Arthroscopic Management of Cam-Type Femoroacetabular Impingement: A Comprehensive Surgical Guide
Key Takeaway
Cam-type femoroacetabular impingement (FAI) results from an aspherical femoral head-neck junction causing abnormal contact with the acetabular rim. Arthroscopic management involves transitioning from the central to the peripheral compartment, dynamic assessment, and precise osteochondroplasty to restore the femoral head-neck offset. This guide details the indications, patient positioning, portal placement, and step-by-step surgical technique required to achieve optimal impingement-free range of motion while preserving capsular integrity and hip biomechanics.
Introduction to Cam Impingement and Femoroacetabular Biomechanics
Femoroacetabular impingement (FAI) is a dynamic, pathomechanical process characterized by abnormal contact between the proximal femur and the acetabular rim. Cam impingement, specifically, arises from an aspherical femoral head-neck junction—often described as a "pistol grip" deformity or a reduction in the normal femoral head-neck offset. During hip flexion and internal rotation, this osseous prominence is forcefully driven into the anterosuperior acetabulum.
The biomechanical consequence of this repetitive abutment is profound. The cam lesion generates massive shear forces at the chondrolabral junction, leading to inside-out delamination of the acetabular articular cartilage and subsequent tearing or detachment of the acetabular labrum. If left untreated, cam impingement is a well-documented precursor to early-onset osteoarthritis of the hip.
Arthroscopic osteochondroplasty has emerged as the gold standard for addressing cam morphology. The procedure demands a meticulous understanding of hip anatomy, precise portal placement, and a systematic approach to both the central and peripheral compartments of the hip joint.
Clinical Pearl: The primary goal of cam resection is not merely to create a perfectly spherical head, but to restore a functional, impingement-free range of motion while meticulously preserving the lateral retinacular vessels that supply the femoral head.
Clinical Evaluation and Indications
Patient Presentation
Patients typically present with insidious onset, activity-related groin pain that is exacerbated by prolonged sitting, deep squatting, or pivoting movements. The "C-sign" is a classic presentation, where the patient cups their hand over the greater trochanter to describe deep, internal hip pain.
Physical Examination
The anterior impingement test (FADIR: Flexion, Adduction, Internal Rotation) is highly sensitive for anterior FAI and labral pathology. A positive test reproduces the patient's characteristic groin pain. The FABER (Flexion, Abduction, External Rotation) test may also elicit pain or demonstrate restricted range of motion compared to the contralateral side.
Imaging and Preoperative Planning
- Radiographs: Anteroposterior (AP) pelvis, Dunn 45-degree, and cross-table lateral views are mandatory. The alpha angle (normal < 50-55 degrees) is measured on the lateral views to quantify the severity of the cam lesion.
- Magnetic Resonance Imaging (MRI) / MR Arthrogram: Essential for evaluating the integrity of the acetabular labrum, the extent of chondral delamination, and the exact three-dimensional morphology of the cam lesion.
- Computed Tomography (CT): 3D CT reconstructions are increasingly utilized for precise preoperative mapping of the resection volume.
Preoperative Positioning and Setup
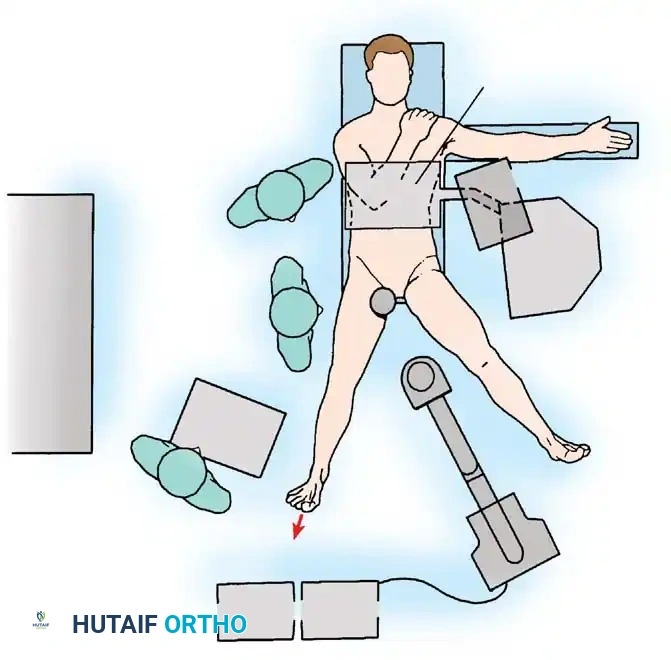
Proper patient positioning is the foundation of a successful hip arthroscopy. The procedure is typically performed with the patient in the supine position on a specialized traction table, though the lateral decubitus position is an acceptable alternative depending on surgeon preference.
Supine Traction Setup
- Perineal Post: A well-padded, oversized perineal post is positioned eccentrically against the medial thigh of the operative leg to lateralize the vector of traction and minimize pressure on the pudendal nerve.
- Traction Application: Gross traction is applied to the operative leg to distract the hip joint by approximately 10 to 15 mm, breaking the suction seal of the joint. This is confirmed via fluoroscopy.
- Counter-Traction: The non-operative leg is placed in slight abduction and traction to stabilize the pelvis.
Surgical Warning: Traction time must be strictly monitored. To prevent neuropraxia of the pudendal or sciatic nerves, continuous traction should not exceed 2 hours. The transition to the peripheral compartment (which removes traction) should be executed as efficiently as possible.
Portal Placement and Diagnostic Arthroscopy
Establishing safe and effective portals is critical to avoid iatrogenic injury to the lateral femoral cutaneous nerve (LFCN), the femoral neurovascular bundle, and the superior gluteal nerve.
Standard Portals
- Anterolateral (AL) Portal: Established first under fluoroscopic guidance. It is located 1 cm anterior and 1 cm superior to the tip of the greater trochanter. This portal enters the capsule at the superior/lateral aspect of the femoral neck.
- Mid-Anterior Portal (MAP): Established under direct arthroscopic visualization from the AL portal. It is located approximately 5 to 7 cm distal and slightly anterior to the AL portal, in line with the anterior margin of the greater trochanter.
- Distal Anterolateral Accessory (DALA) Portal: Often required for optimal trajectory during cam resection in the peripheral compartment.
Central Compartment Evaluation and Treatment
Following the principles outlined by Mauro et al., the surgical intervention begins in the central compartment under traction.
- Diagnostic Sweep: Evaluate the ligamentum teres, acetabular fossa, articular cartilage, and labrum.
- Intervention: Complete any necessary central compartment procedures first. This includes labral repair or reconstruction, resection of pincer lesions (acetabular rim trimming), and treatment of chondral defects (e.g., microfracture or chondroplasty).
Once the central compartment pathology is fully addressed, the surgeon must transition to the peripheral compartment to address the cam lesion.
Surgical Technique: Arthroscopic Osteochondroplasty
The transition from the central to the peripheral compartment is a critical juncture in the procedure. The capsule must be adequately managed, and the hip dynamically repositioned to expose the femoral head-neck junction.
Transition to the Peripheral Compartment
As explicitly detailed in standard operative protocols:
1. Release Traction: Remove the leg from traction completely. This eliminates the risk of traction-related neuropraxia and relaxes the anterior capsule.
2. Hip Flexion: Flex the hip to approximately 45 degrees.
- Biomechanical Rationale: Flexing the hip relaxes the robust iliofemoral ligament, allowing the capsule to distend anteriorly. Furthermore, this degree of flexion rotates the anterior and anterolateral cam deformity directly into the arthroscopic field of view.
Capsulotomy and Exposure
To adequately visualize the cam lesion, a capsulotomy is required. An interportal capsulotomy connecting the AL and MAP portals is standard. If the cam lesion is extensive, a T-capsulotomy extending distally along the femoral neck may be necessary.
Surgical Warning: When performing a T-capsulotomy, avoid extending the vertical limb too far distally or laterally to prevent injury to the zona orbicularis and the lateral retinacular vessels.
Arthroscopic Osteochondroplasty (Femoral Neck Reshaping)
With the peripheral compartment exposed and the hip flexed:
1. Visualization: Place the 70-degree or 30-degree arthroscope in the mid-anterior portal (MAP) to look back toward the femoral neck.
2. Instrumentation: Introduce a motorized arthroscopic burr (typically 4.0 mm or 5.5 mm) or an arthroscopic blade through a distal accessory portal (DALA).
3. Defining the Boundaries:
- Medial/Inferior Boundary: The medial synovial fold.
- Lateral/Superior Boundary: The lateral retinacular vessels. Never resect bone superior or lateral to these vessels, as they provide the terminal blood supply to the femoral head. Damage here can result in avascular necrosis (AVN).
- Proximal Boundary: The articular cartilage margin.
4. Resection: Begin resecting the aspherical bone of the cam lesion. The goal is to recreate a concave, spherical contour at the head-neck junction. The resection typically tapers distally toward the intertrochanteric line.
5. Fluoroscopic Confirmation: Utilize dynamic fluoroscopy during the resection. An AP view, Dunn view, and cross-table lateral view should be obtained intraoperatively to confirm adequate restoration of the alpha angle and to ensure no over-resection has occurred. Over-resection (greater than 30% of the femoral neck diameter) significantly increases the risk of a postoperative femoral neck fracture.
Dynamic Assessment
Once the osteochondroplasty is visually and fluoroscopically satisfactory, the surgeon must perform a dynamic arthroscopic examination.
- Release the arthroscopic instruments but keep the camera in the joint.
- Have an assistant take the hip through a full range of motion, specifically mimicking the FADIR test (flexion to 90 degrees, adduction, and internal rotation).
- Directly visualize the head-neck junction entering the acetabulum. There should be a smooth, gliding articulation with no residual abutment against the repaired labrum or acetabular rim.
Capsular Management
Following the dynamic assessment, the capsulotomy must be addressed. Routine capsular closure (or plication in cases of microinstability) is strongly recommended. Failure to close the capsule, particularly the vertical limb of a T-capsulotomy, can lead to iatrogenic anterior hip instability, subluxation, or persistent pain. Closure is achieved using high-strength non-absorbable sutures passed via specialized arthroscopic suture shuttling devices.
Postoperative Rehabilitation Protocol
Rehabilitation following arthroscopic cam resection is phased and requires strict adherence to protect the osteochondroplasty site and capsular closure.
Phase 1: Protection and Early Motion (Weeks 0-4)
- Weight Bearing: Flat-foot touch weight-bearing (approx. 20 lbs) using crutches for 3 to 4 weeks to protect the femoral neck from stress fractures.
- Range of Motion: Continuous Passive Motion (CPM) machine or stationary biking (no resistance) begins on postoperative day 1 to prevent adhesions.
- Restrictions: Avoid active hip flexion (to prevent hip flexor tendinitis) and limit external rotation and extension to protect the capsular closure.
Phase 2: Gait Normalization and Strengthening (Weeks 4-8)
- Weight Bearing: Progress to full weight-bearing and wean off crutches.
- Strengthening: Initiate isometric and concentric strengthening of the gluteus medius, core musculature, and quadriceps.
- Aquatic Therapy: Can be introduced once portal sites are completely healed.
Phase 3: Advanced Strengthening (Weeks 8-12)
- Focus on eccentric control, closed kinetic chain exercises, and proprioception.
- Progression of core stability and pelvic control.
Phase 4: Return to Sport (Months 3-6)
- Introduction of plyometrics, cutting, and sport-specific drills.
- Clearance for full return to sport is typically granted between 4 to 6 months, contingent upon symmetrical strength, pain-free full ROM, and successful completion of functional testing.
Complications and Pitfalls
While arthroscopic treatment of cam impingement is highly successful, surgeons must be vigilant regarding potential complications:
- Inadequate Resection: The most common cause of revision hip arthroscopy. Failure to adequately resect the distal or lateral extent of the cam lesion results in persistent impingement and continued pain.
- Over-Resection: Resecting more than 30% of the femoral neck diameter creates a stress riser, predisposing the patient to a catastrophic femoral neck fracture.
- Avascular Necrosis (AVN): Caused by iatrogenic injury to the lateral epiphyseal (retinacular) vessels during superior/lateral cam resection.
- Iatrogenic Instability: Resulting from failure to repair a large capsulotomy, particularly in patients with underlying borderline dysplasia or generalized ligamentous laxity.
- Nerve Injury: Pudendal neuropraxia from prolonged traction, or LFCN injury from improper anterior portal placement.
- Heterotopic Ossification (HO): Prophylaxis with NSAIDs (e.g., Naproxen or Indomethacin) for 2 to 3 weeks postoperatively is routinely recommended to prevent HO in the pericapsular tissues.
Conclusion
The arthroscopic management of cam impingement is a highly technical but immensely rewarding procedure that alters the natural history of femoroacetabular impingement. By mastering the transition from the central to the peripheral compartment, respecting the vascular anatomy of the femoral neck, and executing a precise, dynamically verified osteochondroplasty, the orthopaedic surgeon can reliably restore hip biomechanics, alleviate pain, and protect the joint from premature degeneration.
You Might Also Like