Surgical Management of Osteogenesis Imperfecta: The Sofield-Millar Procedure and Deformity Correction

Key Takeaway
Osteogenesis imperfecta (OI) is a congenital disorder of type I collagen characterized by bone fragility, recurrent fractures, and progressive long-bone deformity. Surgical management primarily involves the Sofield-Millar procedure, utilizing multiple osteotomies and intramedullary rod fixation to realign the mechanical axis and prevent further fractures. Telescoping implants, such as the Bailey-Dubow or Sheffield rods, are preferred in growing children to accommodate longitudinal growth while maintaining continuous internal splintage.
CONGENITAL AFFECTIONS: OSTEOGENESIS IMPERFECTA
Most affections of bone seemingly of congenital origin may respond favorably to surgery. Osteogenesis imperfecta (OI) represents a profound surgical challenge, requiring a deep understanding of altered bone biomechanics, specialized implant selection, and meticulous surgical execution.
Osteogenesis imperfecta is a genetic disorder primarily affecting mesodermal tissues, characterized by abnormal or deficient type I collagen. This structural defect manifests across multiple organ systems, most notably in bone, skin, sclerae, and dentin. Clinically, the disease is often identified by the classic diagnostic triad: blue sclerae, dentinogenesis imperfecta, and generalized osteoporosis in a patient presenting with multiple fragility fractures or progressive bowing of the long bones.
There is no single specific laboratory test that definitively diagnoses all variants of this disease; diagnosis remains largely clinical and radiographic. Multiple wormian bones around the base of the skull are a major radiographic finding, predominantly seen in the congenital type of osteogenesis imperfecta.
Classification and Clinical Presentation
Historically, the classification suggested by Falvo et al. divided the disease into distinct prognostic categories:
* Osteogenesis Imperfecta Congenita: Characterized at birth by multiple fractures, severe bowing of the long bones, short extremities, and profound generalized osteoporosis. In the series by Falvo et al., all patients with the congenital type exhibited dentinogenesis imperfecta, and 92% had blue sclerae.
* Osteogenesis Imperfecta Tarda Type 1: Differentiated by the presence of bowing of the long bones. These patients experience progressively increasing deformities that can cause a severe deterioration in functional activity, often transitioning them from walkers to sitters, and from braceable to unbraceable.
* Osteogenesis Imperfecta Tarda Type 2: Characterized by an absence of long-bone bowing, representing a milder form of the disease.
Fractures may be present at birth in both tarda types, although this is exceedingly rare in tarda type 2. Ultimately, only two characteristics are universally present in all patients with osteogenesis imperfecta: recurrent fractures and generalized osteoporosis.
Clinical Pearl: Developmental milestones are highly predictive of future ambulatory status. Daly et al. surveyed 59 children with OI and found that independent sitting by age 10 months was a strong predictor of walking as the primary means of mobility (75% attainment). Conversely, of those who failed to achieve sitting by 10 months, only 18% ever achieved independent walking.
Medical Management and Preoperative Optimization
Modern management of OI requires a multidisciplinary approach. Zeitlin et al. noted that the administration of bisphosphonates significantly reduces osteoclast-mediated bone resorption. Intravenous pamidronate has been shown to decrease bone pain, lower the incidence of fractures, increase bone mineral density, and improve the level of ambulation with minimal side effects. Radiographically, an increase in the size of vertebral bodies and thickening of cortical bone are frequently observed following bisphosphonate therapy.
Surgical Warning: Patients must be rigorously examined for scoliosis before any extremity surgical procedures are undertaken. Widmann et al. noted that thoracic scoliosis greater than 60 degrees has severe adverse effects on pulmonary function in patients with OI. This restrictive lung disease significantly increases perioperative pulmonary morbidity and anesthetic risk.
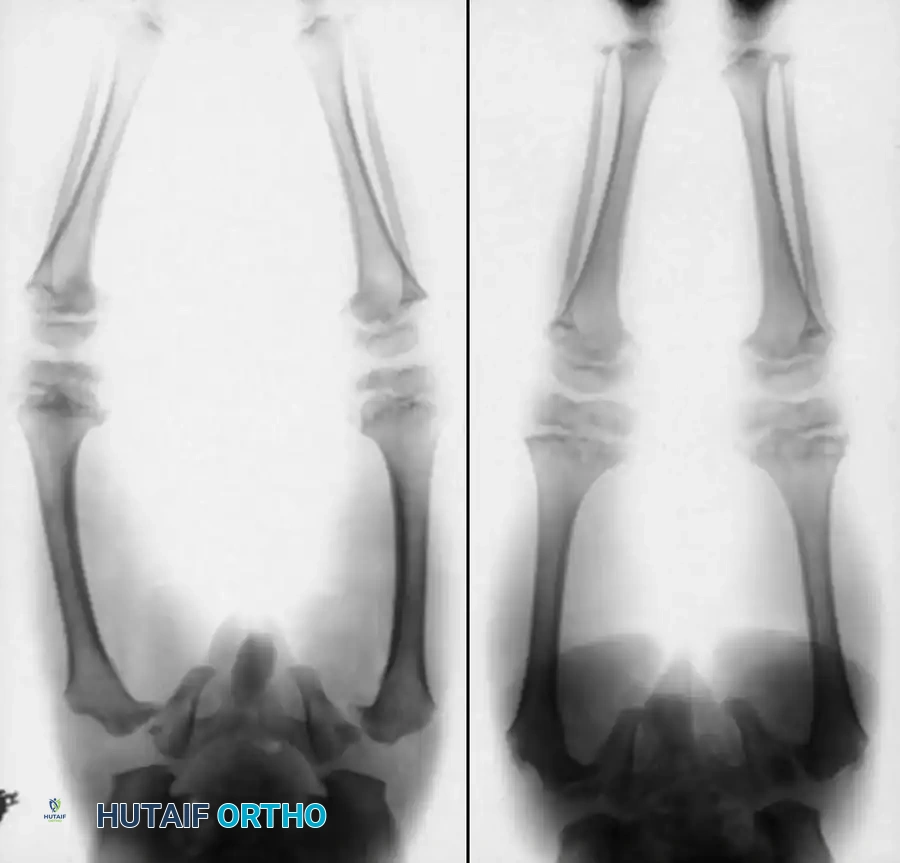
Preoperative radiographic assessment demonstrating severe bowing and osteopenia characteristic of osteogenesis imperfecta, necessitating comprehensive surgical planning.
BIOMECHANICS AND SURGICAL INDICATIONS
Orthopaedic surgery is most heavily involved with addressing the bowing of the long bones, particularly in osteogenesis imperfecta tarda type 1. Progressive deformity alters the mechanical axis, creating massive bending moments that inevitably lead to recurrent fractures.
The primary goals of surgical intervention are:
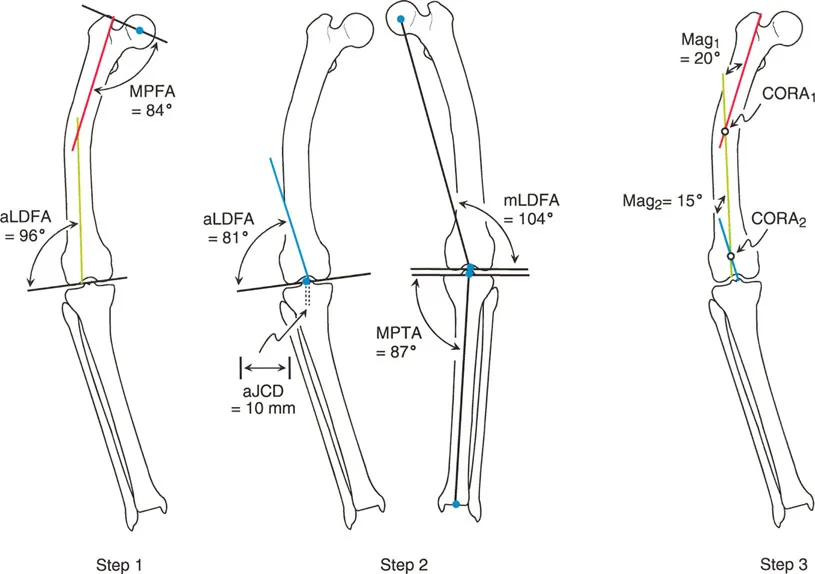
1. Correction of angular deformity to restore the mechanical axis.
2. Internal splintage of the entire long bone to prevent recurrent fractures.
3. Facilitation of upright mobility and bracing.
Healing of fractures and osteotomies in OI is usually satisfactory in terms of union time, although the healed bone is biomechanically no stronger than the original woven bone. Hyperplastic callus is occasionally seen after fractures and osteotomies and should not be mistaken for osteosarcoma.
While alternative methods exist—such as the Ilizarov method of lengthening reported by Ring et al. (which yielded an average angular correction of 23 degrees and 6.6 cm of length, but carried a high rate of 18 major complications in six patients)—intramedullary fixation remains the gold standard. Conversely, for adult patients with severe joint malalignment secondary to periarticular deformity, Papagelopoulos and Morrey reported favorable results with total hip and total knee arthroplasties.

Intraoperative fluoroscopy is mandatory to assess the medullary canal, which is often distorted and narrower than anticipated based on plain radiographs.
IMPLANT SELECTION: ELONGATING VS. NON-ELONGATING RODS
The fundamental challenge in pediatric OI surgery is that the bone grows longitudinally, but the implant does not. If a standard (non-elongating) rod is used, the bone will rapidly grow beyond the end of the nail (usually distally in the lower extremities). The unsupported bone extending beyond the nail tends to angulate, and the nail itself tends to cut out, leading to a "growing away" fracture.
Telescoping (Elongating) Rods
Bailey and Dubow revolutionized treatment by introducing a telescoping medullary rod with small flanges (T-pieces) at the distal and proximal ends that anchor within the bony epiphysis. As the child grows, the rod elongates, allowing the entire length of the diaphysis to remain reinforced for several years.
Marafioti and Westin reported that the incidence of reoperation was decreased 3.5 times when using telescoping rods compared to standard nails. However, complication rates remain high. Gamble et al. reported a 69% complication rate for Bailey-Dubow rods, most commonly involving migration or disengagement of the T-piece.
Surgical Pearl (Gamble and Janus Recommendations): To avoid loosening of the T-junction of the obturator portion, score the T-piece before its insertion into the sleeve, or stoutly crimp the sleeve after insertion. Place the T-piece below the subchondral bone or periosteal surface, but not so deep that it migrates into the medullary canal. After insertion, turn the T-piece 90 degrees to help prevent backout.

Fig. 29-57: Multiple osteotomies of the femur and tibia with the insertion of Bailey-Dubow elongating intramedullary rods in a patient with osteogenesis imperfecta. Note the epiphyseal anchoring of the T-pieces.
Modern Expanding Systems
Wilkinson et al. treated 74 bones using the Sheffield Expanding IM rod system, developed to mitigate the high complication rates of earlier designs. They found no evidence of physeal damage and reported a significantly lower complication rate requiring rod exchange (7%).
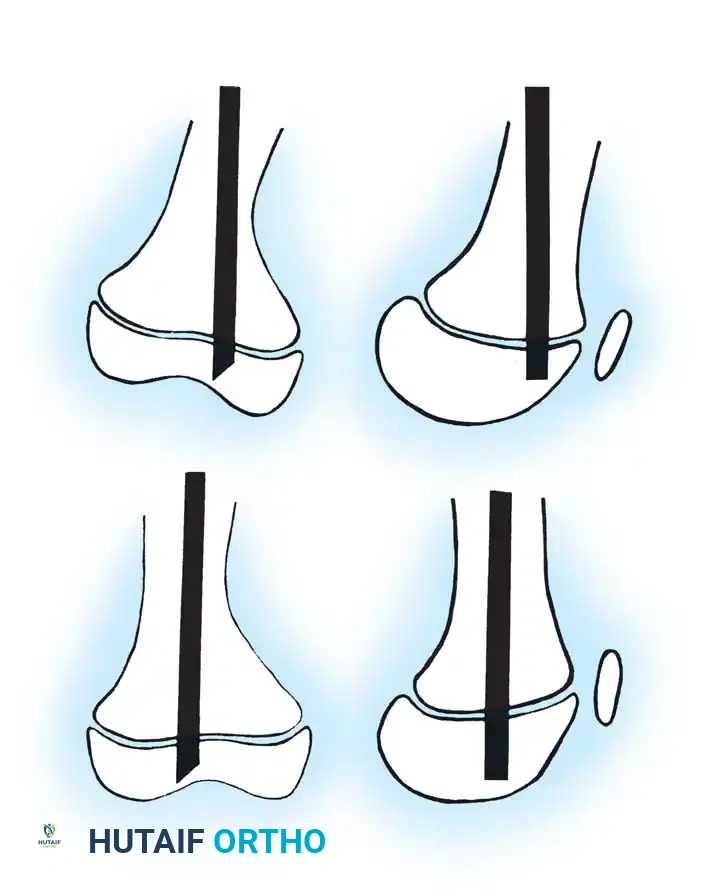
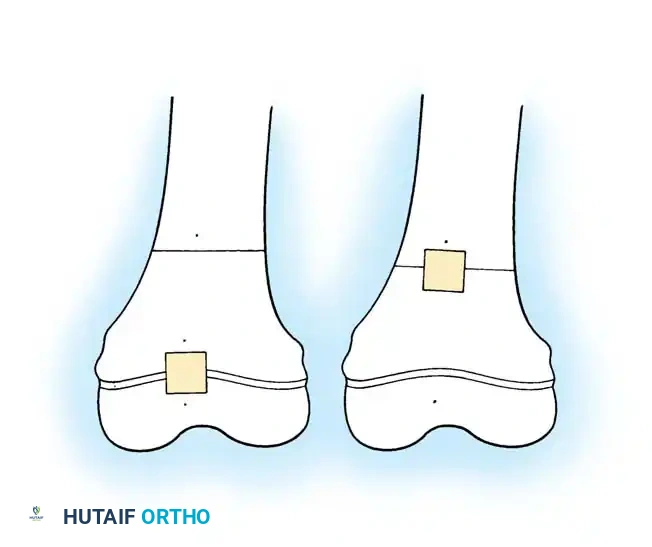
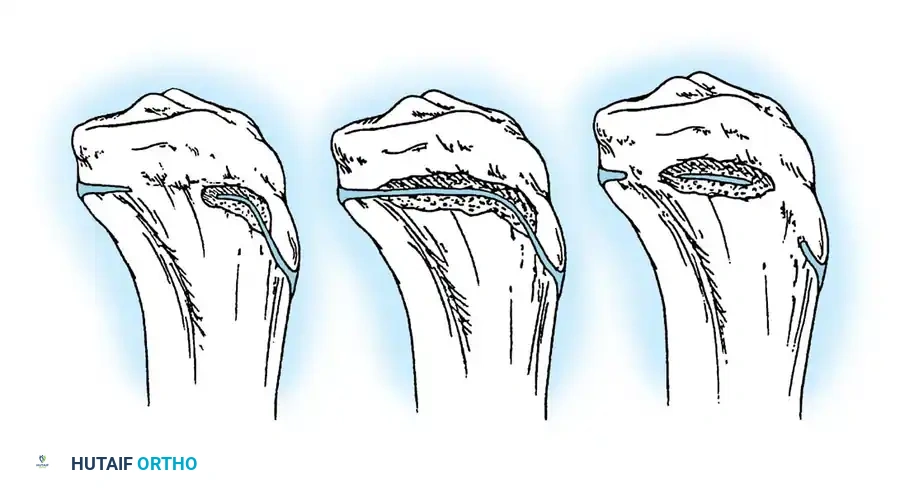
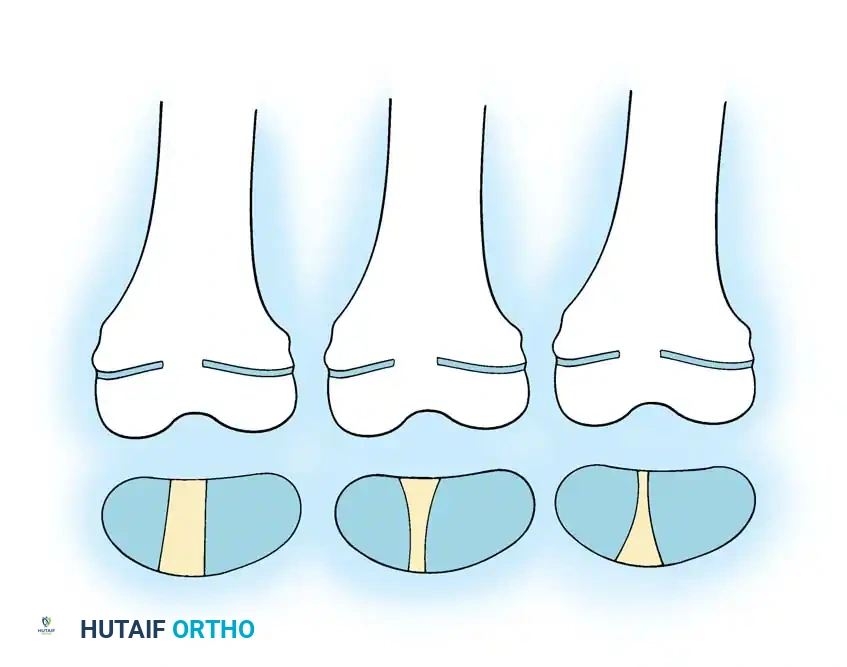
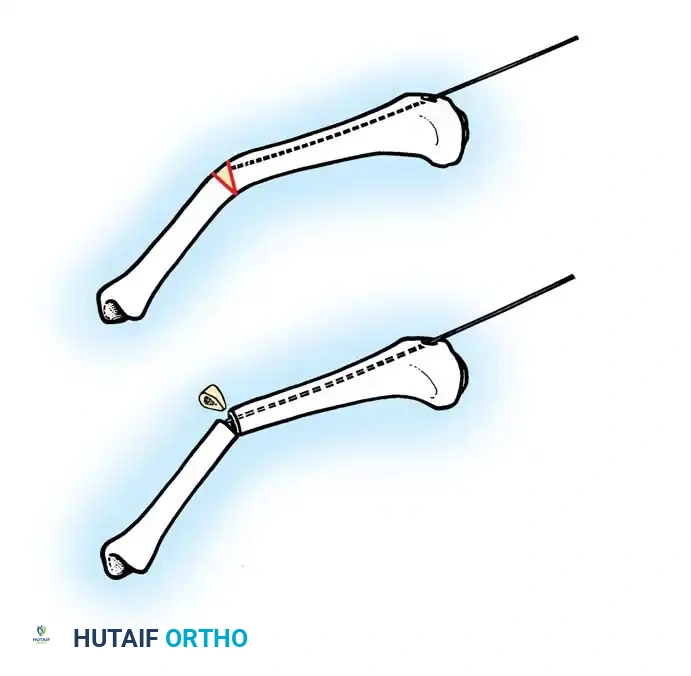
Fig. 29-56: Medullary rod positioning in osteotomies for osteogenesis imperfecta. (A) Incomplete reduction with poor position of the rod; it is not centrally placed and is anterior in the epiphysis. (B) Complete reduction of end fragments and excellent central positioning of the medullary rod.
THE SOFIELD-MILLAR PROCEDURE: MULTIPLE OSTEOTOMIES AND MEDULLARY NAILING
The most successful surgical method for treating the severe deformities of OI is based on the landmark work of Sofield and Millar. This technique involves multiple osteotomies, realignment of the fragmented segments (the "shish kebab" technique), and medullary nail fixation.
Preoperative Planning
Chotigavanichaya et al. emphasized the critical importance of determining the correct rod diameter intraoperatively. Preoperative radiographs are notoriously ineffective at predicting rod diameter due to severe bony distortion, often overestimating the medullary canal size. Repeat fluoroscopic examinations in multiple planes during surgery are mandatory.
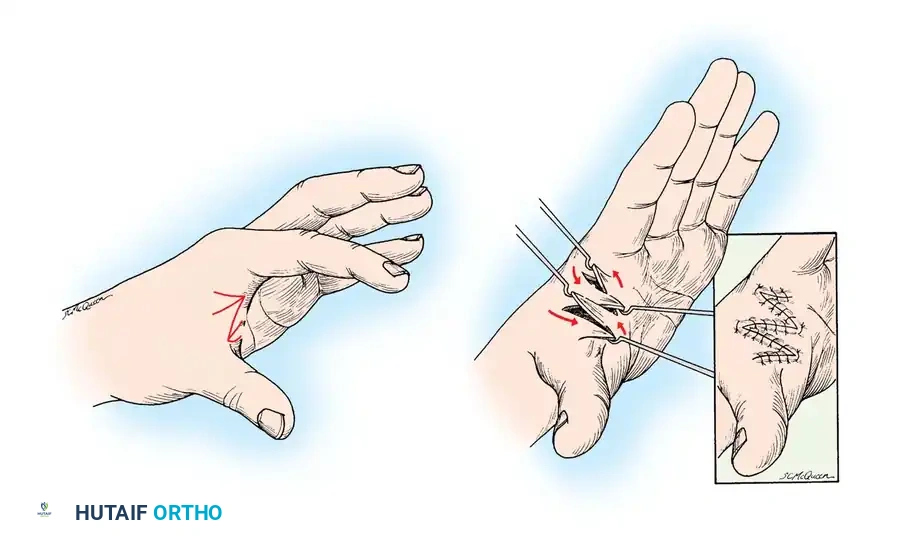
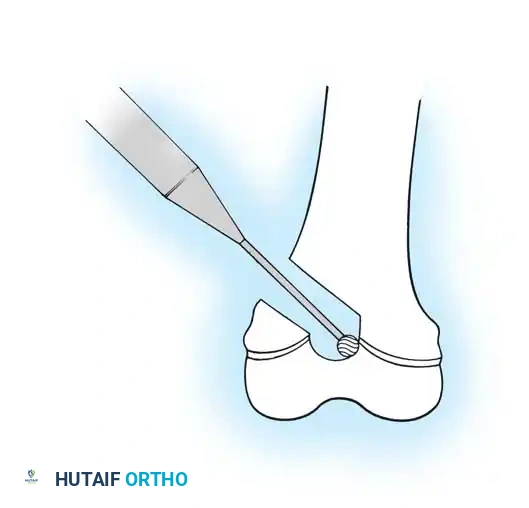
Diagrammatic representation of the initial approach and periosteal elevation required before performing the corrective osteotomies.
Technique 29-20: Sofield and Millar (Modified)
Step 1: Exposure and Periosteal Elevation
Expose the entire shaft of the bone subperiosteally. In OI, the periosteum is often thickened and highly osteogenic; preserving it as an intact tube is critical for the incorporation of the bone fragments and the formation of a new cortical shell.
The diaphysis is exposed subperiosteally. Care must be taken to maintain the integrity of the periosteal sleeve, which will serve as the biological envelope for the realigned fragments.
Step 2: Metaphyseal Osteotomies and Diaphyseal Resection
Make a transverse osteotomy through the proximal metaphysis and another through the distal metaphysis. Carefully remove the entire diaphyseal shaft from the wound.
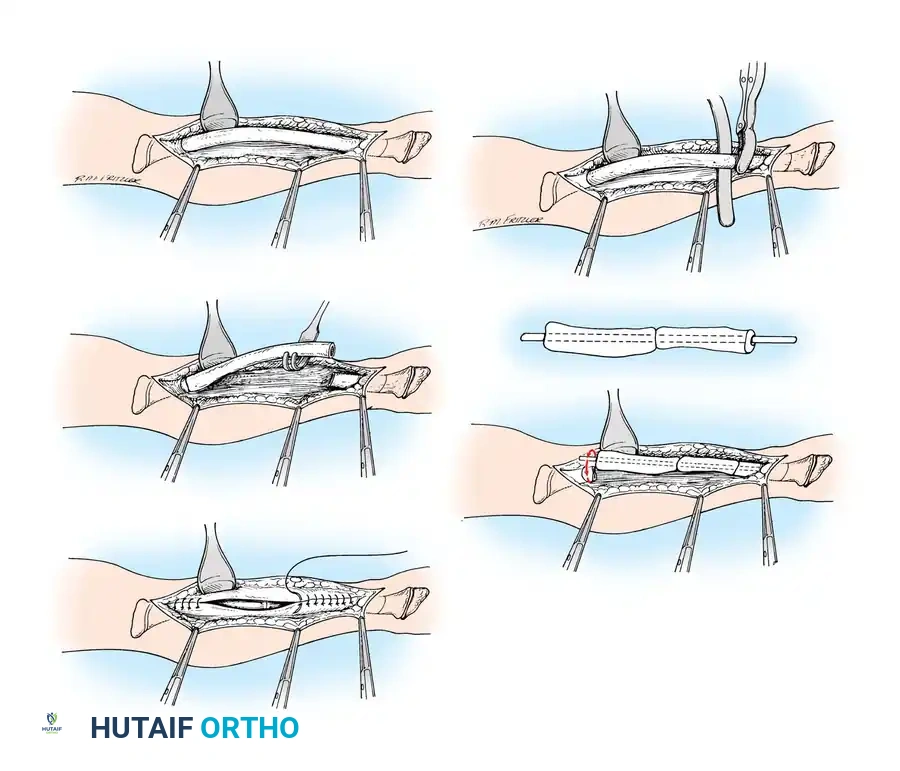
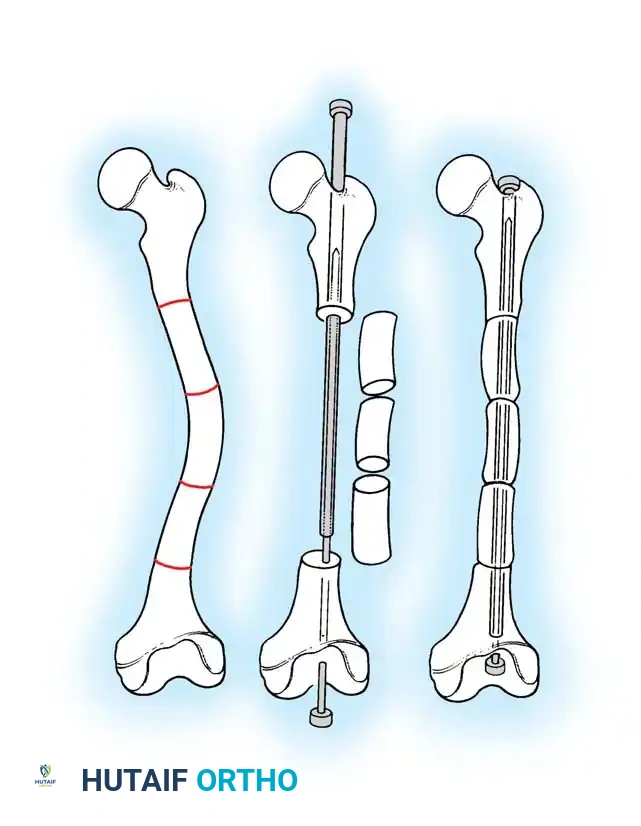
Fig. 29-58 A-E: Technique for fragmentation and realignment of bone. The diaphysis is removed, sectioned, and threaded onto the intramedullary nail to correct the bowing deformity.
Step 3: Fragmentation and Realignment
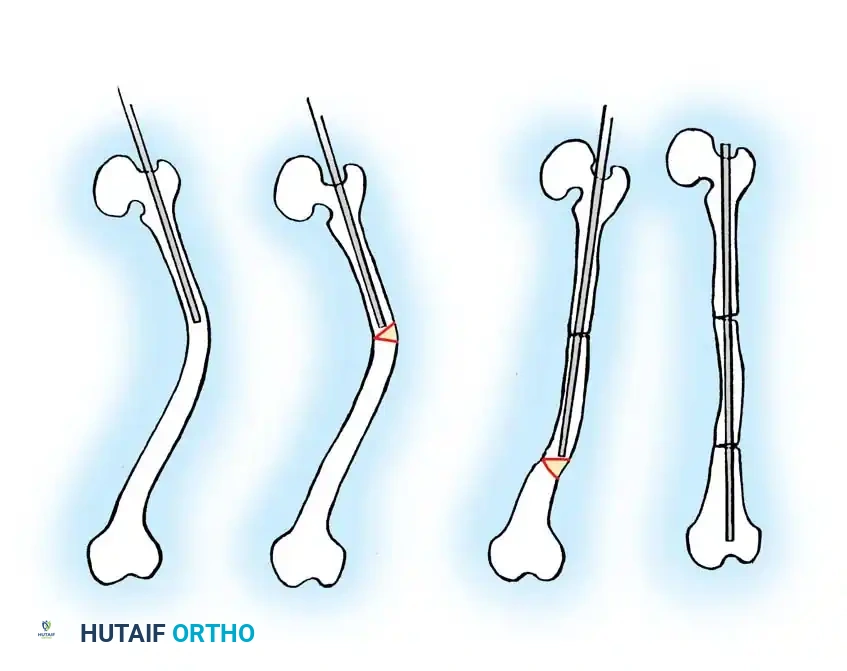
Study the excised shaft to determine how many times it must be osteotomized so that its curved segments can be threaded onto a perfectly straight medullary nail. Commonly, three or four osteotomies are required. Skillfully shift, reverse, and rotate the fragments end-to-end as necessary to align them concentrically on the straight nail.
Pitfall: Li et al. noted that performing more than three osteotomies significantly prolongs the time to union and leads to severe thinning of the bone. Modern modifications advocate for minimal incisions and limited osteotomies at the apex of the deformity to preserve vascularity whenever possible.
The excised diaphyseal segment is sectioned into multiple cylindrical fragments. These fragments will be rotated to neutralize the anatomical bow.
Threading the bone segments onto the intramedullary rod. The fragments act as biological spacers over the load-sharing implant.
Step 4: Nail Insertion and Epiphyseal Fixation
After the nail has been inserted through the fragments, its distal end must lie in the medullary canal near the distal physis, and its proximal end near the proximal physis.
Tiley and Albright recommended routine central placement of the rod across the physis to add length to the rod and postpone the problem of the rod becoming too short as the child grows. Sofield and Millar reported no disturbances in growth when a smooth medullary nail penetrated the physis centrally. We routinely modify the original technique to extend the medullary nails into the bony epiphysis, resting just short of the subchondral bone plate.
Fluoroscopic confirmation of rod trajectory. The rod must be perfectly centralized within the epiphysis to prevent eccentric physeal tethering or joint penetration.
Final seating of the intramedullary rod. The fragments are compressed together within the periosteal sleeve.
Step 5: The Williams Modification for the Tibia
For the tibia, maximizing the length of the medullary rod is paramount. Williams reported a technique in which an extension is screwed onto the distal end of the rod and pushed through the distal tibia, exiting out the sole of the foot. After the tibial fragments are realigned, the nail is reinserted in a retrograde fashion until the distal end lies just proximal to the articular surface of the ankle joint. The extension is then unscrewed, leaving the rod extending maximally into the distal tibial epiphysis without violating the joint space.

The Williams technique for distal tibial fixation, utilizing a retrograde insertion method through the plantar aspect of the foot to maximize epiphyseal purchase.
Radiographic appearance of the tibia following the Williams modification, demonstrating excellent distal epiphyseal seating of the rod.
Step 6: Closure and Postoperative Immobilization
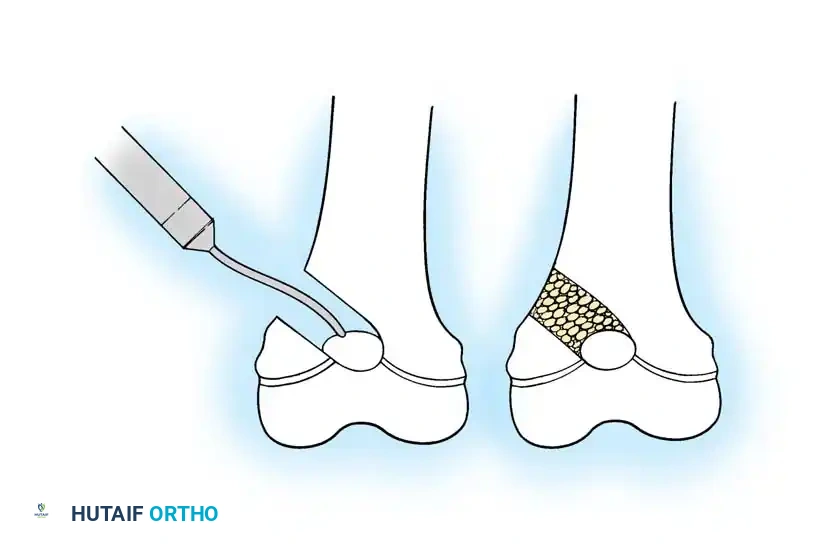
When the cortex of the bone is extremely thin, homogeneous allografts may be added. Meticulously suture the thick periosteum over the realigned bone fragments to create a closed biological tube. Close the subcutaneous tissues and skin in a routine manner.

Postoperative radiograph demonstrating the realigned femur and tibia. The mechanical axis has been restored, and the implants span the entire length of the long bones.
Long-term follow-up showing incorporation of the osteotomized segments and remodeling of the diaphysis around the intramedullary implants.
Semiclosed and Minimally Invasive Techniques
In infants with severe forms of OI, extensive open fragmentation can be highly morbid. Ryöppy et al. described treating young children with closed or semiclosed intramedullary stabilization using nonexpandable rods. They performed closed osteoclasis or a semiclosed technique with a limited open operation at the site of maximal angulation.
This minimally invasive approach is preferred in infants because it saves operative time, reduces surgical trauma and blood loss, and allows several bones to be stabilized in a single anesthetic session. Early stabilization with simple nonexpandable implants is justified; later, around the age of 4 years, these can be exchanged for telescoping nails once the medullary canal is large enough to accept them.
Minimally invasive percutaneous osteoclasis and rod insertion in an infant. This technique minimizes blood loss and preserves the delicate periosteal blood supply.
COMPLICATIONS AND SALVAGE STRATEGIES
Despite meticulous technique, the complication rate in OI surgery remains high due to the inherently poor quality of the host bone.
- Rod Migration: The most common complication for both elongating and non-elongating rods. Proximal migration into the gluteal musculature or distal migration into the knee joint requires prompt revision. Using rods with epiphyseal anchoring flanges (Bailey-Dubow, Fassier-Duval) reduces this risk but introduces the risk of T-piece disengagement.
- Nonunion: More common if the periosteum is severely damaged during exposure or if more than three or four osteotomies are performed (Li et al.). Treatment requires revision with bone grafting.
- Hyperplastic Callus: An exaggerated, tumor-like biological response to fracture or osteotomy, unique to OI. It presents as a massive, warm, painful swelling. It is self-limiting but can cause significant deformity and must be differentiated from osteosarcoma via clinical history and radiographic appearance.

Complication: Distal migration of an intramedullary rod penetrating the articular surface. This requires immediate revision and exchange to a properly sized, epiphyseal-anchored implant.
Rehabilitation and Outcomes
Because of frequently frail bone, disabling joint deformities, and fractures that preclude ambulation, postoperative rehabilitation is as critical as the surgery itself. Gerber et al. described a comprehensive rehabilitation program utilizing custom long-leg bracing (KAFOs) that results in a high level of functional activity with an acceptable level of fracture risk.
Ultimately, the Sofield-Millar procedure, combined with modern telescoping implants and bisphosphonate therapy, offers the best chance for children with severe osteogenesis imperfecta to achieve upright
You Might Also Like