateral malleolus.
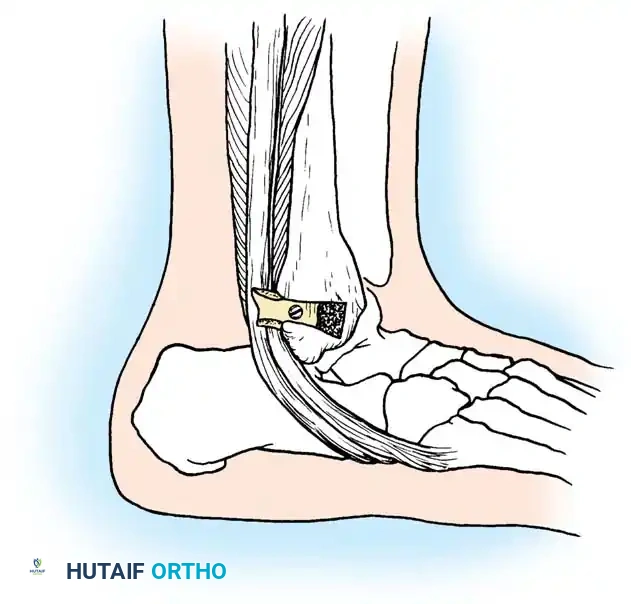
Fig. 46-40 DuVries technique for holding peroneal tendons behind lateral malleolus. A 2-cm wedge of bone is driven backward to act as a buttress.
🔪 Surgical Steps:
* Expose the lateral malleolus.
* Using an oscillating saw, cut a 2-cm wedge of bone from the lateral malleolus (Fig. 46-40).
* Displace the wedge posteriorly by exactly 0.5 cm in its bed so that its posterior edge overhangs the peroneal tendons, creating a bony buttress.
* Secure the wedge in its new displaced position using a small fragment cortical screw.
Micheli, Waters, and Sanders Technique:
This alternative bone block technique utilizes a 3 cm × 5 cm corticocancellous longitudinal graft harvested from the distal fibula. The graft is contoured, translated 1 to 1.5 cm distally, and rigidly fixed with
Associated Surgical & Radiographic Imaging
You Might Also Like