Hip Osteotomy: Precision Correction for Proximal Femoral Deformities & Joint Preservation
Key Takeaway
Proximal femoral osteotomy is a surgical procedure to correct deformities of the upper thigh bone, such as coxa vara or valga. It restores hip biomechanics, optimizes abductor function, and redistributes joint loads. This intervention aims to prevent early osteoarthritis and preserve the native hip joint in young, active patients.
Comprehensive Introduction to Proximal Femoral Deformities
The evaluation and surgical management of proximal femoral deformities represent one of the most mechanically demanding and intellectually rigorous domains within orthopedic surgery. The hip joint, acting as the primary articulation transferring axial loads from the appendicular to the axial skeleton, is exquisitely sensitive to alterations in its spatial orientation. Deformities of the proximal femur fundamentally disrupt the delicate equilibrium of joint reaction forces, necessitating a profound understanding of biomechanics, joint orientation angles, and precise surgical realignment techniques.
These deformities frequently arise as sequelae of pediatric hip conditions, including developmental dysplasia of the hip (DDH), Legg-Calvé-Perthes disease, slipped capital femoral epiphysis (SCFE), and traumatic physeal arrests. When the capital femoral epiphysis suffers an ischemic insult or premature closure, the greater trochanteric apophysis often continues its upward trajectory. This results in the classic presentation of coxa vara combined with trochanteric overgrowth, clinically termed coxa breva. This anatomical distortion drastically alters the resting length and moment arm of the hip abductor musculature, precipitating a cascade of biomechanical failures that culminate in early-onset secondary osteoarthritis.
Historically, the orthopedic community relied heavily on salvage procedures or early arthroplasty for these complex deformities. However, the pioneering work of surgeons such as Pauwels, Bombelli, Wagner, Morscher, and ultimately Dr. Dror Paley, catalyzed a paradigm shift toward precise, biomechanically sound osteotomies aimed at restoring native joint kinematics. These interventions are not merely realignments of bone; they are sophisticated re-engineering efforts designed to optimize the weight-bearing surface area, normalize the articulotrochanteric distance (ATD), and restore the resting tension of the pelvifemoral musculature.
Pathoepidemiology and Natural History
The pathoepidemiology of proximal femoral deformities underscores a critical window for joint-preserving interventions. In pathologic states such as severe coxa vara, the Neck-Shaft Angle (NSA) may plummet below 110 degrees, and the Mechanical Proximal Femoral Angle (MPFA) may concurrently drop. This significantly shifts the mechanical axis medially, increasing shear forces across the articular cartilage.
The resultant lateralization of the femoral shaft and relative proximal migration of the greater trochanter critically shorten the abductor lever arm. Epidemiological data consistently demonstrate that patients harboring such uncorrected deformities exhibit a nearly universal progression to symptomatic osteoarthritis by their third or fourth decade of life. The altered kinematics not only induce a debilitating Trendelenburg gait but also concentrate peak contact stresses on the superolateral acetabular rim, accelerating chondral delamination and subchondral cystic degeneration.
The overarching goal of proximal femoral osteotomy in the young, active patient is to delay or entirely abrogate the need for total hip arthroplasty. By redistributing mechanical loads across preserved, healthy articular cartilage, the orthopedic surgeon can grant the native joint decades of functional longevity.
Biomechanics and Joint Orientation Angles of the Hip
A rigorous mastery of proximal femoral anatomy and its associated biomechanical parameters is the absolute prerequisite for executing complex hip osteotomies. The modern orthopedic surgeon must utilize the systematic approach popularized by Dr. Dror Paley, which relies on standardized joint orientation angles and the calculation of Mechanical Axis Deviation (MAD).
The Normal Proximal Femur
The proximal femur is defined by several critical angular measurements that dictate its spatial relationship to the pelvis and the lower extremity mechanical axis.
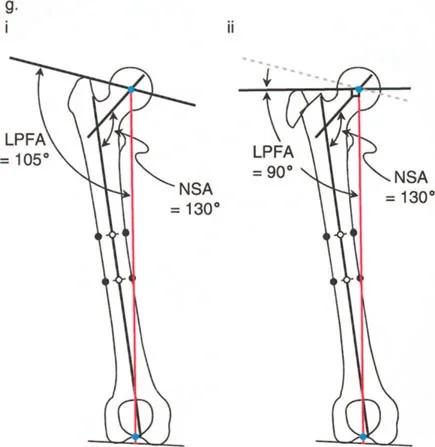
- Neck-Shaft Angle NSA: Formed by the intersection of the anatomical axis of the femoral shaft and the axis of the femoral neck. It dictates the lateral offset of the femur and the verticality of the femoral head within the acetabulum.
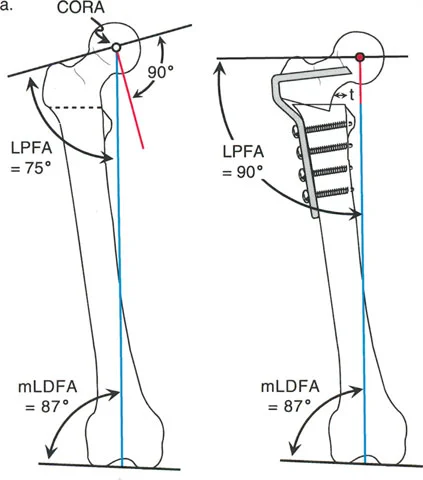
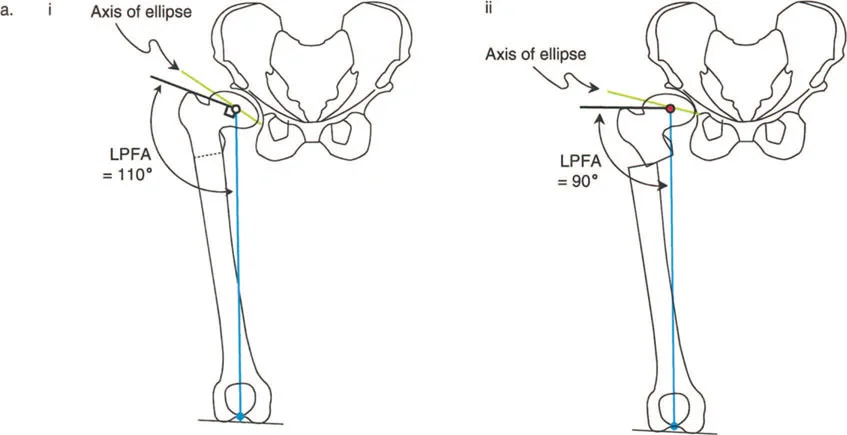
- Mechanical Proximal Femoral Angle MPFA: Defined by the mechanical axis of the femur and the line connecting the tip of the greater trochanter to the center of the femoral head. It is a paramount indicator of abductor mechanics.
- Mechanical Lateral Proximal Femoral Angle mLPFA: The lateral angle formed between the mechanical axis of the femur and the proximal joint orientation line of the femur.
In a structurally normal hip, the NSA typically measures between 130 and 135 degrees, while the normal mLPFA and MPFA hover around 90 degrees (range 85 to 95 degrees). When evaluating the entire lower extremity, these proximal angles must be considered in conjunction with the mechanical Lateral Distal Femoral Angle (mLDFA) and the mechanical Proximal Tibial Angle (MPTA) to ensure the overall mechanical axis passes precisely through the center of the knee joint.
| Joint Orientation Angle | Normal Range | Clinical Significance |
|---|---|---|
| NSA | 130 - 135 degrees | Determines femoral offset and leg length |
| mLPFA | 85 - 95 degrees (Avg 90) | Assesses proximal femoral mechanical alignment |
| MPFA | 85 - 95 degrees (Avg 90) | Indicator of abductor lever arm efficiency |
| mLDFA | 85 - 90 degrees (Avg 87.5) | Distal femoral mechanical alignment |
| MPTA | 85 - 90 degrees (Avg 87.5) | Proximal tibial mechanical alignment |
Abductor Mechanics and the Articulotrochanteric Distance
The abductor mechanism, primarily comprising the gluteus medius and minimus, operates as a first-class lever system where the femoral head serves as the fulcrum. The efficiency of this system is heavily dependent on the length of the abductor lever arm, which is the perpendicular distance from the center of rotation of the femoral head to the line of action of the abductor muscles.
A critical metric in evaluating this lever system is the Articulotrochanteric Distance (ATD). The ATD is the vertical distance between the superior articular surface of the femoral head and the tip of the greater trochanter. A normal ATD is positive, typically measuring 15 to 30 millimeters.
When a varus deformity occurs, or when a varus osteotomy is performed without addressing the greater trochanter, the trochanter is inevitably displaced proximally. This proximal migration drastically shortens the abductor lever arm and results in a negative ATD. The abductor muscles become adaptively shortened and mechanically disadvantaged, leading to a positive Trendelenburg sign and increased joint reaction forces as the muscles must fire with significantly greater force to maintain pelvic level during the single-leg stance phase of gait.
Surgical Pearls for Abductor Mechanics
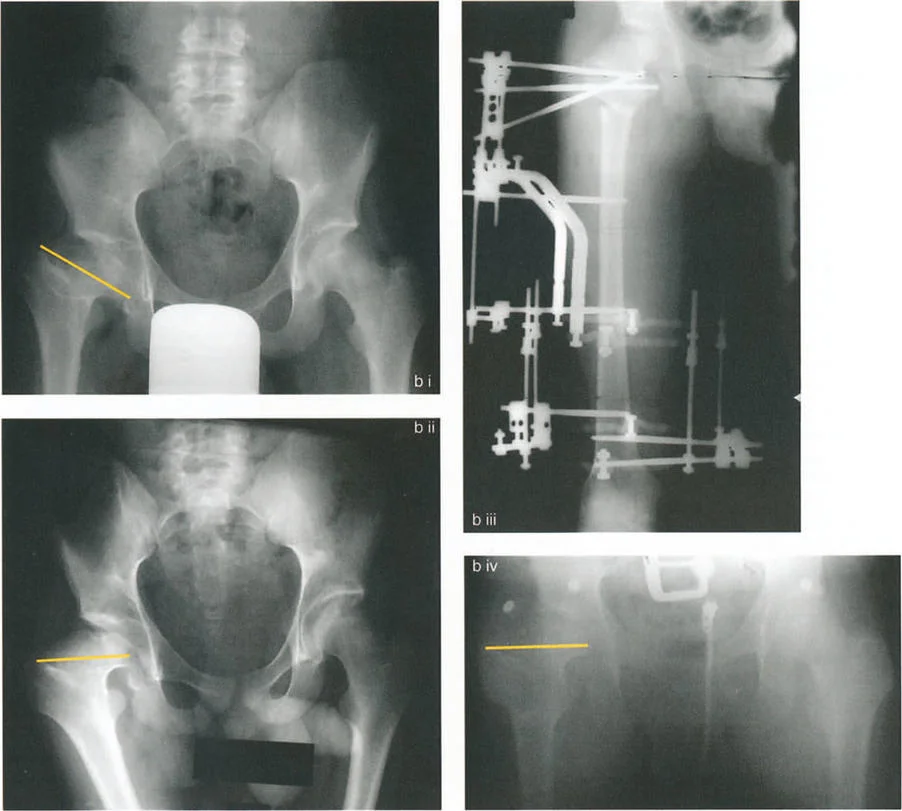
* Always evaluate the ATD on an AP pelvis radiograph prior to planning a proximal femoral osteotomy.
* If the ATD is negative, isolated angular correction of the femoral neck will be insufficient; a concurrent distal and lateral transfer of the greater trochanter is mandatory.
* Restoring a positive ATD decreases the required abductor force, thereby exponentially decreasing the joint reaction forces across the articular cartilage.
Pathoanatomy of Specific Proximal Femoral Deformities
Understanding the specific morphological changes associated with various disease states is critical for applying Paley principles effectively. The decision to intervene surgically requires a nuanced appreciation of the natural history of the specific underlying pathology.
Coxa Vara and Trochanteric Overgrowth
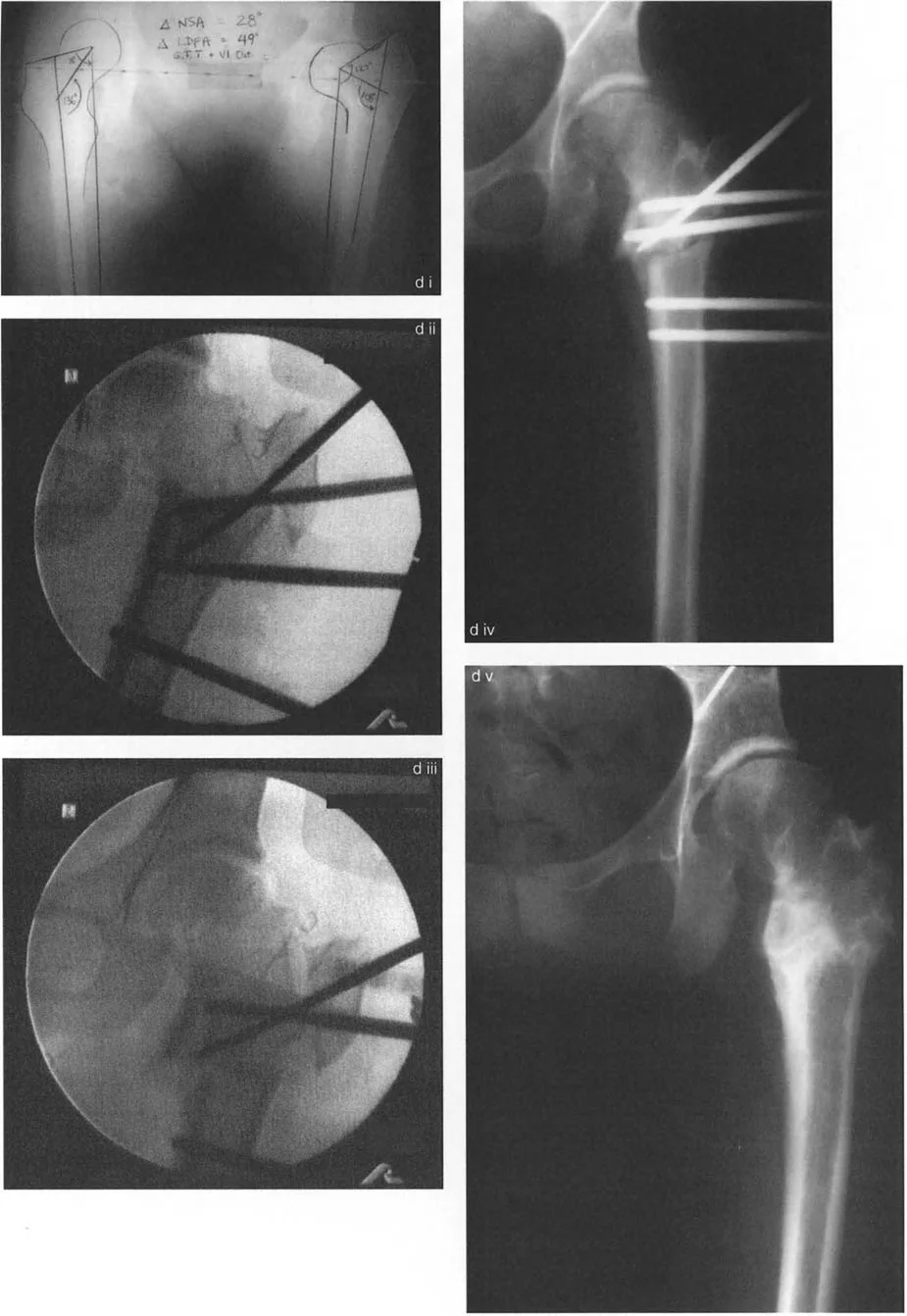
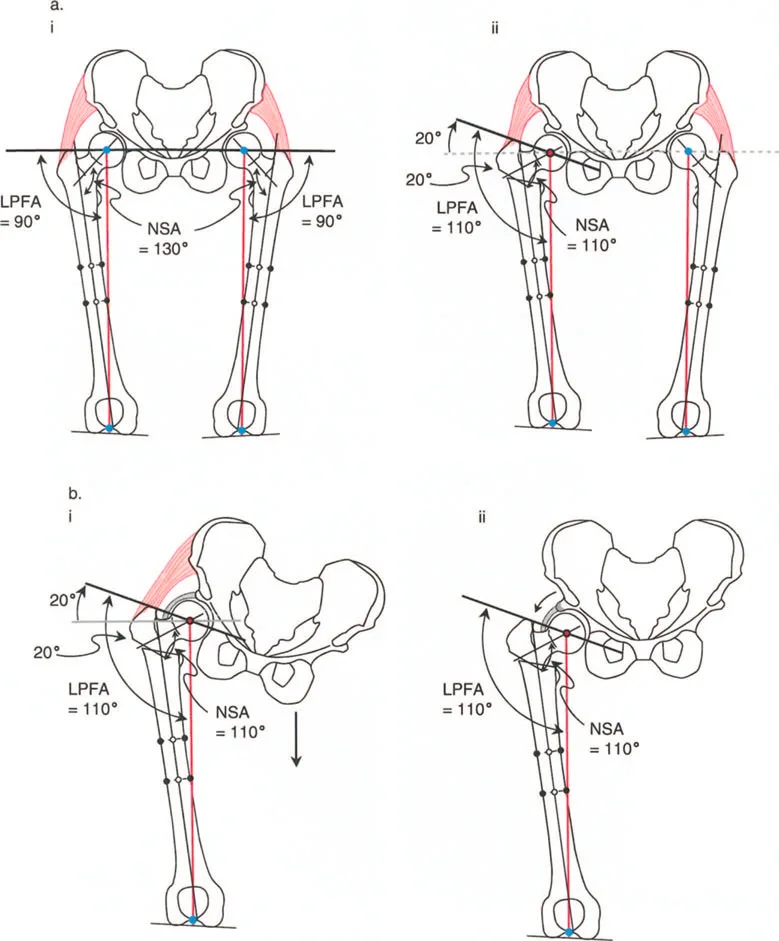
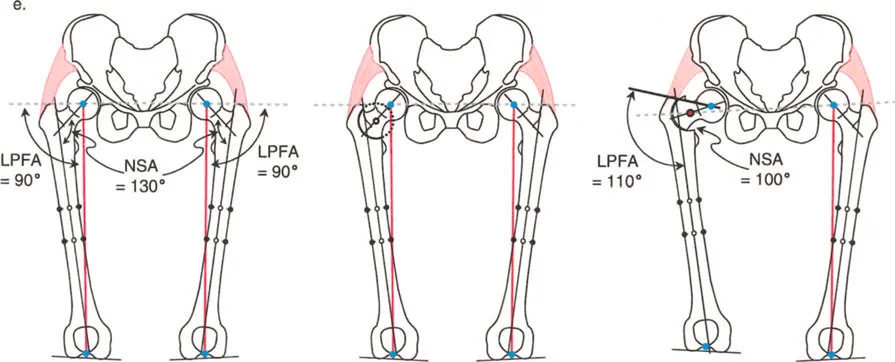
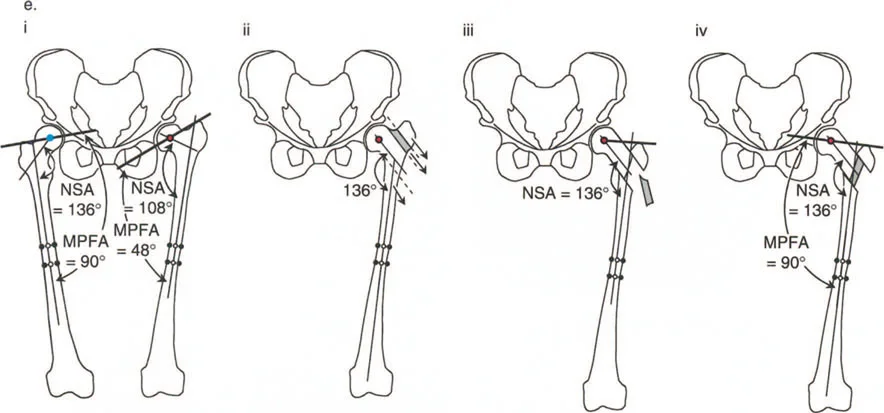
In a classical varus deformity with trochanteric overgrowth (often seen post-Perthes or following avascular necrosis in DDH treatment), a surgeon may encounter an MPFA of 48 degrees and an NSA of 108 degrees. This starkly contrasts with a normal contralateral MPFA of 90 degrees and NSA of 136 degrees.
This discrepancy highlights a crucial Paley concept: the varus deformity is a composite of both femoral neck angulation and trochanteric overgrowth. It demands a multifaceted surgical correction rather than a simple uniplanar wedge excision. The mechanical axis is shifted medially, creating a medial Mechanical Axis Deviation (MAD). The weight-bearing forces are concentrated on the medial compartment of the knee and the superomedial aspect of the femoral head.
Coxa Valga and Hip Dysplasia
Conversely, coxa valga is characterized by an abnormally high NSA (often greater than 140 degrees) and an increased MPFA. This is frequently observed in neuromuscular conditions such as cerebral palsy or as a compensatory mechanism in hip dysplasia.
In coxa valga, the femoral head is subluxated laterally, reducing the weight-bearing surface area (WBF:SA ratio). The abductor moment arm is shortened not by proximal migration, but by a decrease in femoral offset. The mechanical axis is shifted laterally, creating a lateral MAD. Surgical correction typically involves a varus-producing osteotomy to lateralize the mechanical axis, improve femoral head coverage, and restore femoral offset.
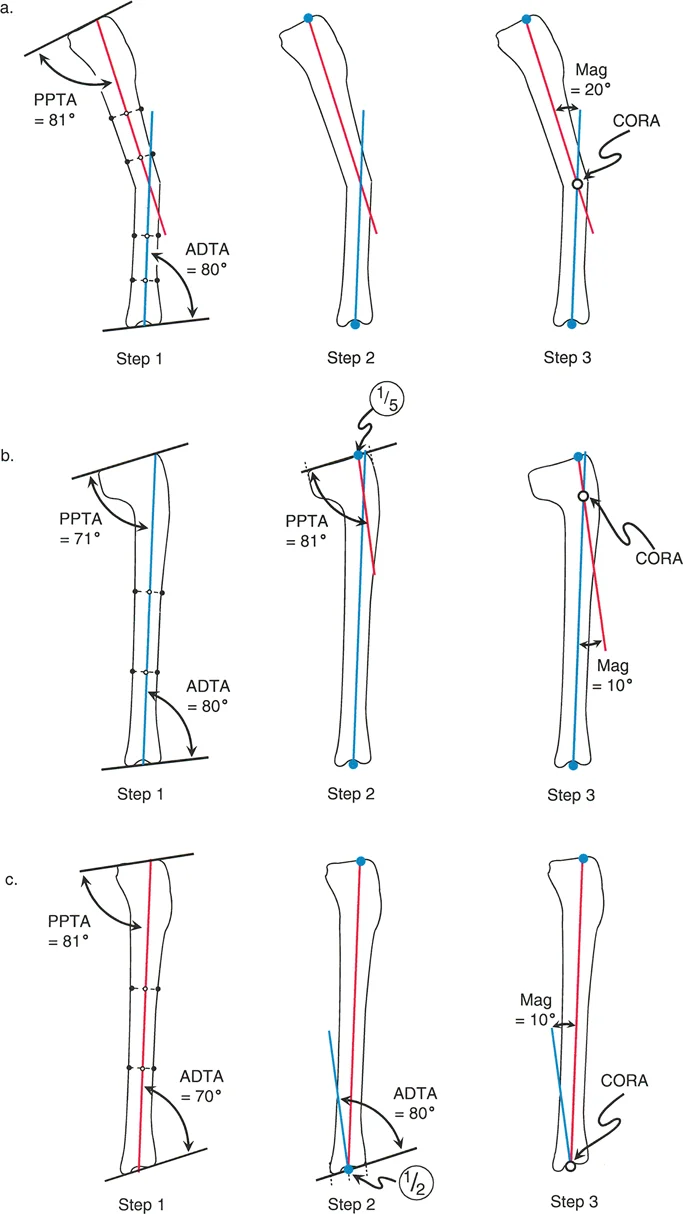
Preoperative Planning Using the CORA Method
The cornerstone of modern deformity correction is the Center of Rotation of Angulation (CORA) method. Applying this method to the proximal femur ensures that angular corrections do not inadvertently induce secondary translational deformities that compromise the mechanical axis.
Identifying the Center of Rotation of Angulation
The CORA is the intersection point of the proximal and distal mechanical (or anatomical) axes of the deformed bone.
Step by Step Guide to Identifying the Proximal Femoral CORA
1. Obtain standard radiographs: A long-leg standing AP radiograph and a dedicated AP pelvis are required.
2. Draw the proximal axis: Establish the proximal joint orientation line (connecting the tip of the greater trochanter to the center of the femoral head). Draw a line at the normal mLPFA (90 degrees) to this joint line. This is the proximal mechanical axis.
3. Draw the distal axis: Draw the mechanical axis of the distal femoral segment (a line from the center of the knee joint extending proximally, accounting for the normal mLDFA).
4. Locate the intersection: The point where the proximal and distal axes intersect is the CORA. In proximal femoral deformities, the CORA is frequently located within the femoral neck or the intertrochanteric region.

Applying Paley Osteotomy Rules to the Hip
Dr. Paley established three fundamental osteotomy rules that dictate the relationship between the CORA, the osteotomy site, and the resulting alignment. Understanding these rules is critical when operating on the proximal femur, as the anatomical constraints of the hip joint often prevent placing the osteotomy directly at the CORA.
| Paley Osteotomy Rule | Description | Application in the Proximal Femur |
|---|---|---|
| Rule 1 | Osteotomy and hinge are at the CORA. | Results in pure angular correction without translation. Ideal but often anatomically impossible in the high femoral neck. |
| Rule 2 | Osteotomy is at a different level than the CORA, but the hinge remains on the bisector line of the CORA. | Results in angular correction with intentional translation. This is the most common scenario for intertrochanteric osteotomies. |
| Rule 3 | Osteotomy and hinge are both away from the CORA. | Results in a secondary translational deformity (zigzag deformity). Must be avoided to prevent mechanical axis deviation. |
When correcting a severe coxa vara deformity, the CORA is often located in the mid-femoral neck. However, performing an osteotomy at this level carries an unacceptably high risk of avascular necrosis due to the disruption of the medial femoral circumflex artery. Therefore, the osteotomy is performed distally in the intertrochanteric or subtrochanteric region.
According to Paley Osteotomy Rule 2, because the osteotomy is distal to the CORA, the surgeon must purposefully translate the distal femoral shaft medially during a valgus correction to ensure the mechanical axis is restored. Failure to translate will result in a lateral mechanical axis deviation and secondary valgus alignment of the knee.
Digital Templating and Axis Determination
Advanced digital templating software is now standard of care for preoperative planning. The surgeon must template the exact angle of the wedge to be resected (or opened) and the precise amount of translation required.
Furthermore, the chronicity of the deformity dictates the degree of adaptive shortening in the abductors, the psoas, and the joint capsule. An overgrown greater trochanter resulting from a treated DDH presents a vastly different soft-tissue envelope compared to a post-traumatic malunion. Digital templating allows the surgeon to anticipate the need for soft-tissue releases, such as a fractional lengthening of the iliopsoas or an adductor tenotomy, to achieve the planned bony correction.
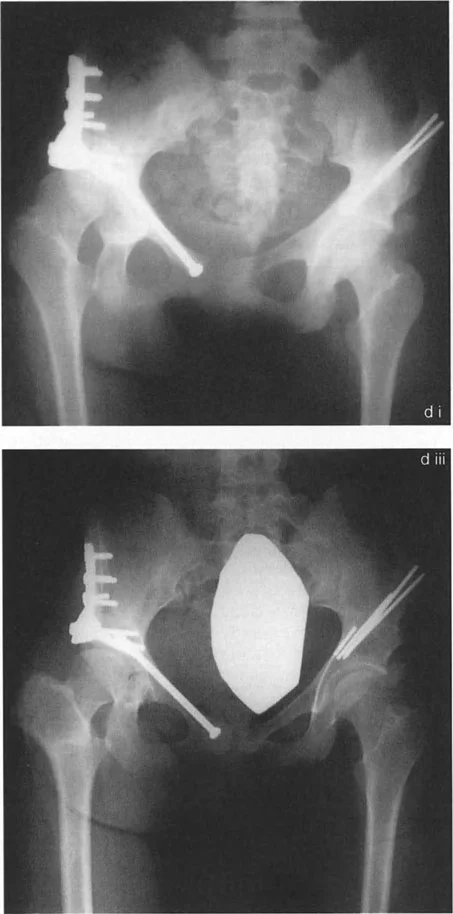
Surgical Execution of Proximal Femoral Osteotomies
The execution of a proximal femoral osteotomy requires meticulous surgical technique, rigid internal fixation, and a deep respect for the vascular supply to the femoral head.
Valgus Producing Intertrochanteric Osteotomy
The valgus-producing osteotomy is the workhorse procedure for correcting coxa vara, improving femoral head sphericity in Perthes disease (hinge abduction), and treating femoral neck non-unions. By converting shear forces into compressive forces across the fracture or physis, valgus osteotomies promote bone healing and stabilize the joint.
Key Surgical Steps
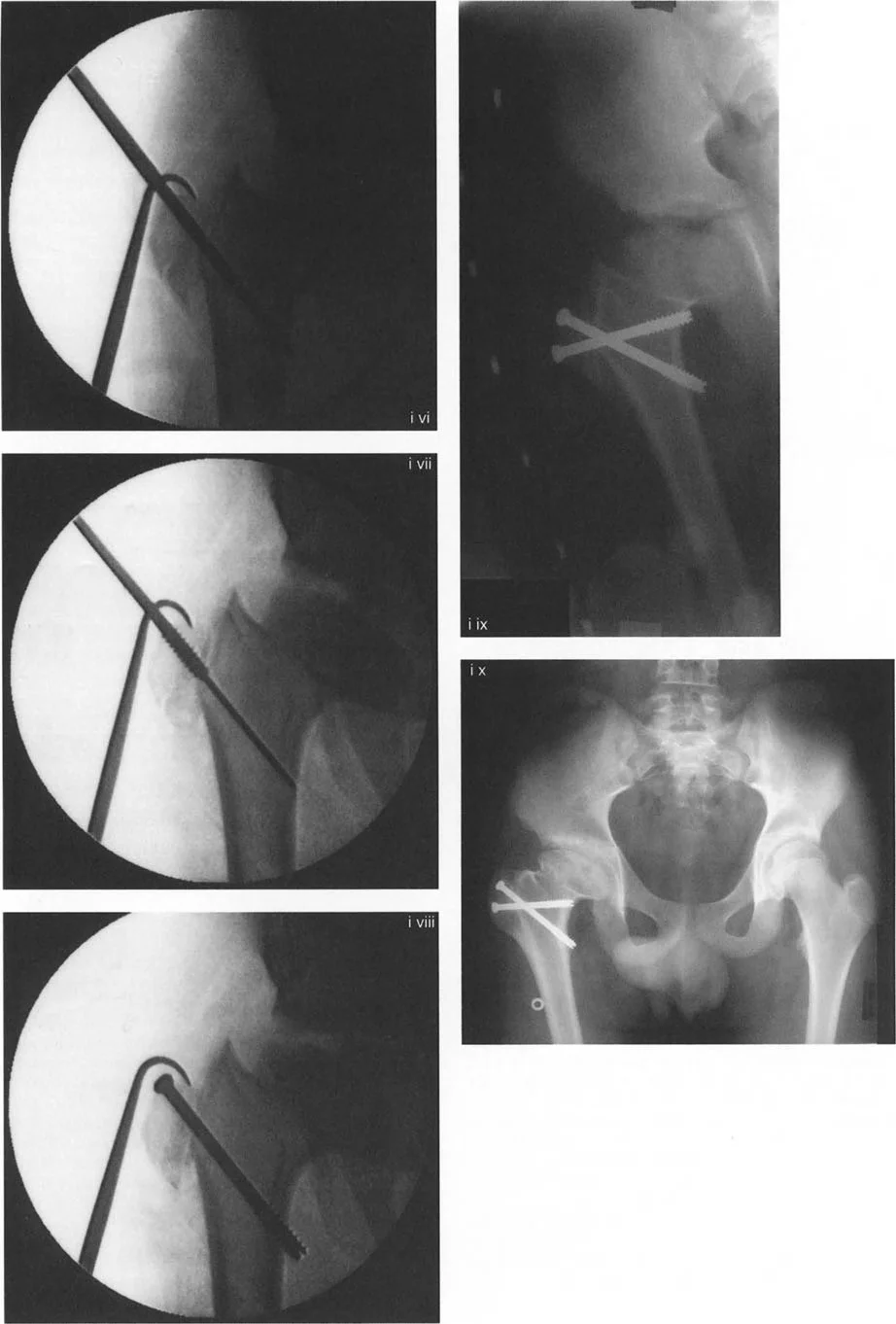
1. Patient Positioning: Supine on a radiolucent flat table or fracture table, ensuring unobstructed fluoroscopic views of the hip and entire femur.
2. Incision and Approach: A standard lateral approach to the proximal femur is utilized. The vastus lateralis is elevated or split to expose the intertrochanteric and subtrochanteric regions.
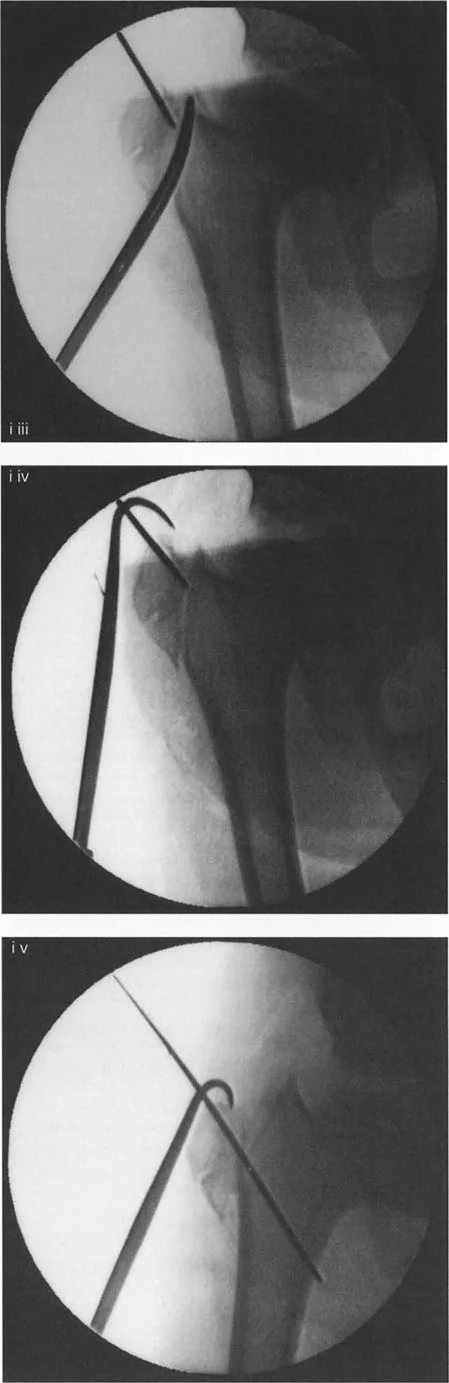
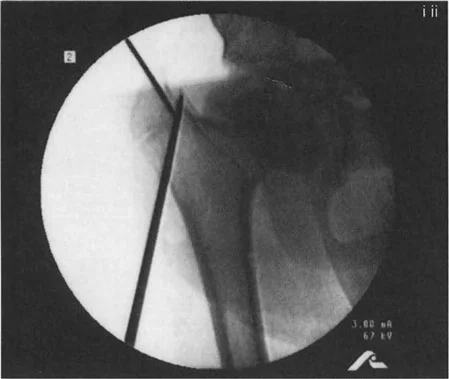
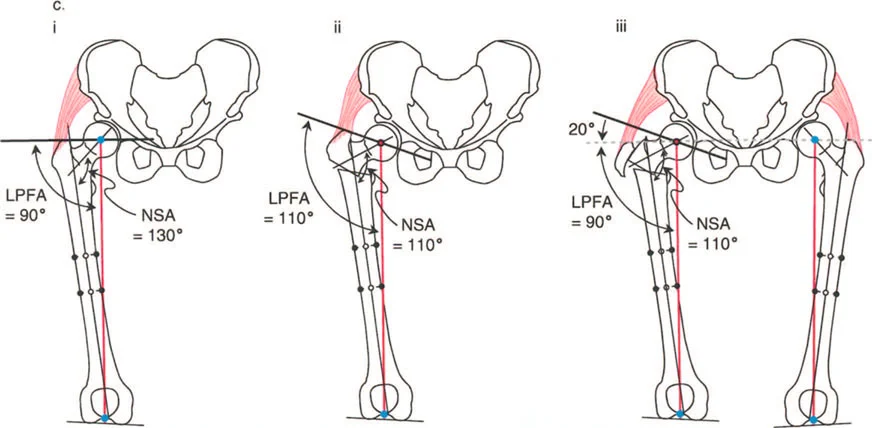
3. Guide Wire Placement: A guide wire is inserted into the femoral neck and head at the predetermined angle (e.g., 90 degrees or 130 degrees, depending on the chosen implant). The trajectory of this wire dictates the final NSA.
4. Osteotomy Execution: A closing wedge or opening wedge osteotomy is performed at the intertrochanteric level.
5. Translation and Realignment: As per Paley Rule 2, the distal fragment is translated medially to realign the mechanical axis.
6. Fixation: The construct is secured using a fixed-angle device.
Varus Producing Intertrochanteric Osteotomy
Varus osteotomies are indicated for coxa valga, hip subluxation in neuromuscular dysplasia, and to improve anterior coverage in developmental dysplasia. The goal is to medialize the mechanical axis, increase the WBF:SA ratio, and improve the containment of the femoral head within the acetabulum.
During a varus osteotomy, a medial closing wedge is typically resected. Because the osteotomy is performed distal to the CORA (which is often in the femoral head for valgus deformities), the distal fragment must be translated laterally to prevent a medial mechanical axis deviation.

Surgical Pearls for Intertrochanteric Osteotomies
* Always release the iliopsoas tendon from the lesser trochanter during significant angular corrections to prevent flexion contractures and excessive joint reaction forces.
* When performing a varus osteotomy, be highly cognizant of the resulting limb length discrepancy. Varus angulation inherently shortens the limb.
* Ensure the guide wire for the seating chisel or proximal locking screws remains strictly within the center-center position of the femoral head on both AP and lateral fluoroscopic views.
Greater Trochanteric Advancement and Transfer
As previously established, restoring the Articulotrochanteric Distance (ATD) is paramount for abductor function. In cases of severe coxa breva or following a varus osteotomy, a concomitant greater trochanteric advancement is required.
The greater trochanter is osteotomized via a digastric approach, preserving the attachments of the gluteus medius and minimus proximally, and the vastus lateralis distally. The trochanteric fragment is then mobilized, transferred distally and laterally, and rigidly fixed to the lateral femoral cortex using heavy non-absorbable sutures, cables, or claw plates. This distal and lateral transfer restores the resting tension of the pelvifemoral musculature and optimizes the abductor moment arm.
Fixation Strategies and Implant Selection
The choice of fixation relies on the patient's age, bone quality, the magnitude of the deformity, and the surgeon's familiarity with the implant systems. The implant must provide absolute stability to allow for early mobilization while resisting the massive bending moments applied to the proximal femur.
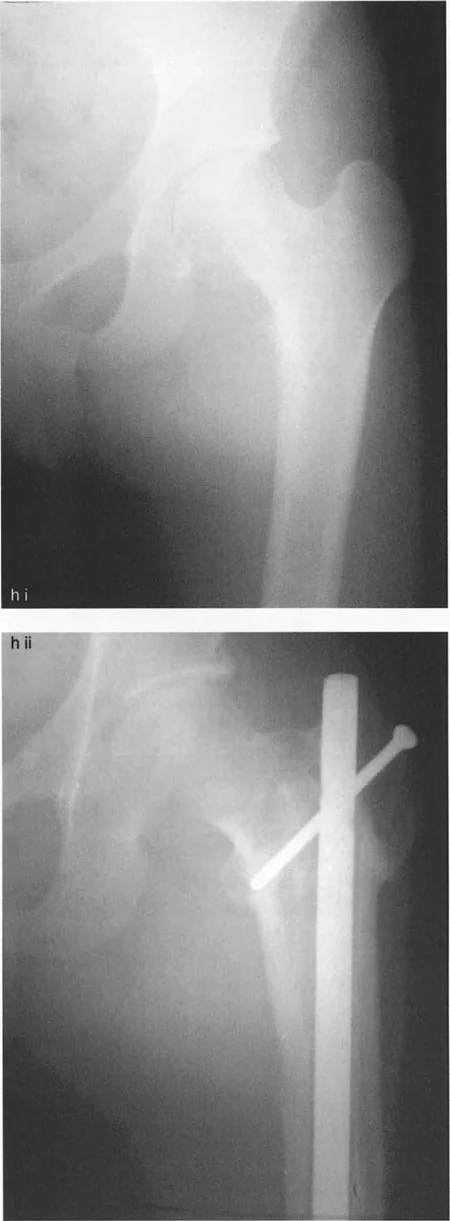
Blade Plates versus Locking Plates
Historically, the angled blade plate (e.g., 90-degree, 130-degree) has been the gold standard for proximal femoral osteotomies. The insertion of a blade plate requires exceptional surgical precision. The seating chisel must be driven into the femoral neck at the exact planned angle in all three planes (coronal, sagittal, and axial). Once the blade is seated and the osteotomy is closed, the plate acts as a rigid, fixed-angle construct that perfectly dictates the final alignment.
In recent years, proximal femoral locking plates (PFLPs) have gained popularity. These plates utilize locking screws rather than a single blade, offering potential advantages in osteoporotic bone or when multiple trajectories are needed to capture a small proximal fragment. However, locking plates do not possess the inherent geometric guidance of a blade plate; the surgeon must manually hold the reduction in perfect alignment while the plate is secured, which can be technically demanding in multiplanar corrections.
Intramedullary Nailing in Proximal Femoral Deformity
For specific deformities, particularly those extending into the subtrochanteric or diaphyseal regions, cephalomedullary nailing may be employed. Nailing offers a load-sharing biomechanical advantage and requires a smaller soft-tissue envelope. However, correcting severe proximal deformities over an intramedullary nail often requires advanced techniques, such as the use of blocking screws (Poller screws) to narrow the medullary canal and direct the nail trajectory, ensuring the osteotomy rules are respected and translation is controlled.
Postoperative Rehabilitation and Clinical Outcomes
The success of a proximal femoral osteotomy is heavily dependent on meticulous postoperative management. The biological healing of the osteotomy and the functional recovery of the soft tissues must be carefully balanced.
Weight Bearing Protocols
- Phase 1 (0 to 6 weeks): Protected weight-bearing is universally instituted. Patients are typically restricted to toe-touch or partial weight-bearing (e.g., 20 pounds) using crutches or a walker. This protects the fixation construct from catastrophic failure due to the high joint reaction forces generated by the abductors during full stance phase.
- Phase 2 (6 to 12 weeks): Progressive weight-bearing is initiated once radiographic evidence of bridging callus is observed at the osteotomy site.
- Phase 3 (3 to 6 months): Intensive physical therapy focuses on restoring abductor strength, normalizing gait mechanics, and eliminating the Trendelenburg limp.
Mitigating Complications in Hip Deformity Correction
Complications in proximal femoral osteotomies can be devastating. Avascular necrosis (AVN) of the femoral head is the most feared complication, typically resulting from iatrogenic injury to the medial femoral circumflex artery during aggressive soft-tissue stripping or misplaced retractors. To mitigate this, dissection should remain strictly extra-capsular unless a concurrent arthrotomy is explicitly indicated.
Non-union or delayed union at the osteotomy site is minimized by ensuring broad bony contact, utilizing rigid fixed-angle compression, and avoiding thermal necrosis during bone cuts. Finally, under-correction or over-correction is avoided by strict adherence to Paley's CORA principles, meticulous preoperative digital templating, and the disciplined execution of intraoperative translation and angulation.
By integrating these biomechanical principles, respecting the joint orientation angles, and executing precise surgical techniques, the orthopedic surgeon can successfully reconstruct the deformed proximal femur, restoring native kinematics and granting the patient a durable, functional, and pain-free hip joint.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like