Chronic Unreduced Proximal Tibiofibular Joint Dislocations: Comprehensive Surgical Management
Key Takeaway
Chronic unreduced dislocations of the proximal tibiofibular joint are rare, frequently missed injuries that present with lateral knee pain, ankle instability, or peroneal nerve dysfunction. Operative management is indicated for symptomatic patients failing conservative care. Surgical options include proximal fibular resection or anatomic ligamentous reconstruction. Arthrodesis is generally contraindicated due to its disruption of normal fibular rotation during ankle dorsiflexion, which predictably leads to secondary ankle morbidity.
Introduction to Chronic Proximal Tibiofibular Joint Dislocations
Posttraumatic, chronic subluxation or unreduced dislocation of the proximal tibiofibular joint (PTFJ) is a relatively rare clinical entity. These lesions typically occur following high-energy trauma or complex twisting injuries that disrupt the anterior and posterior capsular ligaments of the PTFJ, often in conjunction with injuries to the fibular collateral ligament (FCL) of the knee.
Because the primary focus during acute trauma is frequently directed toward more obvious intra-articular knee pathology (such as cruciate ligament tears or tibial plateau fractures), PTFJ dislocations are notoriously underappreciated and frequently missed during the initial assessment. When left unreduced, the joint progresses to a state of chronic instability or fixed dislocation, leading to a complex cascade of biomechanical alterations affecting both the knee and the ankle.
Clinical Presentation and Evaluation
An old, unreduced dislocation of the proximal fibula may occasionally be asymptomatic, requiring no formal intervention. However, when symptoms manifest, they can be profoundly debilitating and present a diagnostic challenge due to their varied nature.
Symptomatology
Patients typically present with one or a combination of the following complaints:
* Lateral Knee Pain: Often exacerbated by deep flexion or pivoting movements.
* Mechanical Symptoms: Patients may describe a palpable "clunking" or a sensation of "giving way" during strenuous activities, particularly those involving sudden deceleration or changes in direction.
* Ankle Pain and Instability: Due to the biomechanical coupling of the proximal and distal tibiofibular joints.
* Neurological Deficits: Peroneal nerve dysfunction is a hallmark of severe or chronic PTFJ disruption. Symptoms range from transient paresthesias to profound decreased foot sensation and, in severe cases, foot drop.
Clinical Pearl: Always evaluate the distal syndesmosis and ankle joint in patients presenting with proximal tibiofibular instability. The fibula acts as a single biomechanical strut; proximal pathology frequently translates to distal symptomatology.
Diagnostic Imaging
Standard orthogonal radiographs of the knee (AP and lateral) are the first line of investigation but can be difficult to interpret due to overlapping bony anatomy. Comparison views of the contralateral normal knee are highly recommended. Computed Tomography (CT) is the gold standard for definitively diagnosing subtle subluxations or chronic unreduced dislocations, allowing for precise evaluation of the articular congruity. Magnetic Resonance Imaging (MRI) is invaluable for assessing the integrity of the FCL, biceps femoris tendon, and the common peroneal nerve.
Anatomy and Biomechanics
A profound understanding of the PTFJ anatomy is prerequisite for any surgical intervention. The PTFJ is a synovial joint with a capsule reinforced by robust anterior and posterior ligaments.
Ligamentous Restraints
The primary stabilizers of the PTFJ include:
1. Anterior Superior Tibiofibular Ligament: Composed of two or three broad, flat bands that pass obliquely upward from the anterior aspect of the fibular head to the lateral tibial condyle.
2. Posterior Superior Tibiofibular Ligament: A single, thick, broad band passing from the posterior aspect of the fibular head to the posterior aspect of the lateral tibial condyle.
3. Fibular Collateral Ligament (FCL) and Biceps Femoris: These structures insert on the fibular head and provide dynamic and static stabilization to both the lateral knee and the PTFJ.
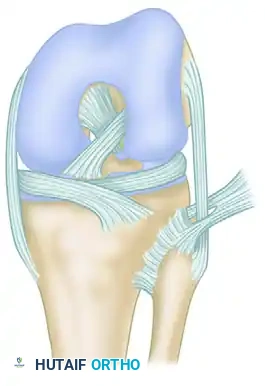
Anterior and lateral ligamentous anatomy of the proximal tibiofibular joint, demonstrating the relationship of the fibular collateral ligament, biceps femoris, and anterior tibiofibular ligament.
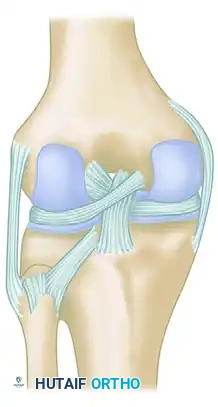
Posterior view highlighting the posterior tibiofibular ligament and the complex posterolateral corner insertions.
Biomechanics of the Fibula
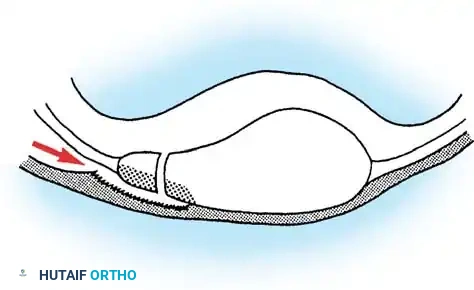
The fibula is not a static bone; it is highly dynamic during the normal gait cycle. During dorsiflexion of the ankle, the wider anterior portion of the talar dome engages the ankle mortise. To accommodate this lateral plane rotation and expansion of the talus, the fibula must translate proximally, move laterally, and rotate externally around its longitudinal axis.
Surgical Warning: Any surgical procedure that rigidly tethers the proximal fibula to the tibia (such as arthrodesis) will abolish this obligate external rotation. This biomechanical mismatch predictably leads to severe ankle pain, restricted dorsiflexion, and secondary ankle instability.
Indications for Treatment
Treatment is strictly dictated by symptomatology. Asymptomatic chronic dislocations discovered incidentally require no treatment.
When symptoms demand intervention, nonoperative modalities should be exhausted first. These include:
* Supportive strapping or bracing (e.g., a proximal tibiofibular strap).
* Targeted physical therapy focusing on biceps femoris and lateral compartment strengthening.
* Activity modification to avoid provocative pivoting maneuvers.
Closed reduction alone for a chronic, unreduced dislocation is universally unsuccessful due to soft tissue contractures, capsular interposition, and fibrotic scarring. When nonoperative treatment is inadequate, surgical intervention is indicated.
Surgical Management Options
Because of the relative rarity of chronic PTFJ dislocations, high-level evidence (Level I/II) from large cohorts with long-term follow-up is lacking. However, established orthopedic principles dictate three primary surgical pathways: Proximal Fibular Resection, Arthrodesis (historically), and Ligamentous Reconstruction.
1. Arthrodesis of the Proximal Tibiofibular Joint (Historical Context)
While arthrodesis has been performed in the past, it is highly problematic and generally contraindicated in modern practice.
As demonstrated in Ogden’s classic studies, fusing the proximal tibiofibular joint eliminates the obligate external rotation of the fibula required during ankle dorsiflexion. In Ogden’s series of four patients treated with PTFJ arthrodesis, three developed severe pain, discomfort, and instability of the ankle joint. Two of these patients required subsequent salvage surgery consisting of resection of the proximal fibula, which successfully relieved their ankle symptoms.
2. Resection of the Proximal Fibula (Fibulectomy)
Most authors historically consider resection of the proximal fibula to be the most reliable option for chronic, painful, unreduced dislocations. It eliminates the painful articulation while preserving ankle biomechanics. However, reservations exist regarding its use in growing children, adolescents, and high-demand athletes due to the alteration of the posterolateral corner (PLC) biomechanics.
Surgical Technique: Proximal Fibular Resection
- Positioning: The patient is placed supine with a sandbag under the ipsilateral hip to internally rotate the leg. A sterile tourniquet is applied.
- Incision: A lateral curvilinear incision is made, starting 3 cm proximal to the joint line, extending distally over the fibular head, and curving anteriorly along the peroneal compartment.
- Nerve Dissection (Critical Step): The common peroneal nerve must be identified and protected. It is located posterior to the biceps femoris tendon, wrapping around the fibular neck. A meticulous neurolysis is performed, freeing the nerve from surrounding scar tissue and retracting it gently with a vessel loop.
- Soft Tissue Detachment: The biceps femoris tendon and the fibular collateral ligament (FCL) are carefully tagged and detached from the fibular head.
- Bone Resection: An oscillating saw is used to resect the proximal 1.5 to 2 cm of the fibula. Care is taken to angle the cut obliquely from proximal-lateral to distal-medial to avoid leaving a prominent bony spike.
- Ligamentous Reattachment: This is the most critical step to prevent iatrogenic posterolateral instability. The tagged FCL and biceps femoris tendon must be securely advanced and reattached to the lateral aspect of the tibial condyle. This is typically achieved using suture anchors or a transosseous bone tunnel technique.
- Closure: The deep fascia is closed meticulously, ensuring no compression on the transposed peroneal nerve.
3. Ligamentous Reconstruction
For younger patients, high-demand athletes, or those in whom preservation of the PLC anatomy is paramount, anatomic or non-anatomic ligamentous reconstruction is the preferred modern approach.
Attempts at reconstruction have utilized various autografts, including split biceps femoris tendon, deep fascia, or free gracilis tendon grafts.
Surgical Technique: Gracilis Autograft Reconstruction
- Graft Harvest: A standard gracilis tendon autograft is harvested from the ipsilateral pes anserinus.
- Approach and Preparation: The PTFJ is exposed via a lateral approach. The common peroneal nerve is identified and protected. The joint is debrided of fibrotic scar tissue, and the fibular head is mobilized.
- Reduction and Temporary Fixation: The fibular head is reduced into its anatomic position on the lateral tibial condyle. Because the joint is chronically unstable, temporary rigid fixation is required. A 3.5 mm or 4.5 mm fully threaded cortical screw is placed across the PTFJ (from the fibula into the tibia) in a syndesmotic fashion. This screw is temporary and must be removed at 3 to 6 months.
- Tunnel Preparation: An anterior-to-posterior bone tunnel is drilled through the fibular head. A corresponding tunnel is drilled in the lateral tibial condyle, mimicking the footprint of the anterior and posterior superior tibiofibular ligaments.
- Graft Passage and Fixation: The gracilis graft is passed through the fibular tunnel and routed into the tibial tunnel in a figure-of-eight fashion to reconstruct both the anterior and posterior ligamentous complexes. The graft is tensioned with the ankle in neutral dorsiflexion and fixed using interference screws or suspensory cortical buttons.
- Closure: Standard layered closure is performed.
Postoperative Rehabilitation Protocols
Rehabilitation depends heavily on the surgical procedure performed.
Post-Fibular Resection Protocol
- Phase 1 (0-2 weeks): Knee immobilized in a hinged brace locked in extension. Weight-bearing as tolerated with crutches. Focus on wound healing and edema control.
- Phase 2 (2-6 weeks): Gradual progression of knee range of motion (ROM). Avoid isolated hamstring (biceps femoris) activation to protect the soft tissue reattachment to the tibia.
- Phase 3 (6-12 weeks): Progressive strengthening of the quadriceps and hamstrings. Return to light jogging at 10-12 weeks.
Post-Ligamentous Reconstruction Protocol
- Phase 1 (0-6 weeks): Strict non-weight-bearing or touch-down weight-bearing to protect the temporary syndesmotic screw and graft. Knee brace locked in extension during ambulation. Passive ROM allowed from 0 to 90 degrees.
- Phase 2 (6-12 weeks): Progression to full weight-bearing. Active ROM exercises initiated.
- Hardware Removal: The temporary trans-articular screw is removed under local or brief general anesthesia between 3 and 6 months postoperatively, prior to the initiation of high-impact activities.
- Phase 3 (3-6 months): Advanced proprioceptive training, plyometrics, and sport-specific rehabilitation following screw removal.
Complications and Pitfalls
Surgeons managing chronic PTFJ dislocations must be prepared to navigate several severe complications:
- Common Peroneal Nerve Palsy: The most devastating complication. It can occur from direct iatrogenic injury during dissection, traction neuropraxia during fibular reduction, or postoperative hematoma compression. Meticulous neurolysis and careful retractor placement are mandatory.
- Posterolateral Corner (PLC) Instability: Failure to adequately reattach the FCL and biceps femoris to the tibia during a fibulectomy will result in profound varus and rotatory instability of the knee.
- Ankle Morbidity: As discussed, arthrodesis or failure to remove a temporary syndesmotic screw will restrict fibular rotation, leading to secondary ankle pain and syndesmotic widening.
- Recurrent Instability: Can occur following ligamentous reconstruction if the graft stretches out or if the temporary fixation is removed prematurely before biologic graft incorporation occurs.
Conclusion
Chronic unreduced dislocations of the proximal tibiofibular joint represent a complex biomechanical challenge. While conservative measures may suffice for low-demand or asymptomatic patients, surgical intervention is required for those with persistent pain, instability, or neurological symptoms. Proximal fibular resection with meticulous PLC reconstruction remains a reliable workhorse procedure, while anatomic ligamentous reconstruction with temporary screw fixation offers an excellent joint-preserving alternative for younger, high-demand patients. Arthrodesis should be relegated to historical interest due to its unacceptable rate of secondary ankle morbidity.
You Might Also Like