Chapter 65: Chapter 19

Proximal Femoral Osteotomy and Hip Joint Considerations
The correction of proximal femoral deformities requires a profound understanding of not only osseous anatomy but also the complex soft tissue envelope surrounding the hip joint. Range of motion of the hip is an absolute prerequisite and a primary limiting factor to consider before executing any proximal femoral osteotomy. When planning a deformity correction based on the principles of Dr. Dror Paley, the surgeon must meticulously evaluate the mechanical axis deviation and the specific joint orientation angles, while simultaneously assessing the hip's capacity to accommodate the newly translated or angulated osseous segments.
Range of motion of the hip can be severely limited due to a combination of intraarticular and extraarticular etiologies. Identifying the exact source of this limitation is the first critical step in preoperative planning. Intraarticular loss of range of motion typically stems from capsular contractures, intraarticular adhesions, or a fundamental deformity in the spherical shape of the articular surfaces (such as in Legg-Calvé-Perthes disease or severe developmental dysplasia of the hip). Conversely, extraarticular limitation of range of motion is most frequently driven by muscle contractures, fascial tethering, or the presence of heterotopic ossification.
The presence or absence of these limitations dictates the surgical approach. If the hip cannot physically achieve the position required to neutralize the mechanical axis post-osteotomy, the surgeon must plan for concomitant soft tissue releases or modify the osteotomy design.
Evaluating Intraarticular and Extraarticular Constraints
To systematically approach hip joint limitations, the surgeon must categorize the constraints during the physical examination and radiographic review.
| Constraint Category | Common Etiologies | Clinical Implications for Osteotomy |
|---|---|---|
| Intraarticular | Capsular contracture, synovial adhesions, aspherical femoral head, acetabular dysplasia, labral pathology. | May require capsulotomy, surgical dislocation, or osteochondroplasty prior to or concurrent with osteotomy. |
| Extraarticular | Muscle contracture (abductors, adductors, flexors), tensor fascia lata tightness, heterotopic ossification, piriformis tethering. | Requires targeted tenotomies, muscle slides (e.g., Paley abductor release), or excision of heterotopic bone. |

Paley Principles of Proximal Femoral Deformity
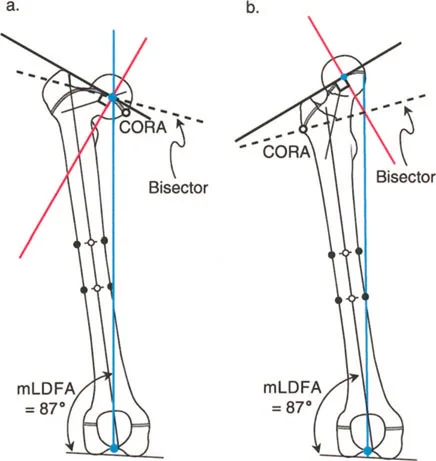
Before delving into the specific management of varus deformities, it is essential to establish the foundational Paley principles governing the proximal femur. Deformity correction relies on identifying the Center of Rotation of Angulation and understanding its relationship to the Mechanical Axis Deviation.
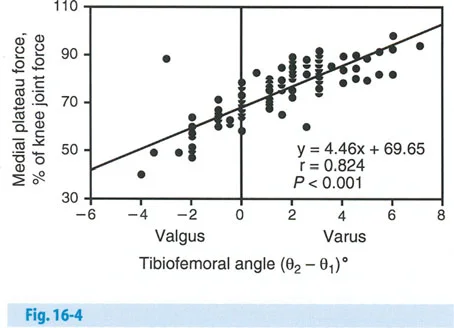
When a varus deformity exists in the proximal femur (coxa vara), the mechanical axis of the lower extremity is shifted medially, leading to a medial Mechanical Axis Deviation. This medial shift drastically alters the load-bearing biomechanics of the knee and ankle, predisposing the patient to premature medial compartment osteoarthritis.

Proximal Femoral Joint Orientation Angles
Accurate preoperative planning requires the measurement of specific joint orientation angles on a standing anteroposterior radiograph. The primary angles evaluated in the proximal femur include
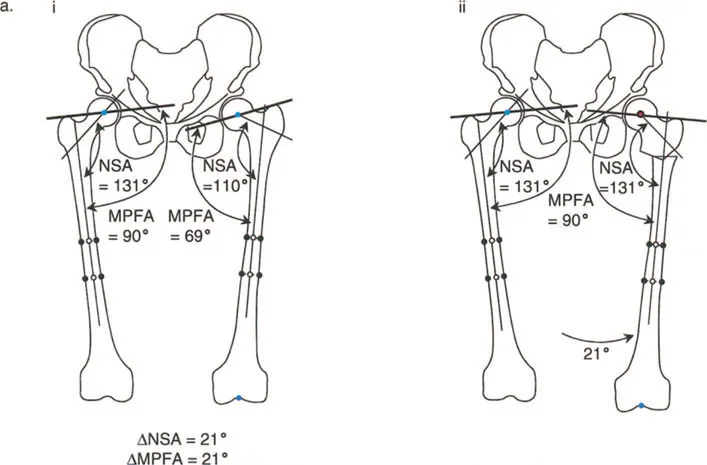
- Neck Shaft Angle (NSA) The angle between the anatomical axis of the femoral shaft and the axis of the femoral neck. Normal is approximately 130 degrees. In varus deformities, this angle is significantly decreased.
- Medial Proximal Femoral Angle (MPFA) The medial angle formed between the mechanical axis of the femur and the proximal joint line of the femur (tip of the greater trochanter to the center of the femoral head). Normal is approximately 84 degrees.
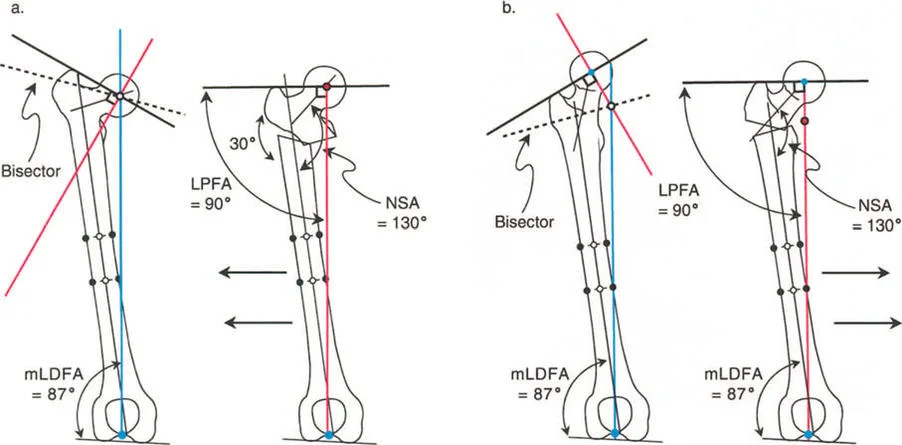
- Lateral Proximal Femoral Angle (LPFA) The lateral angle formed between the mechanical axis of the femur and the proximal joint line. Normal is approximately 90 degrees.
By utilizing these angles, the surgeon can pinpoint the exact magnitude and apex of the deformity, allowing for the precise application of the Osteotomy Rules.
Pathomechanics of Varus Deformity of the Hip
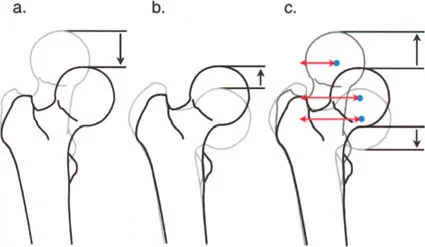
Varus deformity of the hip, or coxa vara, presents a unique biomechanical challenge. In a normal hip, the abductor musculature (gluteus medius and minimus) operates with an optimal lever arm to maintain pelvic stability during the single leg stance phase of gait. In coxa vara, the greater trochanter is elevated relative to the center of rotation of the femoral head. This shortens the functional length of the abductor muscles and decreases their mechanical advantage, resulting in a classic Trendelenburg gait.
When the limb is in neutral alignment to the pelvis and there is no intraarticular or periarticular limitation of range of motion, the primary goal is to restore the normal Neck Shaft Angle and Medial Proximal Femoral Angle.
Biomechanical Implications of Coxa Vara
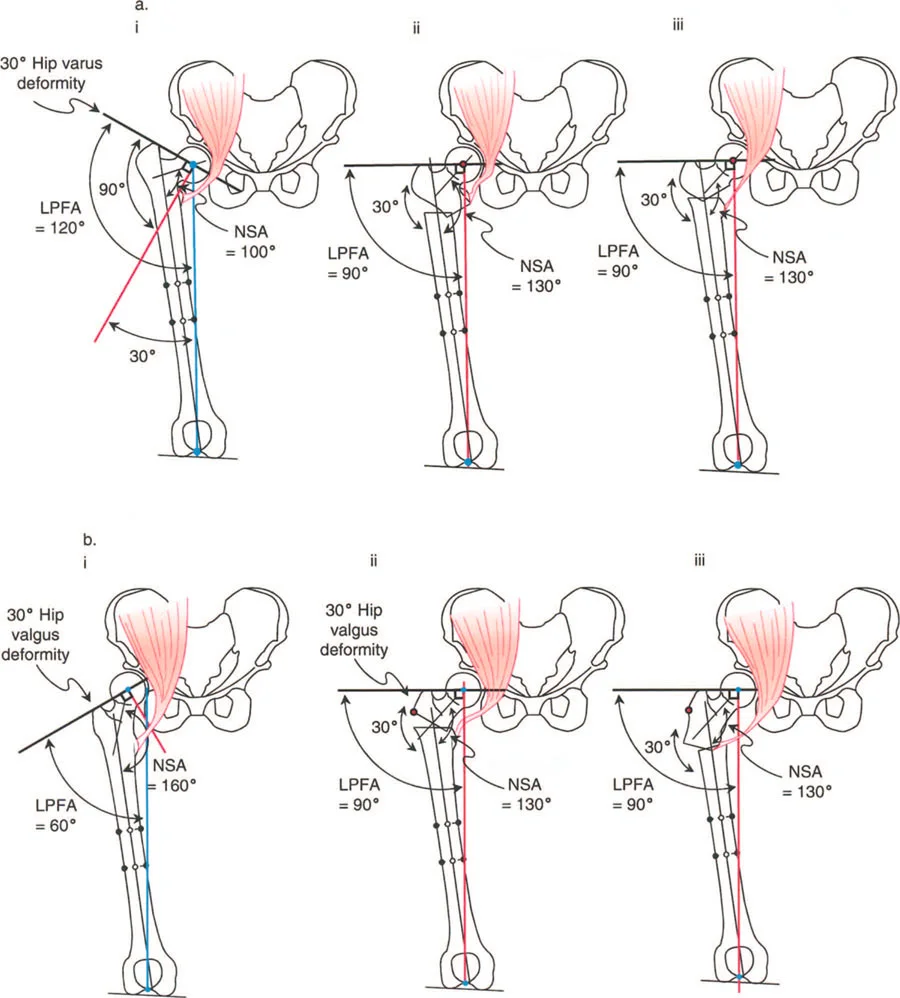
A thirty degree varus hip deformity typically presents with an LPFA of 120 degrees and an NSA of 100 degrees. In this state, the proximal femur is severely structurally compromised. The shear forces across the femoral neck are exponentially increased, which in pediatric populations can lead to progressive worsening of the varus deformity or failure of the proximal femoral physis. Correction of this deformity requires a valgus-producing osteotomy.
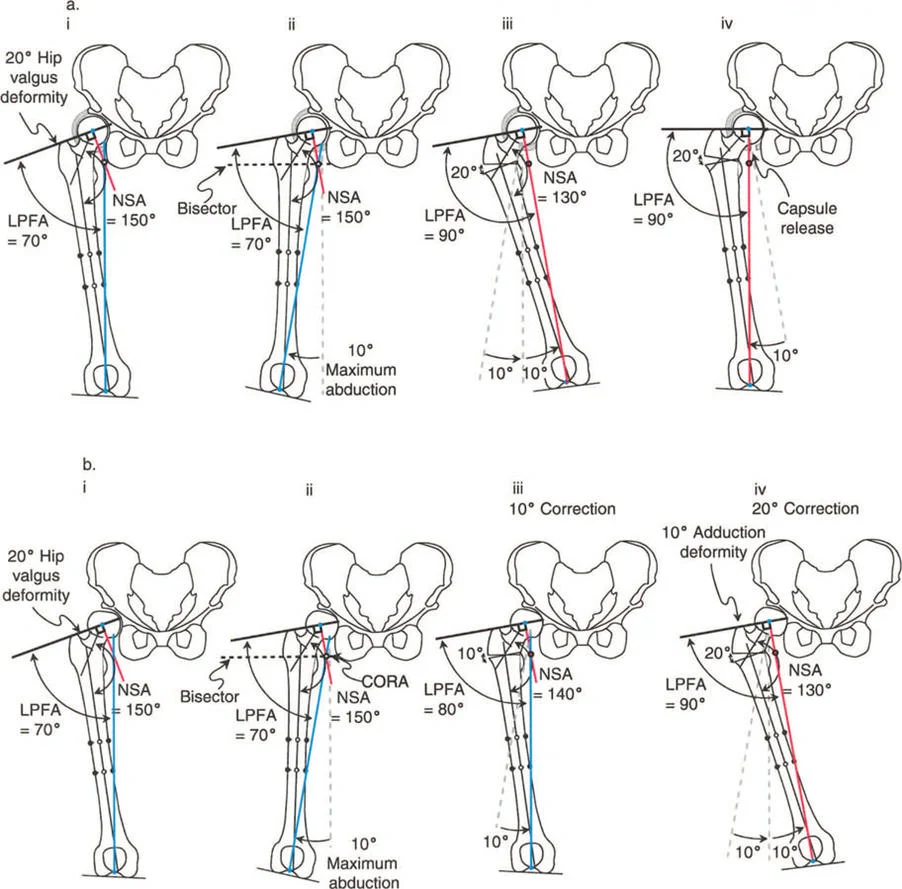
Executing the Valgus Osteotomy
The surgical correction of a varus deformity necessitates a valgus osteotomy. However, the execution of this osteotomy is entirely dependent on the hip joint's ability to accommodate the correction. Specifically, a valgus osteotomy requires adequate adduction of the femoral head within the acetabulum.
When the distal femoral segment is abducted to create valgus at the osteotomy site, the proximal segment (the femoral head and neck) must rotate into adduction within the joint to allow the distal limb to return to a neutral mechanical alignment. If the hip cannot adduct, the entire lower extremity will be forced into fixed abduction.
Managing the Adductor Complex
The adductor musculature plays a paradoxical role during valgus osteotomy. While one might assume the adductors would become lax as the distal femur is abducted, the geometric reality of the correction often results in a lengthening effect on the medial side of the femur.
As the varus deformity is corrected into valgus, the effective length of the femur increases, and the medial soft tissue envelope is placed under significant tension. Consequently, an adductor tenotomy is frequently required after a valgus osteotomy.
Performing an adductor tenotomy serves two vital functions
1. It facilitates the valgus osteotomy by removing a medial tether.
2. It improves postoperative hip abduction and relieves excessive compressive pressure on the femoral head, which is critical for preventing avascular necrosis or chondrolysis.
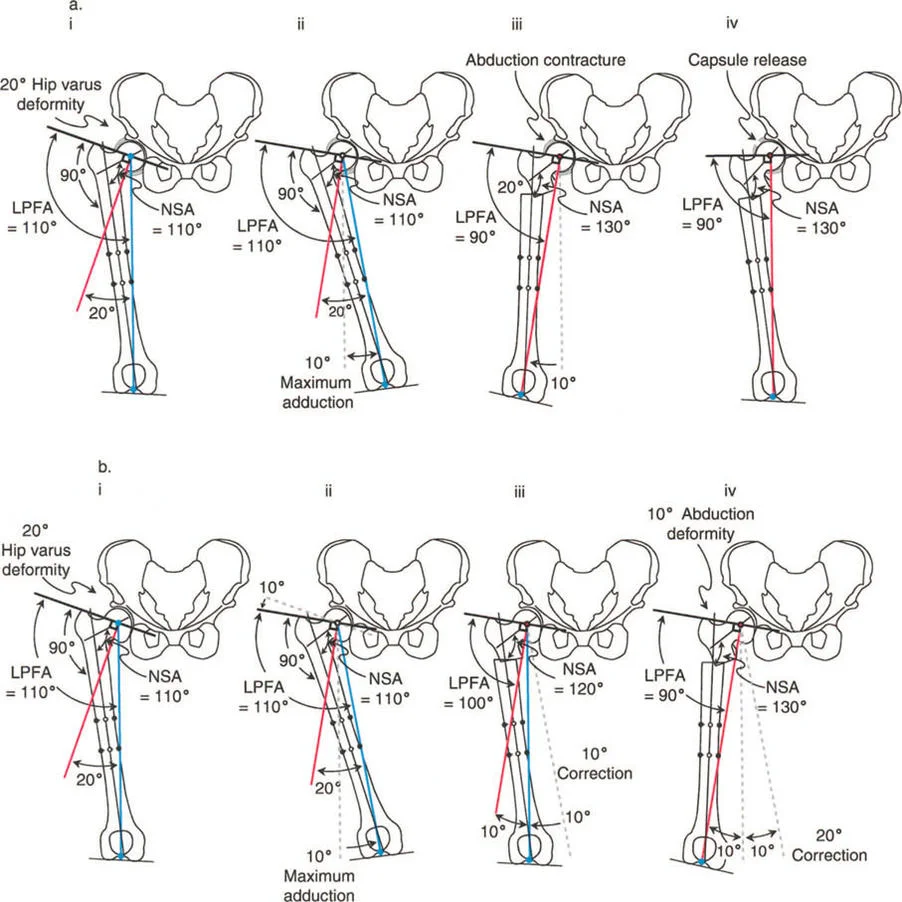
Overcoming Extraarticular Abduction Contractures
While the adductors present a medial challenge, the major extraarticular limitations to the necessary adduction of the proximal femoral segment are found laterally. The tensor fascia lata, gluteus medius, and gluteus minimus muscles act as a formidable lateral tether.
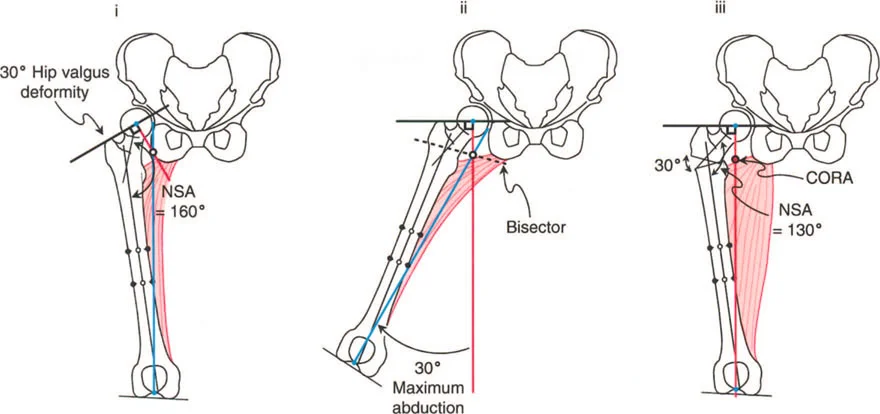
During preoperative evaluation, if the maximum hip adduction is restricted (for example, limited to only 10 degrees or 30 degrees), the surgeon must anticipate an abduction contracture post osteotomy. If a 30 degree valgus osteotomy is performed on a hip that only allows 10 degrees of adduction, the distal limb will remain in 20 degrees of fixed abduction immediately after the correction.

Natural History of Postoperative Abduction Contractures
The management of an iatrogenic abduction contracture depends heavily on the etiology of the underlying varus deformity. Because of the long lever arm of the lower extremity, gravity and the weight of the leg exert a constant adduction force during ambulation and rest.
In acquired or flexible deformities, this long lever arm, combined with aggressive physical therapy, may be sufficient to stretch the abductor complex over time. In these cases, the abduction contracture may resolve spontaneously, eventually allowing the limb to come into neutral alignment relative to the pelvis.
However, children with coxa vara due to congenital causes (such as Congenital Femoral Deficiency) possess fundamentally different soft tissue biology. In congenital cases, the fibrotic and foreshortened abductor musculature will not stretch out. The abduction contracture becomes a rigid, fixed deformity, leading to pelvic obliquity, apparent leg length discrepancy, and severe gait pathology. These patients require additional, specialized surgical intervention to lengthen the abductor mechanism.
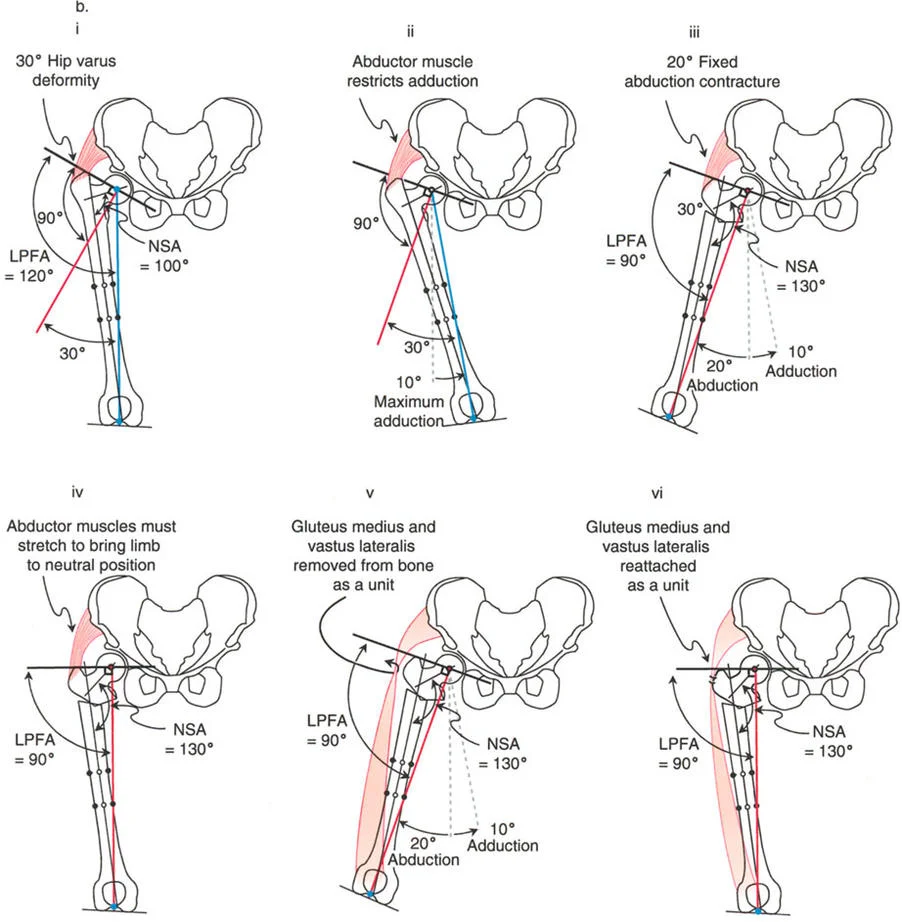
The Paley Abductor Release Technique
To address the severe abduction contractures seen in congenital coxa vara, Dr. Dror Paley developed a novel surgical procedure in 1998. The goal of this procedure is to reposition the hip and allow for massive valgus correction without permanently weakening the critical abductor mechanism.
Traditional fractional lengthenings or complete tenotomies of the gluteus medius and minimus often result in a catastrophic loss of abductor power, leaving the patient with a permanent Trendelenburg lurch. The Paley technique circumvents this by utilizing the anatomical continuity of the lateral musculature.
Anatomical Basis of the Procedure
The Paley abductor release involves the removal of the entire insertion of the gluteus medius and minimus from the greater trochanter in direct continuity with the origin of the vastus lateralis.
This technique is conceptually based on the Hardinge (or Stracathro) approach to the hip, originally described by McLauchlan in 1984. The Hardinge approach removes the anterior third of the gluteus medius and the vastus lateralis as a single, continuous unit. The Paley technique expands upon this by elevating the entirety of the gluteal insertion in continuity with the quadriceps envelope.
Because the gluteal muscles remain in continuity with the vastus lateralis through their conjoint fascial expansion, the entire muscle complex acts as a single unit. Crucially, because they are in continuity, they cannot retract or shorten proximally into the ilium.
Step by Step Surgical Execution
- Surgical Exposure A direct lateral approach to the proximal femur is utilized. The tensor fascia lata is incised longitudinally and lengthened to relieve the primary lateral fascial tether.
- Elevation of the Conjoint Tendon The insertion of the gluteus medius and minimus is identified on the greater trochanter. The origin of the vastus lateralis is identified on the vastus ridge. The entire complex is elevated subperiosteally from the bone as a single, continuous sleeve.
- Piriformis Release It is mandatory to isolate and release the piriformis tendon. The piriformis acts as a potent external rotator and abductor. If left intact, it will severely restrict internal rotation, extension, and the required adduction of the proximal segment.
- Execution of the Osteotomy With the greater trochanter completely free from the extraarticular abduction contracture, the subtrochanteric valgus osteotomy is performed. The proximal femur can now be adducted freely within the constraints of the capsular attachments.
- Reattachment After the osteotomy is stabilized and the varus deformity is corrected, the abductor quadriceps unit is drawn back over the greater trochanter. The conjoint tendon is firmly sutured to the greater trochanter in its new, relatively distal position.
By detaching the gluteal muscles and lengthening the tensor fascia lata, the surgeon uncouples the proximal femoral bone segment from the soft tissue restraints, allowing for massive angular corrections.
Congenital Coxa Vara and Congenital Femoral Deficiency
The true test of these principles is seen in cases of Congenital Femoral Deficiency (CFD) associated with marked congenital coxa vara. These deformities are not merely angular; they represent a global hypoplasia and malorientation of the entire proximal femur.
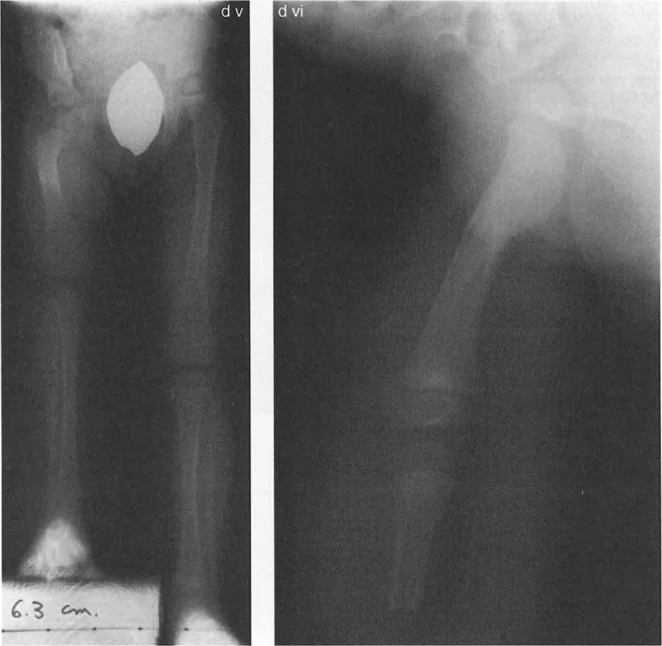
Consider a severe case of congenital coxa vara where the anteroposterior radiograph reveals an MPFA of 15 degrees and an NSA of 60 degrees. To restore normal biomechanics (a normal MPFA of 85 degrees and an NSA of 130 degrees), a massive 70 degree valgus correction is required.
Preoperative Assessment of Severe Deformity
In such extreme cases, a maximum adduction radiograph is mandatory. If the maximum adduction radiograph shows only 20 degrees of adduction limited by the soft tissues, there is a massive deficit. The required 70 degree correction minus the available 20 degrees of adduction leaves the surgeon facing a 50 degree abduction contracture of the hip if soft tissue releases are not performed.
This mathematical certainty dictates the surgical plan. The Paley abductor release in continuity with the vastus lateralis must be utilized.
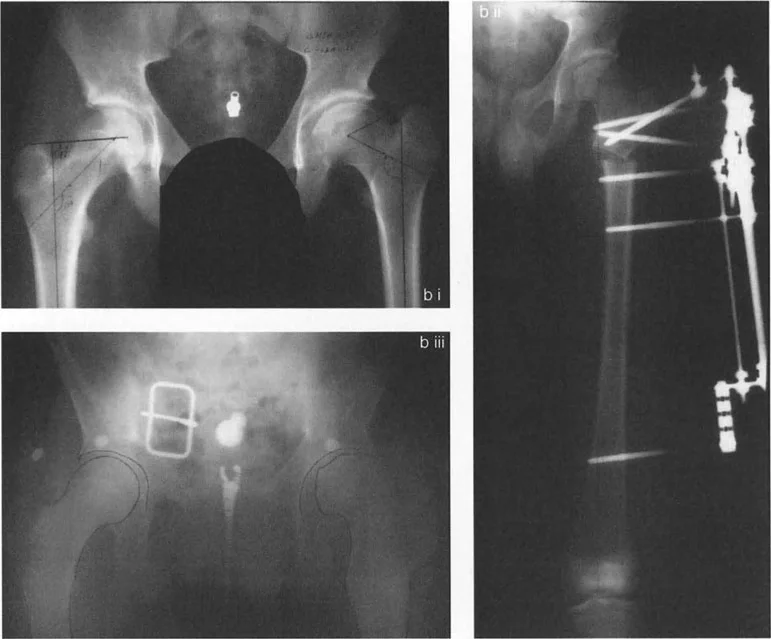
Subtrochanteric Osteotomy and Internal Fixation
Once the hip abductors are removed from the greater trochanter in continuity with the quadriceps muscle, the proximal segment is no longer tethered. It can be manually adducted by pulling the greater trochanter away from the pelvis.
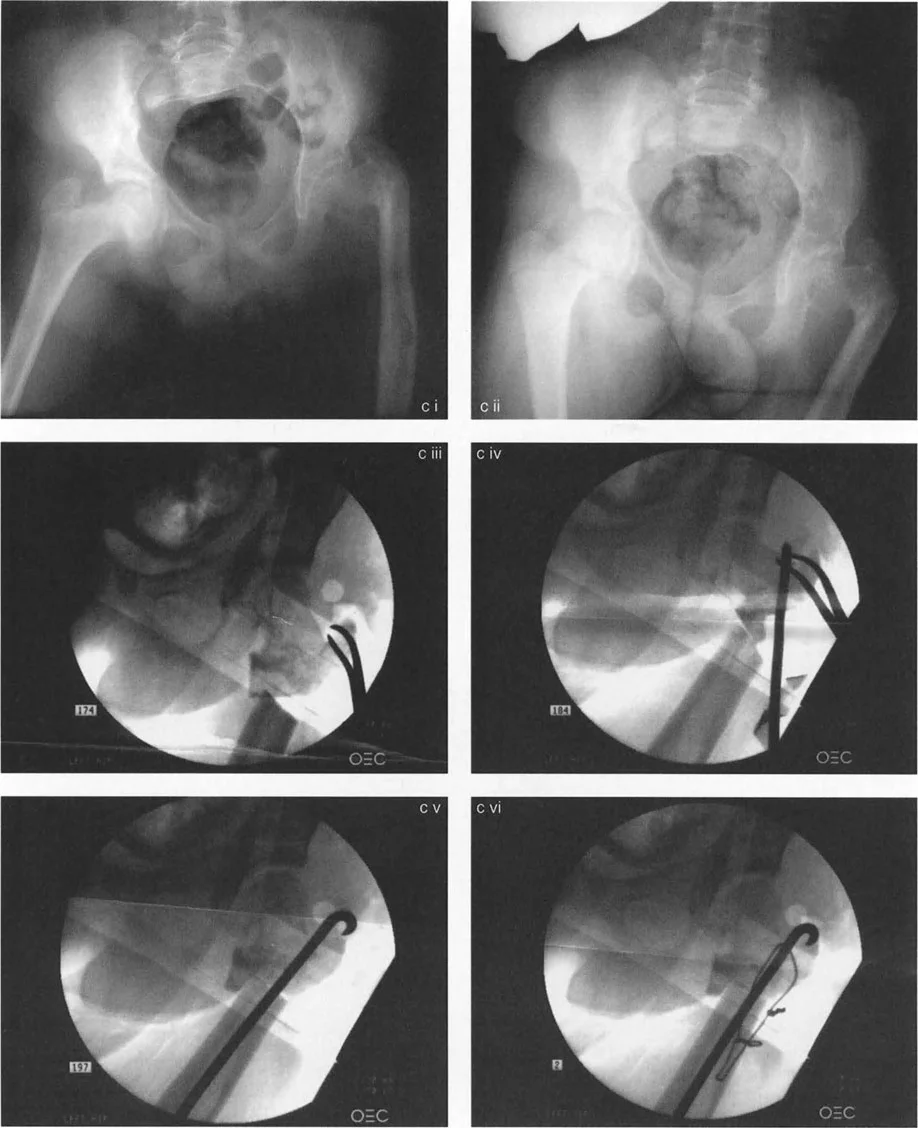
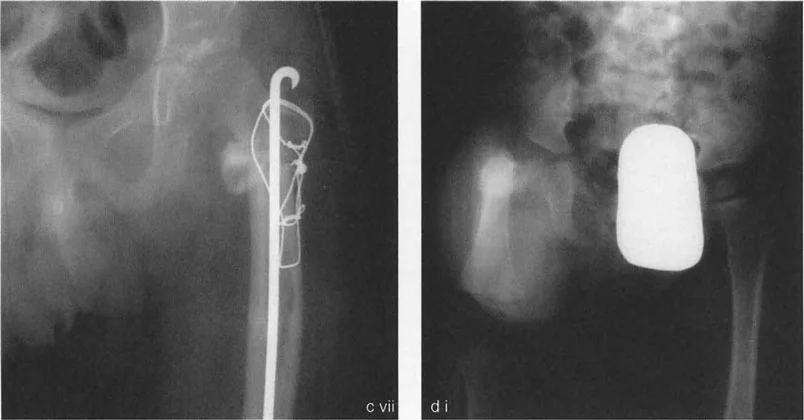
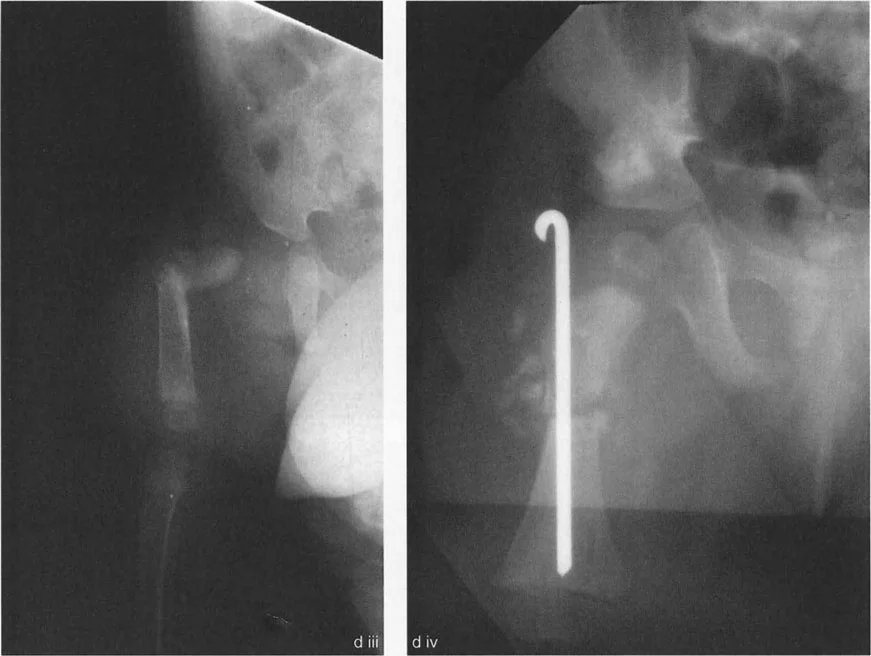
The subtrochanteric osteotomy is then executed. Fixation in these complex pediatric cases requires robust, specialized techniques.
- Preparation of the Intramedullary Path The path of the intramedullary nail is drilled directly into the piriformis fossa. Due to the extreme varus deformity, this path often exits through what was historically the lateral cortex of the upper femur.
- Osteotomy Interdigitation To ensure rotational stability and a high rate of union, a slot is cut in the distal femur perpendicular to the path of the rod. This assures a better geometric fit between the proximal and distal segments.
- Hardware Insertion The rod is passed across the osteotomy site into the lower segment, locking the valgus correction in place.
- Compression A tension band wire is frequently utilized in conjunction with the intramedullary device. The tension band wire is applied to compress and close the lateral opening wedge of the osteotomy site, converting tensile forces into compressive forces to promote rapid bone healing.

Following rigid fixation, a final intraoperative radiograph is obtained to confirm the restoration of the joint orientation angles. Achieving a final MPFA of 85 degrees and an NSA of 130 degrees signifies a complete anatomical correction. The conjoint tendon of the gluteus and vastus lateralis is then resutured to the greater trochanter in the newly corrected position.

Addressing Concurrent Sagittal Plane Deformities
Congenital femoral deficiency rarely presents as an isolated coronal plane deformity. Marked coxa vara is frequently accompanied by a bony hip extension deformity. When viewing the preoperative radiographs, the severe torsional and sagittal plane abnormalities can be confusing. Often, on an AP view, the upper femur appears as a lateral projection, while the lower femur appears as a true AP projection due to severe internal torsion.
The surgeon must account for this multiplanar deformity. The osteotomy must not only create valgus but also correct the version (rotation) and flexion/extension abnormalities. The release of the piriformis, as mentioned earlier, is particularly crucial here, as it allows the proximal segment to be rotated internally and flexed to match the distal segment, restoring a normalized sagittal and axial profile.
Postoperative Rehabilitation and Clinical Pearls
The success of a proximal femoral osteotomy relying on the Paley abductor release technique depends heavily on meticulous postoperative care.
Surgical Pearls for the Orthopedic Surgeon
- Respect the Center of Rotation of Angulation Always template your osteotomy based on the CORA. Failing to translate the bone segments appropriately at the osteotomy site will result in a secondary mechanical axis deviation.
- Anticipate the Adductor Tightening Remember the geometric reality a valgus osteotomy lengthens the medial column. Have a low threshold for performing an adductor tenotomy to protect the hip joint from excessive contact pressures.
- Do Not Compromise the Abductors Never perform a free tenotomy of the gluteus medius or minimus in a pediatric patient with congenital coxa vara. Always utilize the Paley technique of elevating the glutei in continuity with the vastus lateralis to preserve the abductor lever arm.
- Release the Piriformis The piriformis is a hidden tether. If you are struggling to adduct or internally rotate the proximal segment after elevating the abductors, the piriformis is likely the culprit.
- Utilize Tension Band Principles In subtrochanteric osteotomies, the lateral cortex is under immense tension. Supplementing your intramedullary fixation with a lateral tension band wire drastically increases construct stability and union rates.
Rehabilitation Guidelines
Postoperatively, patients are typically placed in a spica cast or highly restrictive orthosis depending on the rigidity of the internal fixation and the age of the patient. Because the abductor mechanism was detached and reattached, active abduction is strictly prohibited for the first 6 weeks to allow for tendinous healing to the greater trochanter.
Passive range of motion, particularly focusing on maintaining the newly acquired adduction and flexion, is initiated early. Once radiographic union is evident at the osteotomy site and the conjoint tendon has healed, an aggressive physical therapy regimen focusing on abductor strengthening and gait retraining is essential to overcome the historical Trendelenburg gait and maximize the functional outcome of the deformity correction.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like