Mastering Orthopedic Deformity Correction: Static Alignment to Dynamic Gait Biomechanics
Key Takeaway
Orthopedic deformity correction requires mastering both static radiographic analysis, including Paley's principles of alignment and osteotomy rules, and dynamic gait biomechanics. Analyzing the Ground Reaction Vector helps identify compensatory patterns and prevent surgical errors, ensuring precise correction of complex deformities like knee flexion.
Introduction to Orthopedic Gait Biomechanics and Deformity Correction
In the realm of complex limb reconstruction and deformity correction, mastering static radiographic analysis is only the foundational step. Identifying the Center of Rotation of Angulation, measuring the Mechanical Axis Deviation, and calculating joint orientation angles are critical, but the true art of orthopedic surgery lies in understanding Orthopedic Gait Biomechanics and dynamic lever arm considerations.
When a patient moves, static deformities become dynamic challenges. The human body is a master of compensation, constantly adjusting adjacent joints, altering muscle firing patterns, and shifting the spine to maintain a functional center of gravity and forward progression. As a surgeon in training, you must learn to look beyond the static radiograph and analyze the Ground Reaction Vector during the gait cycle. Failing to recognize a compensatory gait pattern can lead to disastrous surgical outcomes, such as correcting a compensatory deformity while leaving the primary pathology untouched.
This comprehensive masterclass dissects the biomechanical implications of knee flexion deformities, recurvatum, hip contractures, rotational malalignment, and leg length discrepancies. The entire discussion is framed through the lens of advanced orthopedic principles pioneered by Dr. Dror Paley, ensuring you possess the analytical tools required for precise, dynamic deformity correction.
Core Principles of Static Alignment and Paley Deformity Analysis
Before diving into dynamic gait, the surgeon must have absolute command over static lower extremity alignment. Dr. Dror Paley revolutionized deformity correction by standardizing the nomenclature and mathematical approach to limb alignment. Understanding these principles is non negotiable for any orthopedic surgeon performing osteotomies.
Mechanical Axis Deviation and Joint Orientation Angles
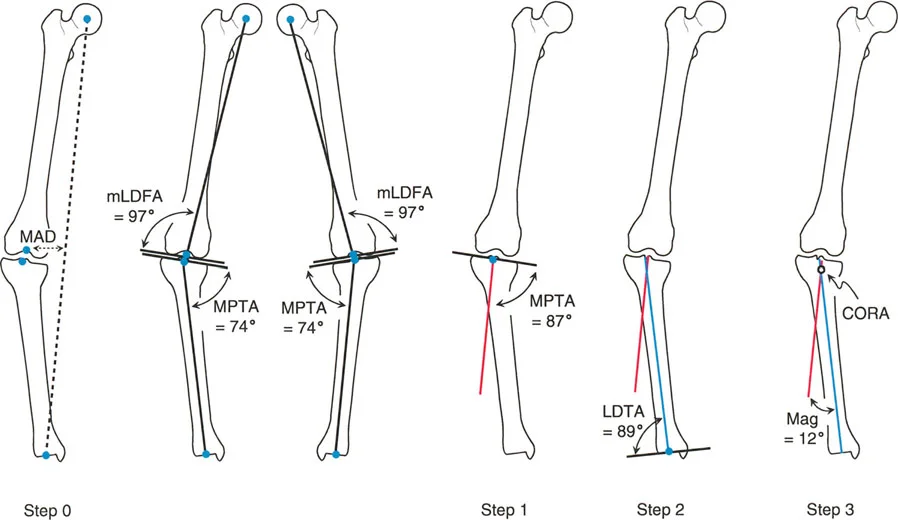
The mechanical axis of the lower extremity is a line drawn from the center of the femoral head to the center of the ankle joint. In a normally aligned limb, this line passes slightly medial to the center of the knee joint. The distance from the center of the knee to this mechanical axis line is the Mechanical Axis Deviation. A medial shift indicates a varus deformity, while a lateral shift indicates a valgus deformity.
To determine the source of the Mechanical Axis Deviation, we rely on Joint Orientation Angles. These angles define the relationship between the mechanical or anatomic axes of the long bones and their respective joint lines in both the coronal and sagittal planes.
| Angle Abbreviation | Full Name | Normal Range | Plane |
|---|---|---|---|
| mLDFA | Mechanical Lateral Distal Femoral Angle | 85 to 90 degrees | Coronal |
| MPTA | Medial Proximal Tibial Angle | 85 to 90 degrees | Coronal |
| JLCA | Joint Line Convergence Angle | 0 to 2 degrees | Coronal |
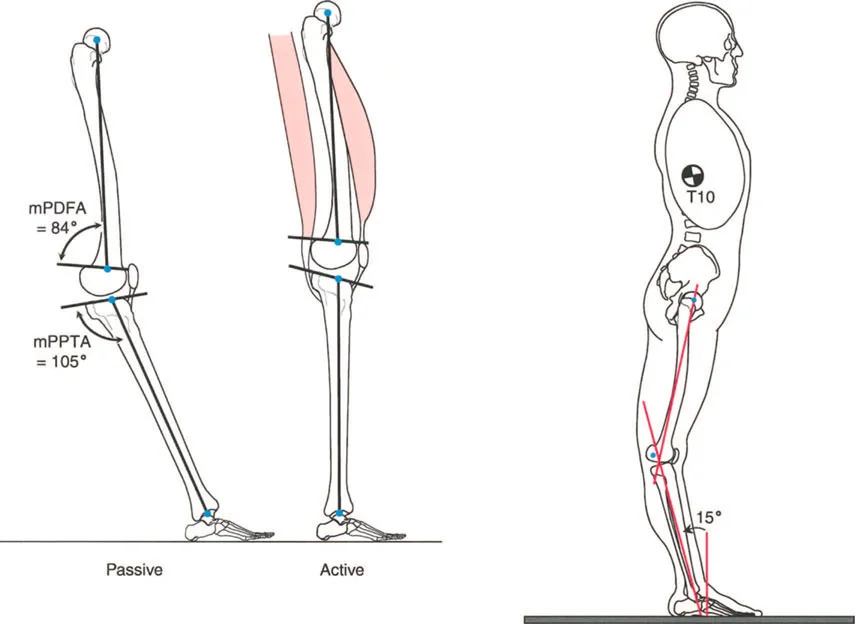
| mPDFA | Mechanical Posterior Distal Femoral Angle | 79 to 87 degrees | Sagittal |
| mPPTA | Mechanical Posterior Proximal Tibial Angle | 77 to 84 degrees | Sagittal |
| LDTA | Lateral Distal Tibial Angle | 86 to 92 degrees | Coronal |
Center of Rotation of Angulation and Osteotomy Rules
Once the abnormal bone is identified via Joint Orientation Angles, the surgeon must locate the apex of the deformity, known as the Center of Rotation of Angulation. The Center of Rotation of Angulation is the intersection of the proximal and distal mechanical or anatomic axis lines of the deformed bone.
Dr. Paley established three fundamental Osteotomy Rules that dictate the geometric outcome of deformity correction. Mastering these rules ensures that your osteotomy corrects angular deformity without inducing unwanted iatrogenic translation.
- Paley Osteotomy Rule 1
When the osteotomy and the axis of correction hinge are both placed at the Center of Rotation of Angulation, the angular deformity is corrected with perfect collinear realignment of the proximal and distal axes. No translation occurs. - Paley Osteotomy Rule 2
When the osteotomy is performed at a level different from the Center of Rotation of Angulation, but the axis of correction hinge remains at the Center of Rotation of Angulation, the axes will realign collinearly. However, the bone ends at the osteotomy site will undergo an expected, calculated translation. - Paley Osteotomy Rule 3
When both the osteotomy and the axis of correction hinge are placed outside the Center of Rotation of Angulation, the proximal and distal axes will become parallel but will not be collinear. This results in an iatrogenic translation deformity that alters the mechanical axis.
Clinical Pearls for Static Alignment
- Always obtain full length standing weight bearing radiographs. Supine films are useless for evaluating Mechanical Axis Deviation.
- A Joint Line Convergence Angle greater than 2 degrees suggests ligamentous laxity or cartilage loss, which will artificially exaggerate the apparent bony deformity.
- Never plan a coronal plane correction without evaluating the sagittal plane. Deformities are inherently three dimensional.
Ground Reaction Vector Dynamics in the Sagittal Plane
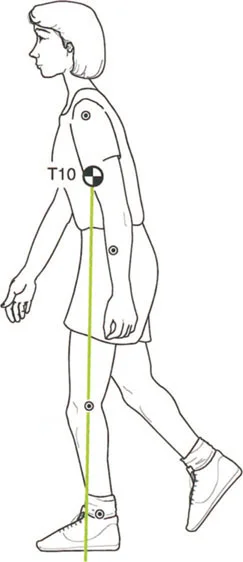
With static alignment defined, we must transition to the dynamic environment. The Ground Reaction Vector represents the magnitude and direction of the force exerted by the ground on the body during contact. Its relationship to the joint centers of the hip, knee, and ankle dictates the external moments applied to those joints, which the internal muscular system must counteract.
Normal Gait Cycle Biomechanics
During the normal stance phase of gait, the Ground Reaction Vector shifts dynamically. At initial contact or heel strike, the Ground Reaction Vector is posterior to the ankle, posterior to the knee, and anterior to the hip. This creates a plantarflexion moment at the ankle, a flexion moment at the knee, and a flexion moment at the hip.
As the body progresses over the planted foot into mid stance, the ankle plantar flexors specifically the gastrocsoleus complex contract to control tibial advancement. This dynamic action pulls the femur posteriorly, extending the knee and driving the Ground Reaction Vector anterior to the knee joint center.
Compensatory Mechanisms in Pathologic Gait
Because the Ground Reaction Vector is anterior to the knee during normal mid stance, the knee is mechanically stabilized in extension without requiring active quadriceps contraction. This is a highly energy efficient state. When structural deformities alter this vector, the body must deploy compensatory mechanisms. These compensations usually manifest as abnormal pelvic tilt, exaggerated trunk sway, or secondary joint contractures designed to artificially realign the Ground Reaction Vector with the joint centers.
Biomechanics and Management of Knee Fixed Flexion Deformity
The knee joint is a highly constrained hinge that relies heavily on the sagittal plane for energy efficient locomotion. Any fixed deformity in this plane drastically alters the Ground Reaction Vector, forcing the muscular system to work overtime to prevent collapse.
Ground Reaction Vector Inversion in Flexion Deformities
A Fixed Flexion Deformity of the knee is one of the most mechanically demanding conditions a patient can endure. In the presence of a knee Fixed Flexion Deformity, the normal biomechanics of mid stance are inverted. The Ground Reaction Vector is forced posterior to the knee joint center, creating a relentless, continuous flexion moment.
To prevent the knee from buckling under the weight of the body, the quadriceps must fire continuously throughout the stance phase. This eliminates the energy efficient resting phase of normal gait, leading to rapid muscular fatigue and vastly increased metabolic demand.
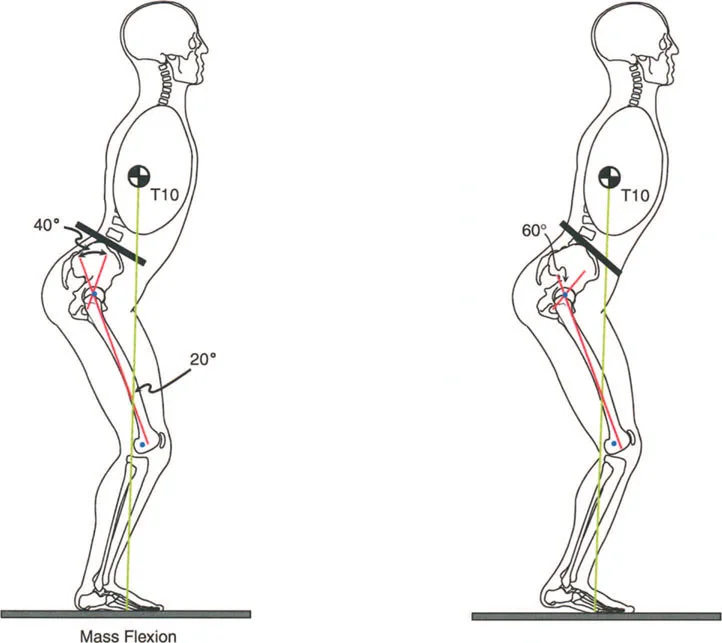
Quadriceps Strength and Anterior Trunk Lean Compensations
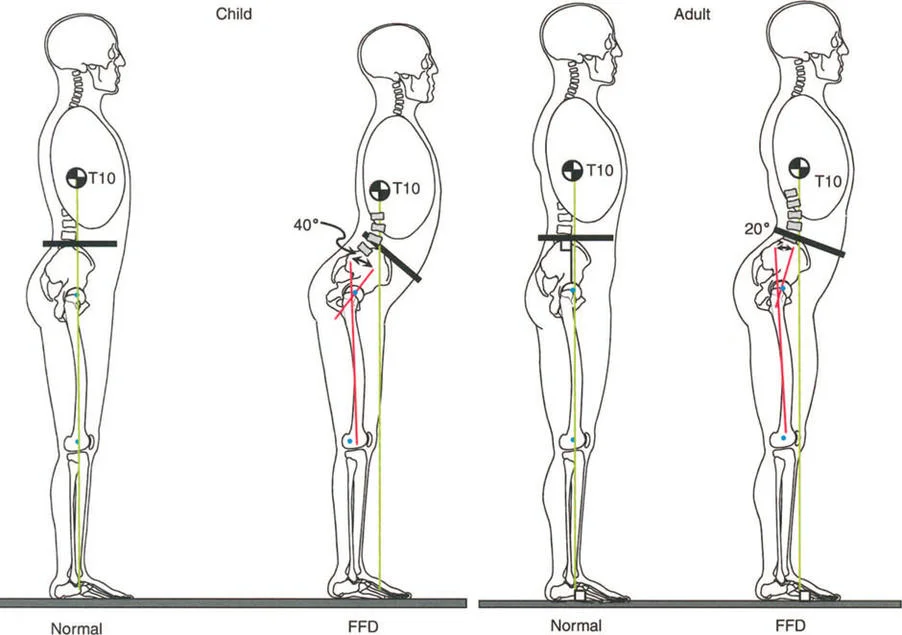
Consider a patient with a severe knee Fixed Flexion Deformity measuring 40 degrees. To position the body weight line anterior to the knee joint line, the body must compensate. This is typically achieved by utilizing 20 degrees of ankle dorsiflexion combined with compensatory hip flexion. Despite maxing out ankle dorsiflexion at 20 degrees, the patient is often forced into a toe walking posture.
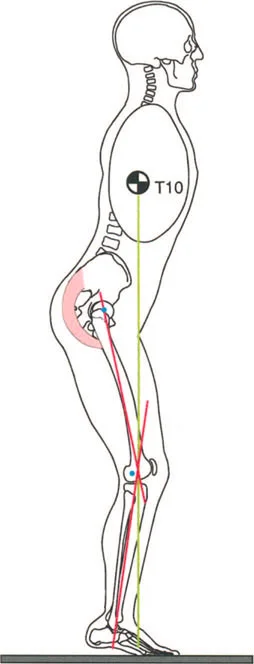
Patients with bilateral knee Fixed Flexion Deformities greater than 20 degrees and stiff ankles cannot achieve a toe to toe gait. Instead, they resort to profound hip flexion coupled with an anterior lean of the trunk. This compensatory mechanism allows them to place the foot flat on the ground during the stance phase, but it exponentially increases the workload on the gluteus maximus.
The most critical clinical consideration when evaluating a knee Fixed Flexion Deformity is quadriceps strength. Because the Ground Reaction Vector is posterior to the knee, the quadriceps are the only defense against collapse. If a patient has a knee Fixed Flexion Deformity combined with a lack of ankle dorsiflexion or quadriceps weakness such as in post polio syndrome, the condition is severely disabling.
Patients with weak quadriceps and a knee Fixed Flexion Deformity have no alternative but to walk with a severe, exaggerated anterior trunk lean. By throwing their upper body mass forward, they artificially force the Ground Reaction Vector anterior to the knee joint, achieving mechanical stability during the stance phase without relying on the weakened quadriceps.
Patellofemoral Joint Consequences and Osteoarthritis
Maintaining a flexed knee posture while continuously firing the quadriceps throughout the stance phase drastically increases the compressive forces across the patellofemoral joint.
Over time, this dynamic overload leads to severe anterior knee pain, cartilage degradation, and premature patellofemoral osteoarthritis. From a surgical perspective, correcting the sagittal plane deformity via a distal femoral extension osteotomy or a proximal tibial flexion osteotomy is paramount to offloading the patellofemoral compartment and restoring normal Ground Reaction Vector kinematics.
Clinical Pearls for Knee Flexion Deformities
- Always assess quadriceps strength before undertaking deformity correction. A patient relying on a flexion contracture for stability may decompensate if the joint is fully extended without adequate muscle control.
- Differentiate between bony deformity and soft tissue contracture. Bony deformity requires osteotomy, while soft tissue contracture may require posterior capsular release or hamstring lengthening.
- Evaluate ankle dorsiflexion. Correcting a knee Fixed Flexion Deformity in the presence of a fixed equinus contracture will result in a severe recurvatum thrust during gait.
Biomechanics and Management of Knee Recurvatum
While Fixed Flexion Deformities cause massive energy expenditure, recurvatum or hyperextension presents a different set of biomechanical challenges. Recurvatum deformity of the knee can originate from both structural bony abnormalities and soft tissue incompetence.
Bony Versus Ligamentous Etiologies of Recurvatum
Recurvatum can be classified into three primary sources based on Paley analysis.
First is bony deformity of the distal femur, identified by an abnormal mechanical Posterior Distal Femoral Angle.
Second is bony deformity of the proximal tibia, identified by an abnormal mechanical Posterior Proximal Tibial Angle.
Third is ligamentous or capsular laxity of the posterior knee joint, often involving the posterior cruciate ligament or the posterolateral corner.
Interestingly, unlike Fixed Flexion Deformities, recurvatum deformities do not always cause immediate, obvious gait deviations in patients with normal muscle strength. During a normal gait cycle, the knee does not fully extend. Maximum knee extension during walking is actually approximately 5 degrees of flexion at heel strike. Anteroposterior control of the knee is dynamically managed by the coordinated co contraction of the hamstrings and quadriceps. Therefore, a patient with a structural recurvatum deformity can still walk with 5 degrees of knee flexion at heel strike and undergo the expected flexion up to 20 degrees during initial stance.
Muscular Weakness and Snapping Recurvatum
However, recurvatum becomes highly problematic and often serves as a necessary compensatory mechanism in the presence of muscular weakness.
When patients exhibit hamstring weakness, they develop a snapping recurvatum during initial stance. Because the hamstrings cannot decelerate the extending tibia as the foot strikes the ground, the knee snaps violently into hyperextension, stretching the posterior capsule and eventually leading to severe joint degeneration.
Conversely, in the presence of quadriceps weakness, patients intentionally use recurvatum to lock the knee in hyperextension. By driving the knee backward, they place the Ground Reaction Vector far anterior to the knee joint center. This creates a massive extension moment, allowing them to maintain stability and bear weight on the limb without needing active quadriceps contraction. Correcting this compensatory recurvatum without addressing the underlying quadriceps weakness will cause the patient to lose their ability to walk, as the knee will buckle uncontrollably.
Advanced Sagittal Plane Deformity Planning
Executing a successful correction requires meticulous adherence to Paley principles and a systematic approach to preoperative planning. The integration of static radiographic data with dynamic gait analysis forms the foundation of the surgical blueprint.
Step by Step Preoperative Radiographic Analysis
- Obtain Dedicated Sagittal Imaging
Acquire a true lateral radiograph of the entire femur and tibia. The condyles must be perfectly superimposed to accurately measure the mechanical Posterior Distal Femoral Angle and mechanical Posterior Proximal Tibial Angle. - Establish the Mechanical Axes
Draw the mechanical axis of the femur from the center of the femoral head to the center of the knee. Draw the mechanical axis of the tibia from the center of the knee to the center of the ankle. - Measure Joint Orientation Angles
Calculate the mechanical Posterior Distal Femoral Angle and mechanical Posterior Proximal Tibial Angle. Compare these values to the normative data table provided earlier to isolate the bone responsible for the deformity. - Locate the Center of Rotation of Angulation
Extend the proximal and distal mechanical axes of the deformed bone until they intersect. This intersection point is the Center of Rotation of Angulation. - Determine the Magnitude of Correction
Measure the angle between the intersecting axes. This represents the exact degree of angular correction required to restore normal sagittal alignment.
Applying Paley Osteotomy Rules to the Sagittal Plane
When addressing a bony recurvatum deformity of the proximal tibia characterized by an abnormally high mechanical Posterior Proximal Tibial Angle, the surgeon typically plans an anterior opening wedge osteotomy.
To adhere to Paley Osteotomy Rule 1, the osteotomy and the hinge must be located at the Center of Rotation of Angulation. In the proximal tibia, the Center of Rotation of Angulation is often located near the joint line. Performing an osteotomy directly at the joint line is impossible without violating the articular surface. Therefore, the surgeon must utilize Paley Osteotomy Rule 2. The osteotomy is made distal to the Center of Rotation of Angulation at the tibial tubercle, but the axis of correction hinge remains at the Center of Rotation of Angulation. This results in the expected collinear realignment of the mechanical axis, alongside a calculated anterior translation of the distal fragment, which must be accommodated during fixation.
Biomechanical Impact of Hip Contractures and Rotational Malalignment
The lower extremity is a linked kinetic chain. Deformities at the knee or ankle rarely exist in isolation. Proximal contractures and rotational malalignments drastically alter the Ground Reaction Vector and must be factored into the comprehensive deformity correction plan.
Hip Flexion Contractures and Pelvic Tilt
Hip flexion contractures are insidious deformities that profoundly alter sagittal plane balance. During normal terminal stance, the hip must extend to approximately 10 to 15 degrees to allow the body to progress over the trailing limb. If a hip flexion contracture prevents this extension, the patient cannot achieve a normal stride length.
To compensate for the lack of hip extension, the patient will anteriorly tilt the pelvis and hyperlordose the lumbar spine. This compensatory lumbar lordosis artificially advances the center of mass, allowing forward progression but placing immense shear stress on the posterior elements of the lower lumbar spine. Over time, this leads to facet arthropathy and chronic low back pain.
When evaluating a patient for lower extremity deformity, the Thomas Test must be performed to unmask hidden hip flexion contractures. Correcting a knee Fixed Flexion Deformity while ignoring a concomitant hip flexion contracture will result in persistent gait abnormalities and patient dissatisfaction.
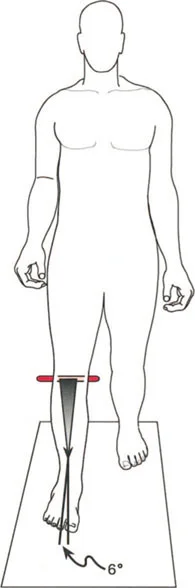
Torsional Deformities and Foot Progression Angle
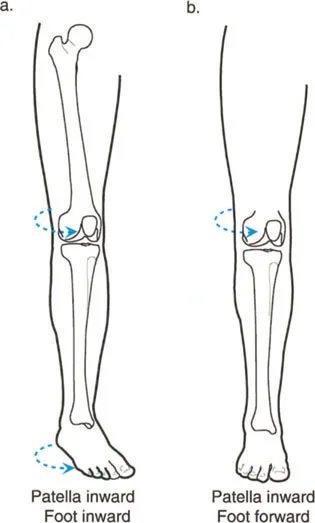
Rotational malalignment of the femur or tibia alters the lever arms of the lower extremity musculature and changes the Foot Progression Angle during gait.
Excessive femoral anteversion causes an internal rotation gait pattern. To maintain a forward facing Foot Progression Angle, the patient must externally rotate the tibia, leading to the classic miserable malalignment syndrome. This syndrome is characterized by increased femoral anteversion, compensatory external tibial torsion, and severe patellofemoral tracking issues.
From a dynamic perspective, severe rotational malalignment shifts the Ground Reaction Vector medially or laterally relative to the knee joint center during the stance phase. This creates abnormal varus or valgus thrusts, accelerating unicompartmental cartilage wear. Derotational osteotomies must be carefully planned using CT version studies to restore the normal mechanical lever arms of the gluteal and quadriceps muscles.
Clinical Pearls for Proximal and Rotational Deformities
- Always evaluate the spine and pelvis. A fixed pelvic obliquity will mimic a leg length discrepancy or a coronal plane deformity.
- Perform rotational profiles on all deformity patients. Correcting a varus knee without addressing severe internal tibial torsion will fail to restore normal gait kinematics.
- When planning a derotational osteotomy, consider the effect on the peroneal nerve, especially during large external rotation corrections of the proximal tibia.
Leg Length Discrepancy and Gait Kinematics
Leg Length Discrepancy is a frequent companion to angular deformity. While static radiographs quantify the absolute millimeter difference in bone length, the dynamic impact of a Leg Length Discrepancy on the gait cycle is far more complex.
Vaulting Steppage Gait and Equinus Compensations
A patient with a significant Leg Length Discrepancy greater than 2.5 centimeters will deploy various energy consuming strategies to clear the longer limb during the swing phase.
One common compensation is vaulting. The patient prematurely plantarflexes the ankle of the shorter stance limb, artificially lengthening it to allow the longer swing limb to clear the ground. Another compensation is circumduction, where the patient swings the longer limb out laterally in a wide arc. Both mechanisms drastically increase the metabolic cost of walking.
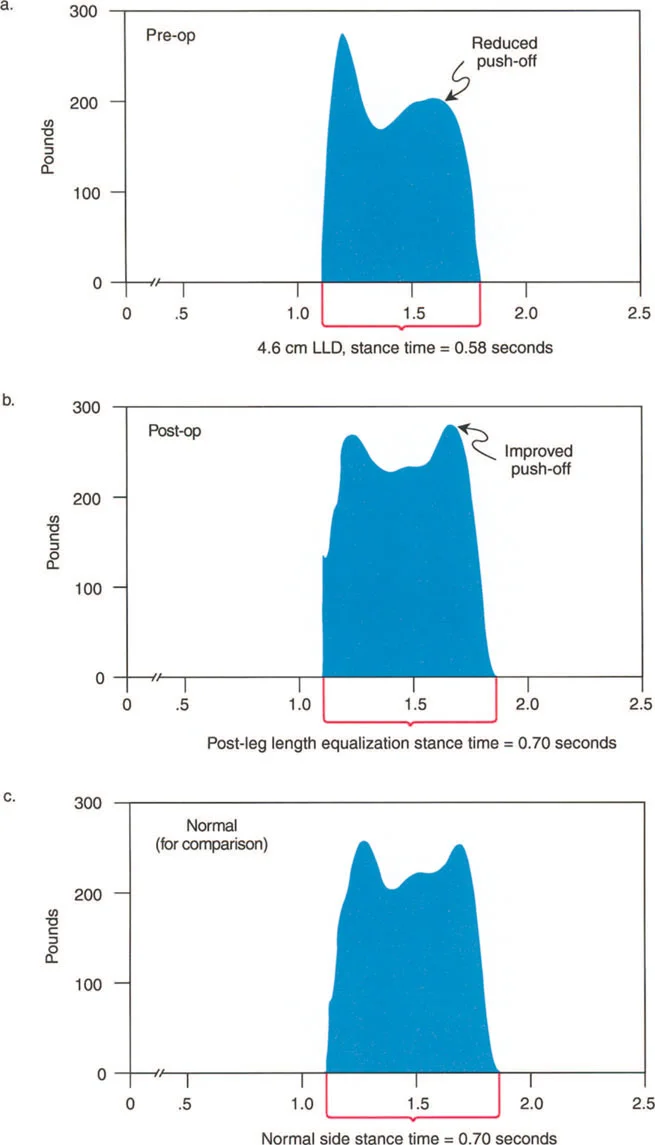
On the shorter limb side, patients frequently develop a compensatory equinus contracture. By walking on their toes, they functionally equalize the limb lengths. However, this locks the ankle out of the normal gait cycle, eliminating the shock absorbing capacity of the foot and ankle during initial contact and transferring abnormal forces directly to the knee and hip.
Dynamic Implications of Limb Lengthening
When planning a limb lengthening procedure using distraction osteogenesis, the surgeon must anticipate the dynamic resistance of the soft tissues. As the bone is lengthened, the surrounding muscles, fascia, and neurovascular structures resist the stretch.
If a femur is lengthened significantly without addressing the iliotibial band, the patient will develop a dynamic valgus deformity and a knee flexion contracture. Similarly, lengthening the tibia without protecting the ankle joint can result in a rigid equinus contracture as the gastrocsoleus complex tightens. Prophylactic soft tissue releases and meticulous physical therapy are mandatory to maintain joint motion and dynamic stability during the consolidation phase.
Conclusion and Future Directions in Deformity Correction
Mastering orthopedic gait biomechanics requires a paradigm shift from static radiographic measurement to dynamic functional analysis. The principles established by Dr. Dror Paley provide the mathematical and geometric foundation for deformity correction, but it is the surgeon's understanding of the Ground Reaction Vector, muscular compensations, and joint kinematics that ultimately dictates clinical success.
By integrating the Center of Rotation of Angulation, Mechanical Axis Deviation, and Joint Orientation Angles with a profound respect for dynamic lever arms, the modern orthopedic surgeon can execute complex osteotomies that not only straighten the bone but functionally restore the patient's ability to navigate the world with energy efficient, pain free locomotion. As technology advances with three dimensional surgical planning and robotic assisted osteotomies, the core biomechanical principles detailed in this masterclass will remain the indispensable bedrock of orthopedic limb reconstruction.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like