Predicting Pediatric Leg Length Discrepancy: Growth Plate Dynamics & Paley Principles
Key Takeaway
Predicting pediatric leg length discrepancy requires understanding growth plate dynamics and applying Paley Principles. This involves analyzing mechanical axis deviation, joint orientation angles, and the Center of Rotation of Angulation. Considering time and active physes is crucial for accurate prediction and precise surgical planning.
Introduction to Pediatric Leg Length Discrepancy and Deformity Correction
In the specialized realm of orthopedic deformity correction, leg length inequality is rarely an isolated clinical phenomenon. As meticulously dictated by Dr Dror Paley and his foundational principles of deformity correction, length inequality is a fundamental component of structural deviation that can be described simply in a single plane as either too long or too short. While length inequality may occasionally present as the sole structural anomaly representing a pure Leg Length Discrepancy, it is far more frequently associated with a complex, multi-planar triad of angular, rotational, and translational deformities.
When evaluating these complex deformities, orthopedic surgeons must meticulously analyze the global biomechanics of the lower extremity. A limb that is both short and bowed alters the entire kinematic chain of the patient. This structural imbalance leads to a cascade of compensatory mechanisms, including pelvic obliquity, compensatory lumbar scoliosis, vaulting gait patterns, and equinus contractures of the ankle joint. Failing to recognize these compensatory mechanisms can lead to catastrophic surgical planning errors, where a secondary compensation is mistakenly treated as a primary deformity.
However, when dealing with the pediatric population, orthopedic surgeons must account for a critical fourth dimension of deformity. That dimension is Time.
Unlike adult patients who present with static bone morphology, children possess active physes. These growth plates act as biological engines driving longitudinal and appositional expansion. When one of these biological engines is impaired, the limb discrepancy does not remain static. It evolves, adapts, and changes over time. In most clinically significant pathological abnormalities, the discrepancy becomes gradually greater as the child grows. Understanding how to predict this discrepancy at skeletal maturity is the absolute cornerstone of pediatric orthopedic planning. This prediction dictates whether a patient will require a simple conservative shoe lift, a precisely timed epiphysiodesis, or a complex multi-apical limb lengthening procedure utilizing distraction osteogenesis via an Ilizarov apparatus or a magnetic internal lengthening nail.
Core Paley Principles in Limb Reconstruction
To master the prediction and treatment of pediatric limb deformities, the surgeon must be fluent in the language of deformity analysis established by Dr Dror Paley. The Paley Principles provide a rigorous, mathematical, and reproducible framework for analyzing lower extremity alignment.
Mechanical Axis Deviation and Global Biomechanics
The mechanical axis of the lower extremity is the foundational reference line for all deformity planning. In a normal lower limb, the mechanical axis line is drawn from the center of the femoral head to the center of the ankle mortise. In a biomechanically neutral limb, this line should pass precisely through the center of the knee joint, specifically bisecting the tibial spines.
Mechanical Axis Deviation occurs when this line falls outside the center of the knee. If the mechanical axis passes medial to the center of the knee, the patient has a varus deformity, placing exponential stress on the medial compartment. If the axis passes lateral to the center of the knee, the patient exhibits a valgus deformity, overloading the lateral compartment. Quantifying the Mechanical Axis Deviation in millimeters is the first mandatory step in assessing the magnitude of the structural pathology. In a growing child, an uncorrected Mechanical Axis Deviation will lead to asymmetric physeal loading. According to the Hueter Volkmann principle, increased compression on a physis retards growth, meaning an existing varus deformity will progressively worsen over time as the medial physis slows down while the lateral physis continues to expand.
Joint Orientation Angles and Normal Values
Once Mechanical Axis Deviation is identified, the surgeon must locate the exact source of the deviation. This requires measuring the joint orientation angles. These angles define the relationship between the mechanical or anatomic axes of the long bones and their respective joint lines.
Understanding these normal parameters is non negotiable for the reconstructive surgeon. Deviations from these normative values indicate whether the deformity is located in the femur, the tibia, or within the joint space itself.
| Angle Acronym | Full Anatomic Definition | Normal Range |
|---|---|---|
| mLDFA | Mechanical Lateral Distal Femoral Angle | 85 to 90 degrees |
| MPTA | Medial Proximal Tibial Angle | 85 to 90 degrees |
| mLPFA | Mechanical Lateral Proximal Femoral Angle | 85 to 95 degrees |
| LDTA | Lateral Distal Tibial Angle | 86 to 92 degrees |
| JLCA | Joint Line Convergence Angle | 0 to 2 degrees |
The Joint Line Convergence Angle is particularly critical. A Joint Line Convergence Angle greater than 2 degrees indicates intra articular pathology, such as ligamentous laxity or cartilage loss, which must be accounted for separately from extra articular diaphyseal or metaphyseal deformities.
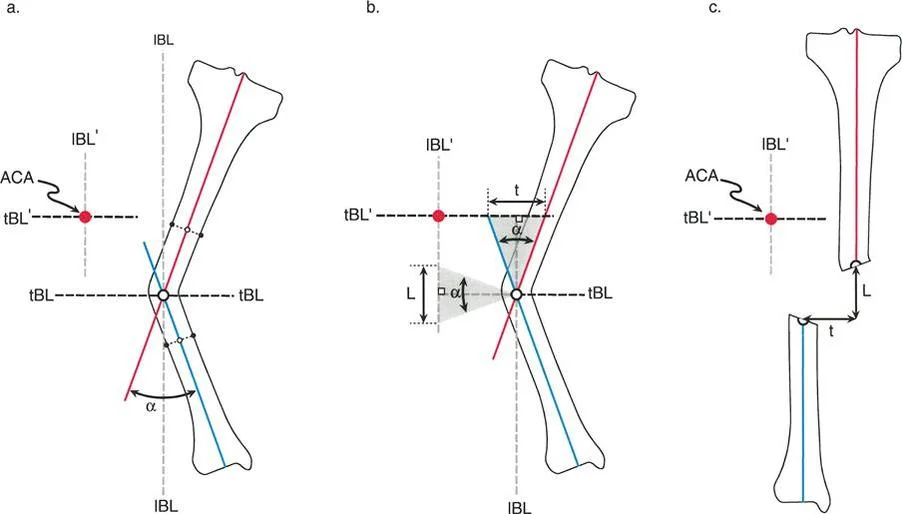
Center of Rotation of Angulation and The Osteotomy Rules
When an extra articular deformity is identified via abnormal joint orientation angles, the surgeon must locate the apex of the deformity, known as the Center of Rotation of Angulation. The Center of Rotation of Angulation is found by drawing the proximal mechanical axis line and the distal mechanical axis line of the deformed bone. The exact point where these two lines intersect is the Center of Rotation of Angulation.
Dr Paley established three fundamental Osteotomy Rules based on the relationship between the osteotomy site, the hinge point, and the Center of Rotation of Angulation. Mastering these rules is essential for avoiding iatrogenic translation during deformity correction.
- Osteotomy Rule 1: When the osteotomy and the correction hinge are both placed exactly at the Center of Rotation of Angulation, the bone will undergo pure angular correction without any translation. The mechanical axis will be perfectly realigned.
- Osteotomy Rule 2: When the osteotomy is made at a different level than the Center of Rotation of Angulation, but the correction hinge remains at the Center of Rotation of Angulation, the bone will undergo angular correction combined with a planned translation. This is highly useful when the Center of Rotation of Angulation is located in poor quality bone or near a joint capsule, necessitating a diaphyseal cut.
- Osteotomy Rule 3: When the osteotomy and the correction hinge are both placed away from the Center of Rotation of Angulation, an iatrogenic translation deformity will be created. This rule is generally a warning of what to avoid, unless the surgeon is intentionally trying to correct a preexisting translational deformity.
Key Surgical Pearls for Deformity Analysis
* Always obtain full length, weight bearing, standing anteroposterior radiographs with the patellae oriented forward to accurately assess the mechanical axis.
* Rotational deformities cannot be accurately assessed on standard two dimensional radiographs and require clinical examination (thigh foot angle, prone internal external rotation) or a rotational computed tomography scan.
* When planning an osteotomy in a child, the surgeon must ensure the planned cut and fixation hardware do not violate the open physis.
Time as the Fourth Dimension in Pediatric Orthopedics
Adult deformity correction is a mathematical exercise in three dimensional space. Pediatric deformity correction requires integrating the dimension of time. To master the prediction of limb length inequality, the reconstructive surgeon must first understand the biological behavior of the physis at a cellular level.
Biomechanics and Histology of the Physis
The growth plate is a highly organized, avascular cartilaginous structure divided into distinct histological zones. Each zone plays a specific role in endochondral ossification, and insults to different zones produce vastly different clinical outcomes.
The Resting Zone, also known as the reserve zone, is located immediately adjacent to the epiphysis. It contains scattered chondrocytes and serves as the stem cell reservoir for the growth plate. It also produces the matrix necessary for the active zones. Ischemia or severe trauma to this zone results in permanent, irreversible growth arrest.
The Proliferative Zone is where chondrocytes undergo rapid mitosis, stacking into longitudinal columns. This zone is the primary biological engine of longitudinal growth. Conditions like achondroplasia specifically target this zone, resulting in profound short stature and disproportionate limb lengths.
The Hypertrophic Zone is subdivided into maturation, degeneration, and provisional calcification layers. Here, chondrocytes swell to several times their original size, preparing the matrix for vascular invasion and osteoblast activity from the metaphysis. Because this zone lacks significant collagen matrix, it is the weakest link in the pediatric bone. It is the anatomical site of failure in Slipped Capital Femoral Epiphysis and the majority of Salter Harris fractures.
Pathophysiology of Physeal Insults
Insults to these zones whether traumatic, infectious, iatrogenic, or congenital alter the longitudinal growth vector. When a deformity involves an angulation, the asymmetrical insult to the physis will not only cause a progressive length discrepancy but also a progressive angular deformity.
For example, a localized meningococcal infection that destroys the medial aspect of the proximal tibial physis creates a medial physeal bar. The lateral physis continues to grow, acting as a tether against the arrested medial side. This creates a rapidly progressive varus deformity (altering the Medial Proximal Tibial Angle) combined with a progressive overall shortening of the tibia. Because of the time dimension, the magnitude of both the discrepancy and the Mechanical Axis Deviation will increase exponentially during the adolescent growth spurt. Therefore, predicting the ultimate discrepancy at skeletal maturity is not just about equalizing limb lengths; it is about timing the surgical intervention to restore the mechanical axis precisely when the child stops growing.
Shapiros Five Patterns of Leg Length Discrepancy Progression
In 1982, Shapiro revolutionized the pediatric orthopedic understanding of limb length inequality by describing five distinct patterns of progression in children. Recognizing these specific patterns is paramount for surgical planning. Our mathematical and graphical methods for predicting discrepancies at skeletal maturity are only reliable when applied to specific progression types. Applying a multiplier method to the wrong Shapiro pattern will result in catastrophic over or under correction.
Type 1 Upward Slope Proportionate Progression
This is the most common pattern observed in congenital and developmental causes of limb length inequality. In this pattern, the discrepancy increases at a constant, linear rate that is strictly proportionate to the childs overall growth. The percentage of growth inhibition remains constant over time. Because the ratio of inhibition is mathematically stable, this is the only type of discrepancy that can be accurately predicted using standard multiplier or graphing methods.
Clinical examples include congenital short femur, fibular hemimelia, hemiatrophy, hemihypertrophy, and complete epiphyseal arrest following a severe Salter Harris fracture. Patients with Type 1 progression typically present with large, clinically significant discrepancies that demand surgical intervention. The slope of the line on a growth graph remains constant until skeletal maturity is reached.
Type 2 Upward Slope Deceleration Pattern
In the Type 2 pattern, the length discrepancy initially increases rapidly, but then the rate of discrepancy begins to slow down and decelerate over time. Because of this unpredictable deceleration phase, standard predictive methods will vastly overestimate the final discrepancy at skeletal maturity.
Clinical examples include certain neuromuscular diseases, mild congenital hypoplasia, or localized radiation therapy. While the growth velocity of the affected limb eventually catches up slightly to the normal limb, the affected limb never regains the lost length. It simply stops falling further behind at such a rapid rate.
Type 3 Upward Slope Plateau Pattern
The Type 3 pattern is characterized by a discrepancy that increases for a defined period and then plateaus. Once the plateau is reached, the affected limb and the normal limb begin growing at the exact same velocity. The absolute magnitude of the discrepancy remains static from the plateau point onward.
The classic clinical example is a fractured femur in a young child. Initially, overriding of the fracture fragments or immediate post traumatic shortening occurs (the upward slope). Subsequently, the hyperemia associated with fracture healing may cause a temporary overgrowth, but eventually, the limbs return to a normal, symmetrical growth rate (the plateau). This pattern typically results in small, static discrepancies that rarely require massive reconstructive lengthening.
Type 4 Upward Slope Plateau Upward Slope Pattern
This is a highly complex, undulating pattern of growth discrepancy. The length inequality increases, plateaus for a period of time, and then unpredictably begins to increase again.
The pathognomonic clinical example is Legg Calve Perthes disease. Initially, the avascular necrosis causes the femoral head to collapse, resulting in an upward slope of discrepancy. As the disease enters the fragmentation and reossification phases, growth stabilizes, creating the plateau. However, eventually, the damaged capital femoral physis undergoes premature senescence and arrest, while the contralateral normal leg continues its adolescent growth spurt, resulting in the second upward slope. This pattern is entirely unpredictable without serial radiographic monitoring over many years.
Type 5 Upward Slope Plateau Downward Slope Pattern
This pattern involves an initial increase in the discrepancy, a stabilization period, and then an actual decrease in the discrepancy. In this scenario, the short leg starts catching up, or the long leg begins to slow down.
The most common clinical examples are Juvenile Idiopathic Arthritis or severe hemophilic arthropathy. Initially, the massive inflammatory hyperemia to the joint causes the affected limb to overgrow, creating a discrepancy where the diseased leg is actually longer than the normal leg. Later in the disease process, the chronic, relentless inflammation causes premature physeal closure of that same overgrown limb. As the normal limb continues to grow, it catches up to and eventually surpasses the diseased limb, creating a downward slope on the discrepancy graph.
Key Takeaways for Shapiro Patterns
* Never apply the Paley Multiplier Method to a Type 4 or Type 5 pattern, as the growth velocity is non linear and highly unpredictable.
* Serial scanograms taken at least six months apart are mandatory to establish which Shapiro pattern a patient is following.
* Congenital anomalies almost universally follow a Type 1 pattern, making early and aggressive surgical planning highly reliable.
Advanced Predictive Methods for Leg Length Inequality
Once a Type 1 proportionate progression is confirmed, the surgeon must calculate the exact predicted discrepancy at skeletal maturity. This number dictates the entire surgical strategy. Over the decades, several methods have been developed, including the Menelaus rule of thumb, the Green Anderson remaining growth graphs, and the Mose circle method. However, the modern gold standard in deformity correction is the Paley Multiplier Method.
The Paley Multiplier Method
Developed by Dr Dror Paley, the Multiplier Method simplifies the complex logarithmic data of the Green Anderson growth charts into a highly accurate, easily applicable mathematical formula. The method is based on the principle that the proportion of bone length achieved at any given age is constant across populations, regardless of the final absolute height of the individual.
The formula is elegantly simple:
Current Leg Length Discrepancy multiplied by the Age and Sex Specific Multiplier equals the Predicted Leg Length Discrepancy at Skeletal Maturity.
For example, if a 4 year old boy has a congenital short femur with a current discrepancy of 3 centimeters, the surgeon consults the Paley Multiplier table for boys at age 4. If the multiplier is 2.0, the predicted discrepancy at skeletal maturity will be exactly 6 centimeters.
This method is revolutionary because it eliminates the need for complex bone age calculations in most patients and can be performed instantly in the clinic. Paley later expanded this method to include multipliers for predicting the timing of epiphysiodesis, predicting the final height of the patient, and predicting the length of individual bone segments.
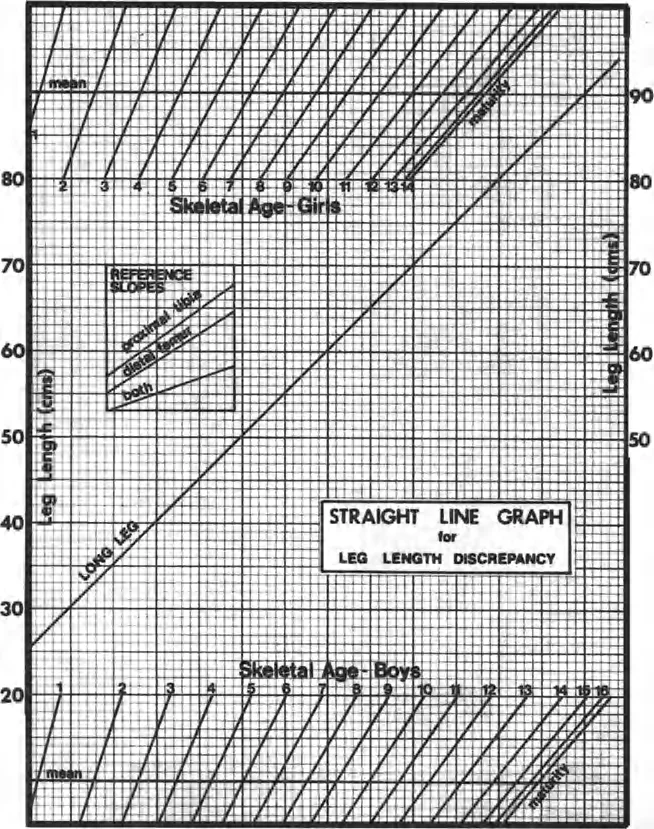
Green Anderson Growth Remaining Method
While the Paley Multiplier is the most efficient modern tool, reconstructive surgeons must still understand the foundational Green Anderson method. This method utilizes standard deviations and percentile charts based on decades of longitudinal radiographic data. It requires the surgeon to determine the childs exact skeletal age using a Greulich and Pyle atlas of the left hand and wrist.
The surgeon plots the length of the normal limb and the short limb on the Green Anderson graph. By extrapolating the lines to the skeletal maturity endpoint (age 16 for females, age 18 for males), the final discrepancy can be visualized. While highly accurate for Type 1 patterns, it is cumbersome, prone to plotting errors, and highly dependent on the subjective interpretation of skeletal bone age from hand radiographs.
Surgical Management Strategies and Timing
The ultimate goal of predicting the discrepancy is to intervene at the optimal biological moment. The surgical management of leg length inequality is broadly divided into two categories: shortening the long leg (epiphysiodesis) or lengthening the short leg (distraction osteogenesis).
Epiphysiodesis and Growth Modulation
For predicted discrepancies between 2.0 and 5.0 centimeters at skeletal maturity, epiphysiodesis of the longer, normal limb is the treatment of choice. This procedure involves surgically arresting the physis of the distal femur, proximal tibia, or both, allowing the shorter limb to catch up over time.
Timing is the most critical variable in epiphysiodesis. If performed too early, the short leg will surpass the normal leg, creating an iatrogenic reverse discrepancy. If performed too late, the short leg will never catch up. The Paley Epiphysiodesis Multiplier is used to calculate the exact chronological age at which the procedure should be performed to achieve perfect symmetry at maturity.
Modern techniques have shifted away from the traditional open Phemister bone block technique toward percutaneous drilling and curettage under fluoroscopic guidance. Alternatively, reversible growth modulation using tension band plates (eight plates) can be utilized. These plates tether the physis without destroying the reserve zone cells. If the limbs equalize before skeletal maturity, the plates can be removed, and physeal growth will resume.
Multi Apical Deformity Correction and Lengthening
For predicted discrepancies greater than 5.0 centimeters, or for discrepancies associated with severe angular and translational deformities, epiphysiodesis is contraindicated because it would result in unacceptable disproportionate short stature. These patients require surgical limb lengthening.
Limb lengthening relies on the biological miracle of distraction osteogenesis, pioneered by Gavriil Ilizarov and refined by Dr Paley. The bone is surgically fractured using a low energy percutaneous corticotomy, meticulously preserving the periosteum and endosteal blood supply.
Following a latency period of 5 to 7 days to allow soft callus formation, the bone ends are gradually pulled apart at a rate of exactly 1 millimeter per day (divided into four 0.25 millimeter increments). This tension stress stimulates the proliferative zone of the callus to generate new, woven bone.
Historically, this was achieved using bulky external circular fixators (the Ilizarov apparatus or Taylor Spatial Frame). These devices allow for simultaneous correction of angulation, translation, and rotation by manipulating the struts according to the Center of Rotation of Angulation rules.
Today, the paradigm has shifted toward fully implantable magnetic lengthening nails (such as the PRECICE or STRYDE systems). These intramedullary devices contain rare earth magnets that interact with an external remote control. They eliminate the high rate of pin tract infections associated with external fixators and drastically improve the psychosocial experience of the pediatric patient. However, because intramedullary nails follow a fixed linear path, the surgeon must acutely correct all angular and translational deformities at the time of the initial osteotomy, relying heavily on precise execution of Paleys Osteotomy Rules.
Step by Step Preoperative Planning Protocol
Successful deformity correction is won or lost in the preoperative planning phase. Surgeons in training must adhere to a strict, reproducible protocol when evaluating a pediatric patient with a limb length inequality.
- Obtain Proper Imaging: Acquire full length, standing, weight bearing anteroposterior radiographs of both lower extremities. Ensure the patellae are facing strictly forward to eliminate rotational artifact. Obtain orthogonal lateral views.
- Establish the Mechanical Axis: Draw the mechanical axis line from the center of the femoral head to the center of the ankle mortise on the affected limb.
- Quantify the Deviation: Measure the Mechanical Axis Deviation in millimeters medial or lateral to the center of the knee joint.
- Measure Joint Orientation Angles: Calculate the mLDFA, MPTA, mLPFA, and LDTA. Compare these values to the normative tables to identify whether the deformity is femoral, tibial, or combined.
- Locate the Apex: Draw the proximal and distal mechanical axis lines of the deformed bone segment to identify the Center of Rotation of Angulation.
- Assess the Discrepancy Pattern: Review historical scanograms to confirm the patient is exhibiting a Shapiro Type 1 proportionate progression.
- Calculate Final Discrepancy: Apply the Paley Multiplier Method based on the childs current age and sex to predict the exact leg length discrepancy at skeletal maturity.
- Formulate the Strategy: Based on the predicted discrepancy, decide between epiphysiodesis (for discrepancies under 5cm) or lengthening (for discrepancies over 5cm).
- Apply Osteotomy Rules: If lengthening or acute angular correction is required, plan the osteotomy level and hinge placement strictly according to Paleys three rules to avoid iatrogenic translation.
- Execute and Monitor: Perform the surgical intervention with meticulous soft tissue handling. If distraction osteogenesis is utilized, monitor the regenerate bone weekly with radiographs to adjust the rate of distraction, preventing premature consolidation or nonunion.
By mastering the intricate relationship between the Paley Principles of deformity analysis and the biological dimension of time, the reconstructive orthopedic surgeon can confidently navigate the immense complexities of pediatric limb lengthening, ultimately restoring biomechanical harmony and function to the growing child.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like