Extraarticular Ankylosis in Flexion: Pathoanatomy, Biomechanics, and Surgical Reconstruction
Key Takeaway
Extraarticular flexion ankylosis of the knee presents a complex reconstructive challenge characterized by posterior tibial subluxation and external rotation. Management requires a meticulous balance of conservative modalities, such as dynamic splinting, and surgical interventions, including hamstring release and external fixation. Extreme caution is paramount during correction to prevent iatrogenic peroneal nerve palsy. This guide details the pathoanatomy, biomechanics, and step-by-step surgical protocols for optimal deformity correction.
INTRODUCTION TO EXTRAARTICULAR ANKYLOSIS IN FLEXION
Extraarticular ankylosis of the knee in flexion represents a profoundly debilitating orthopedic condition, significantly more prevalent than its extension counterpart. Unlike intraarticular ankylosis, which is characterized by intraarticular bony fusion or severe fibrous adhesions within the joint space, extraarticular ankylosis is driven by the severe contracture of the periarticular soft tissues. This condition severely compromises the patient's gait biomechanics, leading to a cascade of compensatory deformities in the ipsilateral hip, ankle, and contralateral limb, ultimately resulting in severe functional impairment and increased energy expenditure during ambulation.
The management of extraarticular flexion contractures demands a comprehensive understanding of knee biomechanics, soft tissue tethering, and neurovascular anatomy. The orthopedic surgeon must navigate a complex interplay of contracted posterior structures while meticulously avoiding iatrogenic injury, particularly to the highly vulnerable common peroneal nerve. This masterclass delineates the pathoanatomy, preoperative optimization, and advanced surgical techniques required to address this formidable deformity.
PATHOANATOMY AND BIOMECHANICS
The pathoanatomy of extraarticular flexion ankylosis is rarely a simple uniplanar deformity. It is a complex, multiplanar distortion of the knee joint driven by the chronic, unopposed pull of the posterior musculature and the subsequent adaptive shortening of the capsuloligamentous structures.
The Deforming Forces
The primary drivers of the deformity are the hamstring muscles. In the presence of a chronic flexion posture (often secondary to trauma, prolonged immobilization, neuromuscular disorders, or inflammatory arthropathies), these muscles undergo myostatic contracture.
* Posterior Subluxation: The semimembranosus, semitendinosus, and biceps femoris exert a continuous posterior translational force on the proximal tibia. As the posterior capsule shortens, the tibia is drawn posteriorly, leading to subluxation of the tibiofemoral articulation.
* External Rotation: The biceps femoris and the iliotibial band exert a strong external rotatory moment on the tibia. Over time, this results in a fixed external rotation deformity of the tibia relative to the femur, further complicating the mechanical axis of the lower extremity.
Adaptive Soft Tissue Changes
All soft tissues within the popliteal fossa undergo adaptive shortening. This includes:
* The posterior joint capsule and the oblique popliteal ligament.
* The collateral ligaments (which may become contracted in their posterior fibers).
* The popliteal artery and vein.
* The tibial and common peroneal nerves.
Clinical Pearl: The severity of the bony deformity is often secondary to the soft tissue contracture. However, in long-standing cases, adaptive remodeling of the femoral condyles and tibial plateau may occur, necessitating osseous procedures in addition to soft tissue releases.
CLINICAL EVALUATION AND PREOPERATIVE PLANNING
A meticulous clinical and radiographic evaluation is paramount to differentiate extraarticular contractures from intraarticular pathology and to formulate an appropriate surgical strategy.
Physical Examination
- Gait Analysis: Assess for compensatory mechanisms such as increased lumbar lordosis, ipsilateral hip flexion, and equinus posturing of the ankle.
- Range of Motion (ROM): Document the exact degree of the flexion contracture and the total arc of motion.
- Neurovascular Status: A rigorous baseline assessment of the sciatic, tibial, and common peroneal nerves is mandatory. Document any pre-existing sensory or motor deficits.
- Joint Stability: Assess for posterior sag and external rotation of the tibial tubercle to quantify the degree of subluxation.
Imaging Modalities
- Standard Radiographs: Weight-bearing anteroposterior (AP), lateral, and skyline views. The lateral view is critical for assessing the degree of posterior tibial subluxation and any adaptive flattening of the femoral condyles.
- Computed Tomography (CT): Useful in long-standing cases to evaluate 3D bony architecture and plan for potential osteotomies.
- Magnetic Resonance Imaging (MRI): Indicated to assess the integrity of the intraarticular structures (cruciate ligaments, menisci) and the extent of posterior capsular thickening.
CONSERVATIVE MANAGEMENT: THE PREOPERATIVE ADJUNCT
Flexion contractures can often be partially corrected through conservative measures. The efficacy of these modalities is inversely proportional to the severity and chronicity of the deformity. Conservative management is rarely curative for severe ankylosis but serves as a critical preoperative adjunct to reduce the magnitude of the required surgical release, thereby minimizing neurovascular risk.
Modalities of Conservative Correction
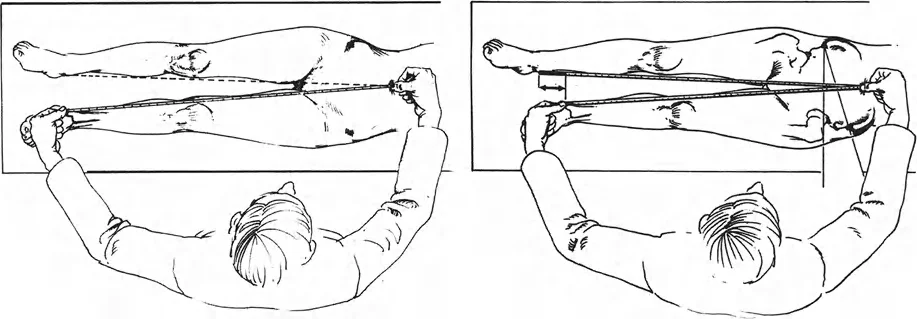
- Traction: Balanced suspension or Buck's extension traction can provide a continuous, low-load stretch to the posterior structures.
- Dynamic Splinting: Devices such as the Dynasplint apply a prolonged, low-load stretching force, capitalizing on the viscoelastic properties of the contracted soft tissues to induce creep.
- Serial Casting: Drop-out casts or serial wedging can gradually improve extension. However, extreme care must be taken to avoid creating a posterior subluxation force on the tibia during cast application.
- Custom Bracing: Extension-assist knee-ankle-foot orthoses (KAFOs) can be utilized both preoperatively and postoperatively to maintain gains in extension.
Surgical Warning: When utilizing serial casting or dynamic splinting, the fulcrum of extension must be carefully controlled. Applying an extension force to the distal tibia without supporting the proximal tibia posteriorly will exacerbate posterior tibiofemoral subluxation rather than correct the joint angle.
SURGICAL MANAGEMENT: INDICATIONS AND APPROACHES
When conservative measures plateau or fail to achieve a functional arc of motion, surgical intervention is indicated. The surgical strategy is dictated by the severity of the contracture, the presence of subluxation, and the status of the articular cartilage.
1. Open Soft Tissue Release (Posterior Capsulotomy and Hamstring Lengthening)
For moderate contractures (typically 20 to 45 degrees) without severe bony remodeling, an open soft tissue release is the procedure of choice.
Patient Positioning:
The patient is positioned prone on a radiolucent operating table. A high thigh tourniquet is applied. The limb must be draped free to allow intraoperative assessment of the range of motion and joint reduction.
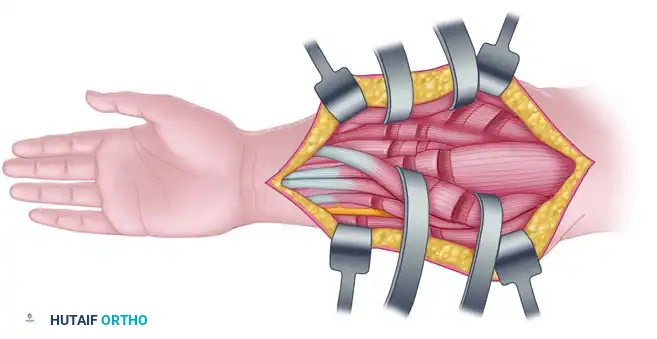
Surgical Approach:
A utilitarian S-shaped incision across the popliteal fossa is classically described, though dual medial and lateral longitudinal incisions are increasingly preferred to avoid wound healing complications in the popliteal crease.
Step-by-Step Technique:
1. Neurovascular Identification: The most critical initial step is the identification and protection of the common peroneal nerve laterally and the tibial nerve and popliteal vessels centrally. The common peroneal nerve is traced from the posterior aspect of the biceps femoris down to the fibular neck.
2. Hamstring Lengthening:
* Medial: The semimembranosus and semitendinosus tendons are identified. A Z-lengthening or fractional lengthening is performed depending on the severity of the contracture.
* Lateral: The biceps femoris tendon is Z-lengthened. Crucial: The common peroneal nerve lies immediately deep and medial to the biceps tendon; meticulous dissection is required.
3. Iliotibial Band Release: If external rotation and valgus forces are present, the posterior fibers of the iliotibial band are released or lengthened.
4. Posterior Capsulotomy: The popliteal vessels are gently retracted. The origins of the medial and lateral gastrocnemius muscles are elevated from the posterior femoral condyles. A transverse incision is made through the posterior capsule, taking care not to damage the intraarticular structures (cruciate ligaments).
5. Assessment: The knee is gently extended. If full extension is not achieved, further release of the posterior cruciate ligament (PCL) may be necessary, though this risks iatrogenic instability.
2. Gradual Distraction via External Fixation
For severe contractures (>45 degrees), long-standing deformities, or cases complicated by severe posterior subluxation, acute open release carries an unacceptably high risk of neurovascular compromise. In these scenarios, gradual distraction osteogenesis principles utilizing external fixation are indicated.
Biomechanical Rationale:
Gradual distraction allows for the simultaneous correction of flexion, posterior subluxation, and external rotation while providing the neurovascular structures time to adapt via histogenesis.
Frame Constructs:
* Ilizarov Circular Fixator / Taylor Spatial Frame (TSF): These multiplanar devices offer the highest degree of control. Rings are applied to the distal femur and proximal tibia.
* Monolateral Fixators (e.g., Orthofix): Can be used for simpler, uniplanar flexion contractures, though they offer less control over subluxation and rotation.
Surgical Technique (Circular Frame Application):
1. Femoral Block: A two-ring block or a 5/8th ring is applied to the distal femur using a combination of tensioned fine wires and hydroxyapatite-coated half-pins.
2. Tibial Block: A two-ring block is applied to the proximal tibia.
3. Hinge Placement (The Critical Step): The mechanical hinges connecting the femoral and tibial blocks must accurately replicate the anatomical axis of rotation of the knee.
* Placement: The hinges are typically placed at the level of the femoral epicondyles.
* Error Consequence: If the hinges are placed too anteriorly, the joint will distract during extension. If placed too posteriorly, the joint will compress, leading to severe cartilage necrosis.
4. Distraction Protocol: Distraction is initiated postoperatively at a rate of 1 mm per day (divided into 0.25 mm increments every 6 hours). The rate is adjusted based on patient tolerance and neurovascular monitoring.
Clinical Pearl: While gradual distraction improves the functional position of the arc of motion (e.g., shifting a 40-100 degree arc to a 0-60 degree arc), the total arc of motion often remains essentially unchanged. Patients must be counseled preoperatively regarding this expectation.
THE PERONEAL NERVE: A CRITICAL SURGICAL PITFALL
The most devastating complication in the correction of knee flexion ankylosis is iatrogenic palsy of the common peroneal nerve.
Pathoanatomy of Nerve Injury
The common peroneal nerve is anatomically tethered at the fibular neck as it passes through the fibro-osseous tunnel of the peroneus longus muscle. During the correction of a flexion contracture, the nerve is subjected to significant longitudinal traction.
Unlike the popliteal artery, which has a tortuous course and can accommodate a degree of stretching, the peroneal nerve is highly susceptible to ischemic injury from tension. The literature dictates that extreme caution is indicated when signs of irritation develop along its course. Prolonged or permanent paralysis can result after a flexion contracture has been corrected as little as 20 degrees acutely.
Prophylactic and Management Strategies
- Prophylactic Decompression: In severe contractures undergoing acute release or rapid external fixation correction, a prophylactic release of the common peroneal nerve at the fibular neck should be routinely performed. This involves releasing the fascia of the peroneus longus to untether the nerve.
- Intraoperative Neuromonitoring: Somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) can provide real-time feedback regarding nerve strain during acute correction.
- Postoperative Vigilance: During gradual distraction, the patient's motor function (extensor hallucis longus and tibialis anterior) and sensory distribution (first dorsal webspace) must be assessed multiple times daily.
- Management of Palsy: If a nerve palsy develops during gradual distraction, the frame must be immediately reversed by 5 to 10 degrees until symptoms resolve. Distraction is then halted for several days before resuming at a significantly slower rate (e.g., 0.5 mm/day).
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of the surgical intervention relies heavily on a rigorous, prolonged postoperative rehabilitation protocol. The tendency for recurrence of the flexion contracture is exceptionally high.
Immediate Postoperative Phase
- Pain Management: Adequate analgesia, often utilizing continuous peripheral nerve blocks (e.g., adductor canal block), is essential to allow for early mobilization.
- Positioning: The limb is maintained in maximum achieved extension using a posterior splint or a locked hinged knee brace. Pillows under the knee are strictly prohibited.
Rehabilitation Strategy
- Continuous Passive Motion (CPM): May be utilized early to prevent intraarticular adhesion formation, though its efficacy in maintaining extraarticular length is debated.
- Active and Active-Assisted ROM: Aggressive physiotherapy focusing on quadriceps strengthening is vital. A strong extensor mechanism is the best defense against recurrent flexion contracture.
- Bracing: Patients are typically transitioned to a dynamic extension splint (e.g., Dynasplint) or a custom KAFO to be worn at night for 6 to 12 months postoperatively. The biological remodeling of the lengthened soft tissues takes months, and premature discontinuation of bracing will inevitably lead to relapse.
Long-Term Follow-Up
Patients require close outpatient monitoring. Serial clinical examinations and radiographic assessments are necessary to ensure the maintenance of the mechanical axis and the prevention of recurrent posterior tibial subluxation. In cases managed with external fixation, the frame is removed only when the desired correction is achieved and the soft tissues have adequately adapted, followed immediately by the application of a rigid extension cast or brace to protect the correction during the vulnerable immediate post-frame period.
You Might Also Like