Tibialis Anterior Tendon Rupture: From Diagnosis to Full Recovery
Key Takeaway
Discover the latest medical recommendations for Tibialis Anterior Tendon Rupture: From Diagnosis to Full Recovery. A tibialis anterior tendon rupture is an injury presenting as acute pain or chronic painless foot drop, often with delayed diagnosis. This crucial tendon originates from the lateral tibial condyle and inserts into the medial cuneiform, controlling ankle dorsiflexion. Ruptures commonly occur in older individuals with degenerative tendinopathy, often near its insertion, and can cause gait disturbance.
Introduction and Epidemiology
Tibialis anterior tendon rupture is an infrequent but highly morbid clinical entity that significantly impairs lower extremity biomechanics and gait efficiency. While it represents the third most common lower extremity tendon rupture—following the Achilles and patellar tendons—its absolute incidence remains relatively low, contributing to a high rate of delayed or missed diagnoses. The clinical presentation is dichotomous, manifesting either as an acute traumatic injury in younger, active patients or as a chronic, often painless, foot drop in older individuals with preexisting degenerative tendinopathy.

In the acute setting, patients may report a sudden "pop" or tearing sensation on the anterior aspect of the ankle following an eccentric loading event. Conversely, chronic ruptures frequently present insidiously. Patients may complain of a gait disturbance, specifically a "slap foot" gait or a tendency to trip over uneven terrain, rather than acute pain. The diagnosis is frequently delayed, with literature suggesting that up to 50% of cases are initially misdiagnosed as peroneal nerve palsy, lumbar radiculopathy (specifically L5), or generalized lower extremity weakness.

Epidemiologically, spontaneous ruptures predominantly affect males in their sixth to eighth decades of life. These cases are almost exclusively associated with underlying degenerative tendinosis, microvascular compromise, and repetitive microtrauma. Systemic risk factors mirroring those of Achilles tendinopathy—such as diabetes mellitus, inflammatory arthropathies, local corticosteroid injections, and fluoroquinolone use—are frequently implicated in the pathogenesis. In contrast, younger patients typically sustain lacerations from penetrating trauma or experience ruptures secondary to high-energy distal tibia fractures or compartment syndrome.
Surgical Anatomy and Biomechanics
A thorough understanding of the tibialis anterior musculotendinous unit is paramount for accurate diagnosis and successful surgical reconstruction. The tibialis anterior muscle originates from the lateral condyle and the proximal two-thirds of the lateral surface of the tibia, as well as the adjacent interosseous membrane and the deep surface of the crural fascia.

The musculotendinous junction typically forms at the transition between the middle and distal thirds of the tibia. From this junction, the tendon courses distally within a distinct synovial sheath. It passes deep to the superior extensor retinaculum and the upper band of the inferior extensor retinaculum. The tendon ultimately inserts onto the medial and plantar surfaces of the medial cuneiform and the inferomedial base of the first metatarsal.

Vascular supply to the tendon is derived primarily from branches of the anterior tibial artery. Injection studies have demonstrated a distinct hypovascular zone located approximately 2 to 3 cm proximal to its insertion. This watershed area correlates clinically with the most frequent site of spontaneous rupture, secondary to compromised healing capacity and degenerative susceptibility. Innervation is provided by the deep peroneal nerve (L4, L5), which descends adjacent to the anterior tibial artery between the tibialis anterior and extensor hallucis longus (EHL) muscles.

Biomechanically, the tibialis anterior is the primary dorsiflexor of the ankle, contributing approximately 80% of the total dorsiflexion torque. During the normal gait cycle, the muscle performs two critical functions. First, during the initial contact phase (heel strike to foot flat), the tibialis anterior contracts eccentrically to decelerate plantarflexion, preventing the foot from slapping against the ground. Second, during the swing phase, it contracts concentrically to dorsiflex the ankle, allowing the foot to clear the ground.

Rupture of the tendon obliterates these mechanisms. The loss of eccentric control results in the characteristic "slap foot" at heel strike, while the loss of concentric dorsiflexion leads to a "steppage" gait, wherein the patient must hyperflex the hip and knee to prevent the toes from dragging. Over time, the unopposed action of the Achilles tendon and posterior compartment musculature inevitably leads to an equinus contracture of the ankle.
Indications and Contraindications
The decision-making process for managing tibialis anterior tendon ruptures hinges on patient age, functional demands, medical comorbidities, and the chronicity of the tear. While conservative management may yield acceptable results in sedentary, low-demand individuals, surgical intervention is the standard of care for active patients to restore normal gait mechanics and prevent secondary equinus contractures.

Nonsurgical treatment typically involves the use of an ankle-foot orthosis (AFO) to hold the ankle in neutral, thereby facilitating ground clearance during the swing phase. However, conservative management does not restore active dorsiflexion strength, and patients often experience persistent fatigue and difficulty on uneven terrain. Surgical management, ranging from primary end-to-end repair to complex tendon transfers or allograft reconstructions, aims to restore the continuity and tension of the musculotendinous unit.

Operative Versus Non Operative Management
| Variable | Operative Management | Non-Operative Management |
|---|---|---|
| Patient Profile | Young, active, high functional demand | Elderly, sedentary, low functional demand |
| Chronicity | Acute or subacute ruptures (< 6-8 weeks) | Chronic, asymptomatic ruptures in frail patients |
| Clinical Exam | Unacceptable gait disturbance, severe weakness | Tolerable gait with AFO, minimal ambulatory needs |
| Comorbidities | Medically optimized for surgery | Severe peripheral vascular disease, uncontrolled diabetes, high anesthetic risk |
| Tissue Quality | Reparable tendon or viable local transfer options | Massive soft tissue compromise, active local infection |
| Goal | Restore active dorsiflexion and normal gait | Prevent tripping, stabilize gait with orthosis |
Pre Operative Planning and Patient Positioning
Comprehensive preoperative planning begins with a meticulous physical examination. The examiner must palpate the entire course of the tibialis anterior tendon. In acute cases, a palpable defect or gap is often appreciated, frequently accompanied by localized edema and ecchymosis. An anterior ankle mass may be present, representing the retracted proximal stump of the ruptured tendon.

Manual motor testing will reveal absent or profoundly weak ankle dorsiflexion. It is critical to observe for extensor substitution; patients will often recruit the extensor hallucis longus (EHL) and extensor digitorum longus (EDL) in an attempt to dorsiflex the ankle, resulting in marked hyperextension of the toes. The examiner must also assess for heel cord tightness. Subacute and chronic injuries frequently present with secondary Achilles contractures. A minimum of 10 degrees of passive ankle dorsiflexion is required for a successful tibialis anterior reconstruction; failure to achieve this necessitates a concomitant gastrocnemius recession or Achilles tendon lengthening.
Diagnostic imaging is essential. Weight-bearing radiographs of the foot and ankle should be obtained to rule out avulsion fractures of the medial cuneiform or base of the first metatarsal, and to assess for underlying midfoot osteoarthritis. Magnetic Resonance Imaging (MRI) is the gold standard for preoperative evaluation.

MRI accurately delineates the location of the tear, the degree of proximal tendon retraction, and the quality of the remaining tendon substance. Furthermore, T1-weighted sagittal and axial sequences are critical for evaluating the tibialis anterior muscle belly for fatty infiltration and atrophy. Severe fatty degeneration (Goutallier stage 3 or 4) suggests irreversible muscle damage, which may portend poor functional recovery even with a structurally sound tendon repair, potentially altering the surgical plan toward a tendon transfer rather than direct repair.

Patient Positioning and Preparation
The patient is placed in the supine position on the operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot and ankle into a neutral, upward-facing position, counteracting the natural external rotation of the lower extremity.

A thigh tourniquet is applied to provide a bloodless surgical field. The entire lower extremity is prepped and draped in a standard sterile fashion. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation. Depending on the anticipated complexity of the reconstruction (e.g., need for allograft or autograft harvest), the surgical field should allow access to the proximal tibia or ipsilateral knee if a hamstring autograft is considered.
Detailed Surgical Approach and Technique
The surgical strategy is dictated by the gap length between the tendon ends after debridement and the chronicity of the rupture. Acute ruptures with minimal retraction can typically be managed with primary end-to-end repair. Chronic ruptures with large defects require reconstruction utilizing tendon transfers, sliding lengthening, or interpositional grafting.
Incision and Superficial Dissection
An anteromedial longitudinal incision is utilized, centered over the palpable defect or the expected course of the tibialis anterior tendon. The incision typically extends from the distal third of the tibia to the medial cuneiform.

Careful subcutaneous dissection is performed to protect the terminal branches of the superficial peroneal nerve laterally and the saphenous nerve medially. The superficial fascia is incised, exposing the extensor retinaculum.

The superior and inferior extensor retinacula are meticulously incised in a step-cut or Z-lengthening fashion. Preserving the retinaculum is crucial; it must be repaired at the conclusion of the procedure to prevent bowstringing of the reconstructed tendon during active dorsiflexion.
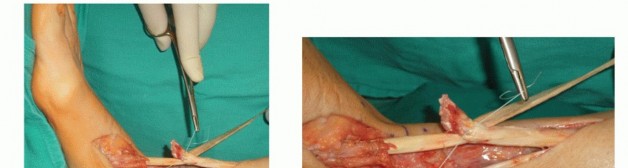
Tendon Retrieval and Debridement
Once the tendon sheath is opened, the ruptured ends are identified. In chronic cases, the proximal stump is often encased in dense scar tissue and retracted proximally into the anterior compartment.

The tendon ends must be aggressively debrided back to healthy, viable tissue. Degenerative, mucin-infiltrated tendon appears yellow, disorganized, and friable; this tissue will not hold suture and must be excised until firm, white, parallel collagen bundles are visualized.

The proximal tendon is then mobilized by bluntly dissecting the muscle belly from the surrounding anterior compartment fascia. Applying distal traction to the proximal stump while plantarflexing the ankle allows the surgeon to assess the size of the residual defect.
Primary Repair Technique
If the tendon ends can be opposed with the ankle in neutral dorsiflexion (typically defects < 2-3 cm after mobilization), a primary repair is performed.

A heavy, non-absorbable, braided suture (e.g., #2 or #5 FiberWire or Ethibond) is woven into the proximal and distal stumps utilizing a locking Krackow or modified Kessler technique. At least three to four locking loops should be placed on each side of the rupture to ensure adequate pull-out strength.

If the rupture occurs at or very near the insertion on the medial cuneiform, there may be insufficient distal tendon for a suture weave. In these instances, the proximal stump is reattached directly to the bony footprint using suture anchors or a bi-cortical button technique. The footprint on the medial cuneiform is decorticated to bleeding bone to promote biologic healing.

Reconstruction of Chronic Defects
For defects exceeding 3 cm that cannot be closed under physiologic tension, reconstruction is mandatory. Several techniques are available:
1. Extensor Hallucis Longus (EHL) Transfer: The EHL tendon is harvested distally, routed through the tibialis anterior sheath, and woven into the proximal TA stump. To prevent a drop hallux, the distal stump of the EHL is tenodesed to the extensor hallucis brevis (EHB) or the adjacent EDL tendon.
2. Sliding Tendon Lengthening: A fractional lengthening of the proximal TA tendon or a V-Y advancement of the musculotendinous junction can provide 2 to 3 cm of additional length.
3. Interpositional Grafting: Free autograft (e.g., semitendinosus, gracilis, or plantaris) or allograft (e.g., Achilles, anterior tibialis, or peroneus longus) can be utilized to bridge massive defects.

When using a graft, the Pulvertaft weave technique is preferred to maximize the surface area for healing. The graft is passed through longitudinal slits in the native tendon stumps and sutured in place under appropriate tension.

The tensioning of the repair or reconstruction is a critical step. The ankle must be held in neutral (0 degrees) or slight dorsiflexion while the final knots are tied. This ensures that the resting tension of the muscle is restored, allowing for effective concentric contraction postoperatively.

Following the tendon repair, the extensor retinaculum is carefully reapproximated over the tendon to prevent bowstringing. If the retinaculum is tight, it may be repaired in a lengthened fashion, but it must be competent. The subcutaneous tissues and skin are closed in layers.
Complications and Management
Surgical intervention for tibialis anterior tendon rupture is generally highly successful, but complications can occur, particularly in patients with underlying vasculopathy or diabetes. Meticulous surgical technique and strict adherence to postoperative protocols are essential for minimizing these risks.

Wound healing complications are the most frequently encountered issue, given the thin soft tissue envelope over the anterior ankle. Dehiscence or superficial infection can often be managed with local wound care and oral antibiotics. However, deep infections involving the tendon repair or graft require aggressive surgical debridement and intravenous antibiotics, which may compromise the ultimate functional outcome.

Neurologic injury is another potential pitfall. The superficial peroneal nerve is at risk during the lateral aspect of the dissection, while the deep peroneal nerve can be injured during deep dissection or aggressive retraction. Neuromas resulting from iatrogenic nerve injury can cause debilitating chronic pain.

Summary of Common Complications
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Wound Dehiscence / Infection | 5 - 10% | Prevention: Atraumatic soft tissue handling, optimize diabetic control, limit tourniquet time. Salvage: Aggressive debridement, negative pressure wound therapy, local rotational flaps if tendon is exposed. |
| Tendon Re-Rupture | 2 - 5% | Prevention: Secure locking sutures, appropriate postoperative immobilization, avoid early aggressive stretching. Salvage: Revision surgery with allograft reconstruction or tendon transfer. |
| Persistent Weakness / Foot Drop | 10 - 15% | Prevention: Ensure adequate tensioning at neutral dorsiflexion during surgery, address equinus contractures. Salvage: Prolonged physical therapy, AFO utilization, consider revision for severe laxity. |
| Tendon Bowstringing | < 5% | Prevention: Meticulous repair of the superior and inferior extensor retinaculum. Salvage: Surgical reconstruction of the retinaculum using local tissue or graft. |
| Superficial Peroneal Nerve Injury | 3 - 8% | Prevention: Careful superficial dissection, avoid excessive self-retaining retractors. Salvage: Gabapentinoids, targeted nerve blocks, surgical excision of neuroma and burying into muscle. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is designed to protect the integrity of the repair while mitigating the risks of stiffness, adhesions, and muscle atrophy. The protocol spans several months and requires high patient compliance.

Phase I: Protection (Weeks 0-2)
Immediately following surgery, the patient is placed in a well-padded short leg cast or rigid posterior splint with the ankle secured in neutral or slight dorsiflexion. The patient is instructed to remain strictly non-weight-bearing (NWB) on the operative extremity. Elevation and cryotherapy are emphasized to control edema and promote wound healing.
Phase II: Controlled Mobilization (Weeks 2-6)
At the two-week mark, sutures are removed, and the patient is transitioned into a removable controlled ankle motion (CAM) boot. The ankle remains locked in neutral. The patient may begin progressive partial weight-bearing with crutches. Gentle, passive range of motion (ROM) exercises for dorsiflexion and plantarflexion are initiated under the guidance of a physical therapist. Active plantarflexion is permitted, but active dorsiflexion is strictly prohibited to avoid placing tension on the healing repair.


You Might Also Like


