Comprehensive Surgical Management of Anterior Tibial and Peroneal Tendon Disorders

Key Takeaway
Anterior tibial and peroneal tendon disorders require precise surgical management to restore foot and ankle biomechanics. This comprehensive guide details the step-by-step operative techniques for primary repair, autogenous graft reconstruction, and tenodesis. Key procedures include medial cuneiform anchoring for anterior tibial ruptures and the management of peroneal tendinopathy, subluxation, and tears. Strict adherence to postoperative immobilization protocols ensures optimal graft incorporation and functional recovery.
BIOMECHANICS AND CLINICAL SIGNIFICANCE OF ANKLE TENDON DISORDERS
The dynamic stability and functional biomechanics of the foot and ankle rely heavily on the integrity of the extrinsic musculotendinous units. The anterior tibial tendon serves as the primary dorsiflexor of the ankle and invertor of the midfoot, accounting for over 80% of dorsiflexion power. Conversely, the peroneal tendons (longus and brevis) are the primary evertors of the foot, playing a critical role in stabilizing the first ray during the stance phase of gait and preventing excessive inversion.
Pathologies affecting these tendons—ranging from acute traumatic ruptures to chronic attritional tendinopathy and stenosing tenosynovitis—can severely compromise gait mechanics, leading to secondary deformities such as a varus hindfoot or progressive arch collapse. This comprehensive academic guide delineates the evidence-based surgical protocols for the débridement, primary repair, and autogenous reconstruction of the anterior tibial tendon, as well as the systematic management of peroneal tendon disorders.
DÉBRIDEMENT AND REPAIR OF THE DISTAL ANTERIOR TIBIAL TENDON
Rupture of the anterior tibial tendon is a relatively uncommon clinical entity, typically occurring in patients over the age of 50 due to chronic attritional degeneration, or in younger patients following a forced plantarflexion injury against a maximally contracted dorsiflexor. Prompt surgical intervention is indicated to restore dorsiflexion power, prevent foot drop, and mitigate the development of secondary equinus contractures.
Surgical Approach and Tendon Mobilization
The surgical approach for the débridement and repair of the anterior tibial tendon utilizes an anteromedial incision, identical to the approach used for an ankle synovectomy.
- Incision and Exposure: Make a longitudinal incision over the course of the anterior tibial tendon, extending from the distal tibia to the medial cuneiform.
- Retinaculum Management: If the tendon is ruptured beneath the inferomedial limb of the inferior extensor retinaculum, carefully incise this fibrous band. It is critical to preserve as much of the retinaculum as possible to prevent postoperative bowstringing.
- Tendon Advancement: Mobilize the proximal stump of the tendon and advance it as far distally as possible. In chronic cases, significant retraction and fibrosis may necessitate extensive proximal release.
Surgical Pearl: If the tendon is ruptured beneath the superomedial limb of the inferior extensor retinaculum, advancement can be challenging. Slowly pass a curved hemostat or a small tendon passer proximally through the tendon sheath to grasp and advance the stump. If this fails, make a secondary 2- to 3-cm anteromedial incision proximal to the ankle joint to identify the tendon at the anteromedial border of the tibia, then pass it distally using a tendon passer or by suturing it to a rubber urinary catheter.
Primary Repair of Complete Rupture
When sufficient tendon length is available after the excision of degenerative tissue, a primary repair to the anatomical footprint on the medial cuneiform is the gold standard.


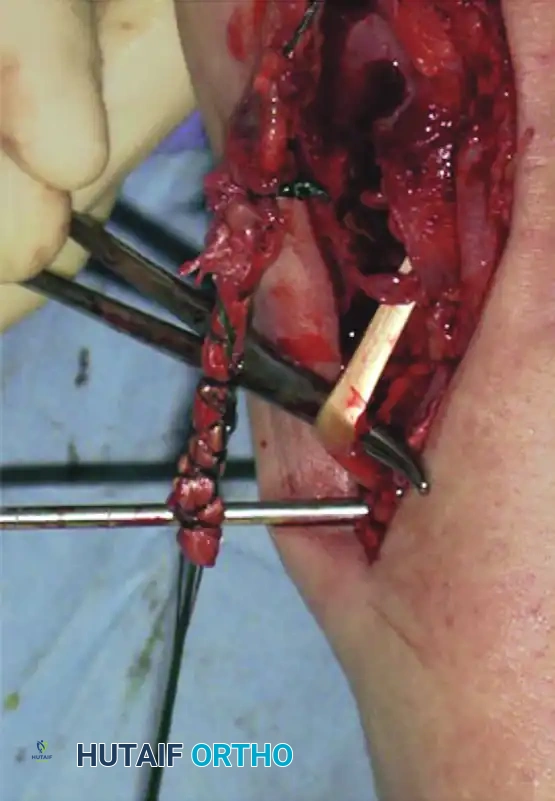
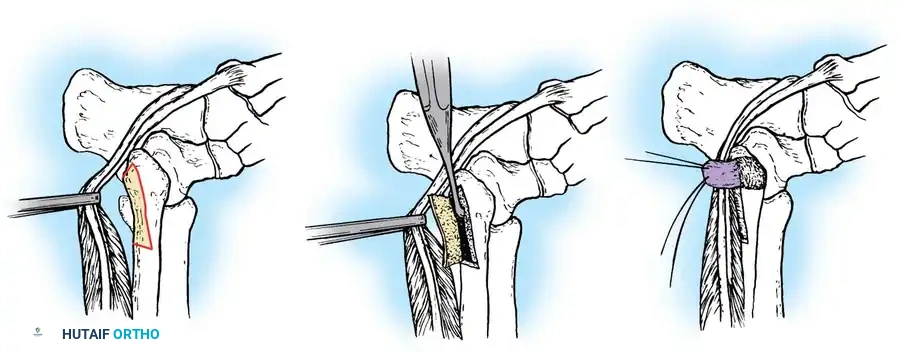
Figure 82-44: Repair of chronic anterior tibial tendon rupture. (A) Ruptured anterior tibial tendon. (B) Extensor hallucis longus tendon identified distally and anastomosed to extensor hallucis brevis before transection. (C) Extensor hallucis longus tunnel passed through a drill hole in the cuneiform. (D) Tendons fixed with suture anchors.
Step-by-Step Fixation Technique:
1. Bone Tunnel Preparation: Drill a hole in the medial cuneiform from dorsal to plantar. Raise the inferior flap and the abductor hallucis muscle plantarward just enough to visualize the drill bit emerging. Incrementally enlarge the bone tunnel to 1/4 inch or 5/16 inch to accommodate the tendon stump.
2. Suture Configuration: Place a Bunnell weave of #0 nonabsorbable suture on free straight needles into the distal end of the proximal tendon stump.
3. Tendon Passage: Pass the tendon through the osseous tunnel. This step is facilitated by passing one end of the suture at a time using the straight needles.
4. Tensioning and Fixation: Pull the tendon firmly into the hole. While holding the ankle in 20 to 30 degrees of maximal dorsiflexion, suture the edge of the tendon to the adjacent periosteum and deep plantar fascia.
5. Alternative Insertion (Navicular): If the tendon is severely retracted and cannot reach the medial cuneiform, the navicular may be used as an alternative bony insertion. Dissect plantarward, staying strictly plantar to the posterior tibial tendon. Retract the abductor hallucis plantarward, remaining cognizant of the long toe flexor tendons laterally. Using a small, free, curved cutting needle (e.g., No. 7 Murphy needle), pass the tendon through the middle of the navicular and suture it under tension to the inferior surface of the bone while the ankle is dorsiflexed.
6. Closure: Bring the abductor hallucis fascia and muscle dorsally back to their anatomical positions and secure them with absorbable sutures. Repair the extensor retinaculum meticulously to prevent bowstringing.
Tendon Reconstruction with Autogenous Graft (Sammarco Technique)
In cases of chronic, neglected ruptures where the tendon ends cannot be approximated or apposed to the insertion site due to massive defects, an interpositional autogenous tendon graft is required to bridge the gap and reinforce the repair.

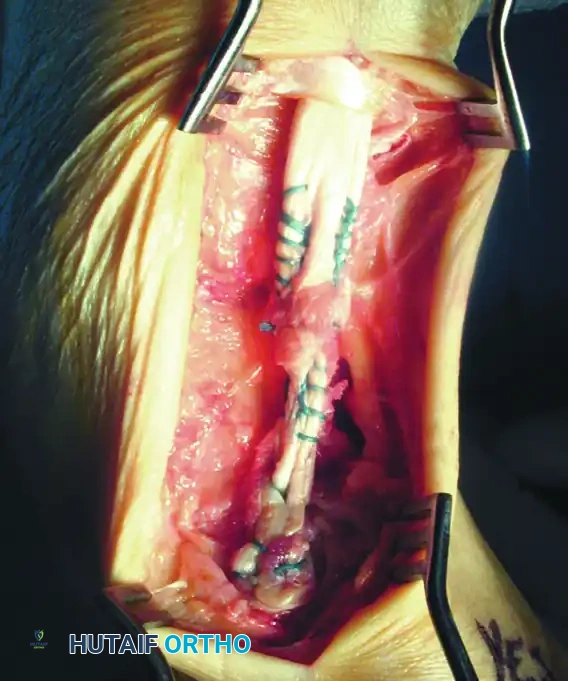
Figure 82-45: Tendon reconstruction with autogenous tendon graft. (A) Remaining portion of the anterior tibial tendon after excision of the degenerated portion and interposed scar tissue. Suture anchors have been placed. (B) Tripled interpositional plantaris tendon graft used to reconstruct the defect.
- Graft Selection: The plantaris tendon is the preferred autograft due to its expendability and adequate length. Alternative sources include the extensor digitorum longus, peroneus tertius, Achilles tendon strips, or a semitendinosus allograft.
- Graft Preparation: If the plantaris is absent and the extensor digitorum or peroneus tertius is utilized, harvest approximately 8 to 10 cm of tendon. Suture the remaining free segment of the distal part of the donor tendon to the intact extensor digitorum communis tendons to preserve toe extension.
- Weaving the Graft: Because these autografts are significantly smaller in diameter than the native anterior tibial tendon, fold the grafts over two or three times (tripling the graft) to achieve a satisfactory biomechanical diameter. Weave the graft between the proximal stump and the distal insertion site, securing it with nonabsorbable sutures under appropriate tension (ankle in dorsiflexion).
Postoperative Care Protocol
Strict adherence to postoperative immobilization is critical for graft incorporation and the prevention of elongation.
- Initial Phase (0-3 Weeks): The patient is placed in a short-leg cast with the ankle locked in 0 degrees of dorsiflexion (neutral). The patient remains strictly non-weight-bearing.
- Intermediate Phase (3-6 Weeks): Weight-bearing in the cast is permitted after 3 weeks for primary repairs. However, patients who underwent an autograft-augmented reconstruction must remain in the cast for a full 6 weeks to protect the graft integration.
- Rehabilitation Phase (6-12 Weeks): Once the cast is removed, the patient transitions to a controlled ankle motion (CAM) boot with a hinged ankle joint. The hinge is set to allow full dorsiflexion but strictly prevents plantar flexion to avoid tensioning the repair. Plantar flexion is gradually increased over the subsequent weeks. The boot is typically discontinued 10 to 12 weeks postoperatively, followed by aggressive physical therapy focusing on eccentric strengthening and proprioception.
DISORDERS OF THE PERONEAL TENDONS
Peroneal tendon disorders are a frequent cause of lateral ankle pain and instability, often misdiagnosed as chronic lateral ankle sprains. The pathology encompasses a spectrum ranging from acute inflammatory tendinitis to chronic stenosing tenosynovitis, subluxation, and attritional ruptures.
Classification of Peroneal Disorders
Disorders of the peroneal tendons are primarily categorized into three distinct clinical entities:
- Primary Peroneal Tendinitis (Without Subluxation): This condition involves inflammation, swelling, and effusion within the peroneal tendon sheath without demonstrable instability on manual examination. It may or may not be accompanied by attritional ruptures. It is relatively rare and predominantly affects middle-aged athletes.
- Peroneal Tendinitis with Instability: This type is characterized by instability of the peroneal tendons at the level of the superior peroneal retinaculum. It is frequently associated with an acute rupture or stripping of the superior peroneal retinaculum, often occurring in younger athletes following acute ankle inversion/dorsiflexion trauma. It is highly correlated with chronic lateral ankle instability.
- Stenosing Tenosynovitis of the Peroneus Longus: This condition is localized to the cuboid tunnel. It is frequently associated with a painful, hypertrophic, or fractured os peroneum, an enlarged peroneal tubercle, or degenerative joint disease at the calcaneocuboid joint. In severe cases, the peroneus longus tendon becomes completely encased in a bony tunnel at the level of the cuboid.
Clinical Pitfall: Patients presenting with stenosing tenosynovitis of the peroneus longus frequently exhibit underlying biomechanical abnormalities, most notably a high arch (cavus foot) or a rigid varus hindfoot. Failure to address the underlying cavovarus deformity will inevitably lead to surgical failure and recurrence of the tendon pathology.
Clinical Diagnosis and Imaging
The diagnosis of peroneal tendinopathy is primarily clinical, supported by targeted advanced imaging.


Figure 82-46: Clinical appearance of peroneal tenosynovitis. Note the prominent swelling and effusion just posterior to the lateral malleolus.
- Physical Examination: Patients typically present with swelling, tenderness, grating, and audible crepitance posterior to the lateral malleolus as the tendons (peroneus longus lateral to the brevis) course beneath the superior peroneal retinaculum. Palpable fluid within the sheath is common.
- Biomechanical Assessment: Evaluation with the patient standing is mandatory to identify hindfoot varus or valgus alignment.
- Strength Testing: Manual testing of eversion strength is necessary. Selective testing of the peroneus longus is performed by asking the patient to actively evert the foot while the examiner pushes upward on the medial column at the level of the first metatarsal head (assessing the longus's ability to plantarflex the first ray).
- Rupture Presentation: Complete or incomplete ruptures may occur at the musculotendinous junction (due to violent eccentric contraction) or within the cuboid tunnel (attritional rupture associated with an os peroneum).


Figure 82-47: (A) A 61-year-old man with a rupture of the peroneus longus tendon and a varus right foot. (B) Note the hypertrophic os peroneum and its proximal migration following the rupture.
Imaging Modalities:
While clinical awareness is paramount, imaging confirms the extent of the pathology.
- Plain Radiographs: Essential for identifying bone avulsions (e.g., "fleck sign" of the superior peroneal retinaculum) or the proximal migration/fracture of an os peroneum.
- MRI and Ultrasound: MRI is the gold standard for evaluating intratendinous tearing, tenosynovitis, and retinacular integrity.



Figure 82-48: (A and B) Radiographs demonstrating a tear of the peroneus longus with proximal retraction of the sesamoid bone (os peroneum). (C) T2-weighted MRI showing a type I tear of both the peroneus longus and peroneus brevis tendons.
Surgical Management of Peroneal Tears
Krause and Brodsky established a widely accepted classification for tears of the peroneus brevis, which dictates the surgical approach:
- Grade I Tears: Longitudinal split tears involving 50% or less of the cross-sectional area of the peroneus brevis tendon.
- Grade II Tears: Severe tears involving more than 50% of the tendon cross-section.
Operative Technique:
1. Tenosynovectomy and Exploration: Through a lateral retromalleolar incision, open the peroneal sheath. The intraoperative findings often reveal a progression from clear fluid and relatively normal tendons to thickened, fibrotic sheaths with grayish, degenerative tendons containing longitudinal split tears.
2. Grade I Repair: For tears involving <50% of the tendon, the degenerative edges of the split are sharply excised (débrided), and the remaining healthy tendon is tubularized using a running locking suture of fine nonabsorbable or slowly absorbing material.
3. Grade II Repair (Tenodesis): If >50% of the tendon is compromised, leaving insufficient viable tissue for tubularization, the diseased segment must be completely excised. The proximal and distal viable limbs of the peroneus brevis are then tenodesed (sutured side-to-side) to the adjacent intact peroneus longus tendon to preserve eversion power.
Treatment Outcomes and Prognosis
Conservative management—comprising cast or CAM boot immobilization, NSAIDs, targeted corticosteroid injections (used with extreme caution to avoid iatrogenic rupture), and orthotic correction of biomechanical faults—can be effective for isolated tendinitis without structural tearing.
However, for patients failing conservative therapy or those with MRI-confirmed significant intratendinous tearing or subluxation, operative débridement, repair, and tenosynovectomy are indicated.
Surgeons must counsel patients appropriately regarding postoperative expectations. A landmark study by Steel and DeOrio evaluating patients at an average 3-year follow-up after operative treatment of peroneal tendon tears revealed sobering statistics: over half of the patients reported residual complaints, including scar tenderness, mild lateral ankle swelling, localized numbness, or shoewear limitations. Only a small fraction (5 out of 26 patients) were able to return to competitive sports with absolutely no limitations, underscoring the severe biomechanical toll of chronic peroneal tendon pathology.
📚 Medical References
- tendon repair: an in vitro biomechanical study of tendon attachment, Am J Sports Med 26:428, 1998.
- Bernstein AD, Breslow MJ, Jazrawi LM: Distal biceps tendon ruptures: a historical perspective and current concepts, Am J Orthop 30:193, 2001.
- Beskin JL, Sanders RA, Hunter SC, et al: Surgical repair of Achilles tendon ruptures, Am J Sports Med 15:1, 1987.
- Bhandari M, Guyatt GH, Siddiqui F, et al: Treatment of acute Achilles tendon ruptures: a systematic overview and metaanalysis, Clin Orthop Relat Res 400:190, 2002.
- Bhole R, Johnson JC: Bilateral simultaneous spontaneous rupture of quadriceps tendons in a diabetic patient, South Med J 78:486, 1985.
- Blazina ME, Kerlan RK, Jobe FW, et al: Jumper’s knee, Orthop Clin North Am 4:665, 1973.
- Bosworth DM: Repair of defects in the tendo Achillis, J Bone Joint Surg 38A:111, 1956.
- Boucher PR, Morton KS: Rupture of the distal biceps brachii tendon, J Trauma 7:626, 1967.
- Bourne MH, Morrey BF: Partial rupture of the distal biceps tendon, Clin Orthop Relat Res 271:143, 1991.
- Boyd HB, Anderson LD: A method for reinsertion of the distal biceps brachii tendon, J Bone Joint Surg 43A:1041, 1961.
- Bradley JB, Tibone JE: Percutaneous and open surgical repairs of Achilles tendon ruptures: a comparative study, Am J Sports Med 18:188, 1990.
- Bugg EI Jr, Boyd BM: Repair of neglected rupture or laceration of the Achilles tendon, Clin Orthop Relat Res 56:73, 1968.
- Calder JDF, Saxby TS: Early, active rehabilitation following mini-open repair of Achilles tendon rupture: a prospective study, Br J Sports Med 39:857, 2005.
- Carroll RE, Hamilton LR: Rupture of biceps brachii: a conservative method of treatment, J Bone Joint Surg 49A:1016, 1967.
- Casey MT Jr, Tietjens BR: Neglected ruptures of the patellar tendon: a case series of four patients, Am J Sports Med 29:457, 2001.
- Ceccarelli F, Berti L, Giuriati L, et al: Percutaneous and minimally invasive techniques of
You Might Also Like