Precision Sagittal Plane Knee Deformity Correction: Paley Principles & Osteotomy Techniques
Key Takeaway
Sagittal plane knee deformities (genu recurvatum, fixed flexion) are corrected using Paley Principles. This involves identifying the Center of Rotation of Angulation (CORA) and performing precise osteotomies based on joint orientation angles (PDFA, PPTA) to restore normal alignment.
Comprehensive Guide to Sagittal Plane Knee Considerations
The evaluation and management of lower extremity deformities require a profound understanding of three-dimensional spatial geometry. While coronal plane alignments often dominate initial clinical assessments, sagittal plane knee considerations are equally critical for restoring normal gait kinematics, optimizing extensor mechanism function, and preventing early joint degeneration. Deformities in the sagittal plane—specifically genu recurvatum (hyperextension) and fixed flexion deformities (FFD)—present unique challenges because they frequently involve a complex interplay between bony malalignment and soft tissue contractures.
This comprehensive guide translates the foundational principles of Dr. Dror Paley into an actionable, high-yield resource for orthopedic surgeons, residents, and fellows. By mastering the Center of Rotation of Angulation (CORA), Mechanical Axis Deviation (MAD), and specific joint orientation angles, surgeons can accurately diagnose and execute precise osteotomies for sagittal knee deformities.
Paley Principles in the Sagittal Plane
To successfully correct sagittal plane deformities, the surgeon must first quantify the deformity using standardized radiographic parameters. Dr. Paley’s principles dictate that every deformity has a CORA, and identifying this point is the cornerstone of preoperative planning.
In the sagittal plane, the mechanical and anatomical axes of the tibia are essentially parallel and collinear. For the femur, the anatomical axis exhibits an anterior bow, which must be accounted for when drawing mid-diaphyseal lines. The key joint orientation angles used to evaluate the sagittal knee are the Posterior Distal Femoral Angle (PDFA) and the Posterior Proximal Tibial Angle (PPTA).
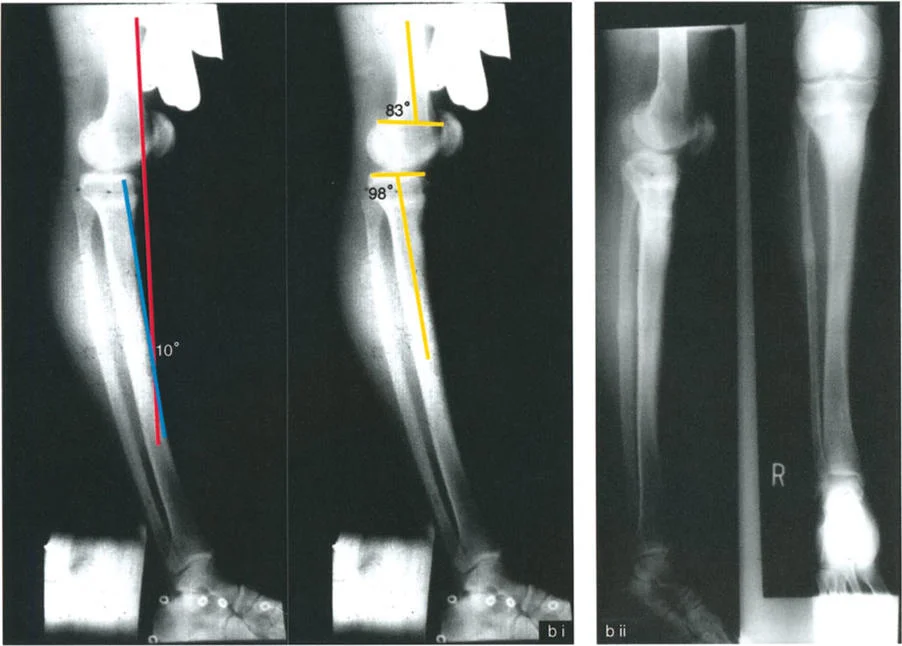
- Posterior Distal Femoral Angle (PDFA) The normal PDFA is approximately 83 degrees. An increased PDFA indicates distal femoral recurvatum (extension deformity), whereas a decreased PDFA indicates a flexion deformity (procurvatum).
- Posterior Proximal Tibial Angle (PPTA) The normal PPTA is approximately 81 degrees. An increased PPTA indicates proximal tibial recurvatum, while a decreased PPTA indicates proximal tibial procurvatum.
When evaluating a patient with a hyperextended knee, the surgeon must determine whether the deformity originates in the femur, the tibia, the soft tissues, or a combination thereof. This distinction dictates the entire surgical approach.
Defining the Center of Rotation of Angulation
The CORA is the intersection of the proximal and distal mechanical or anatomical axis lines of a deformed bone segment. In the sagittal plane, locating the CORA accurately ensures that the subsequent osteotomy restores normal joint orientation without introducing secondary translational deformities.
Paley’s Osteotomy Rules apply directly to the sagittal plane
1. Rule 1 When the osteotomy and the hinge (axis of correction) are placed at the CORA, pure angular correction is achieved without translation.
2. Rule 2 When the hinge is at the CORA but the osteotomy is made at a different level, the correction will result in angulation and intentional translation. This is highly relevant when avoiding the patellar tendon insertion.
3. Rule 3 When the hinge and the osteotomy are both outside the CORA, a secondary translation deformity will be induced, which is generally undesirable unless planned for specific mechanical advantages.
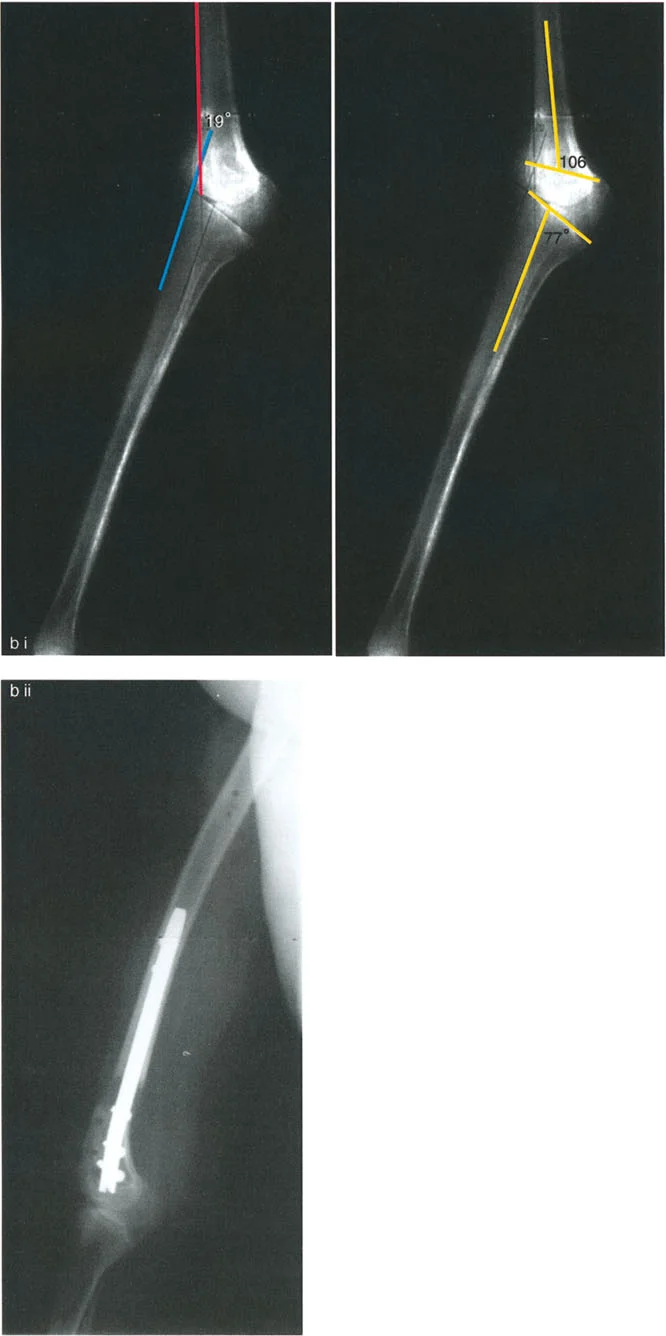
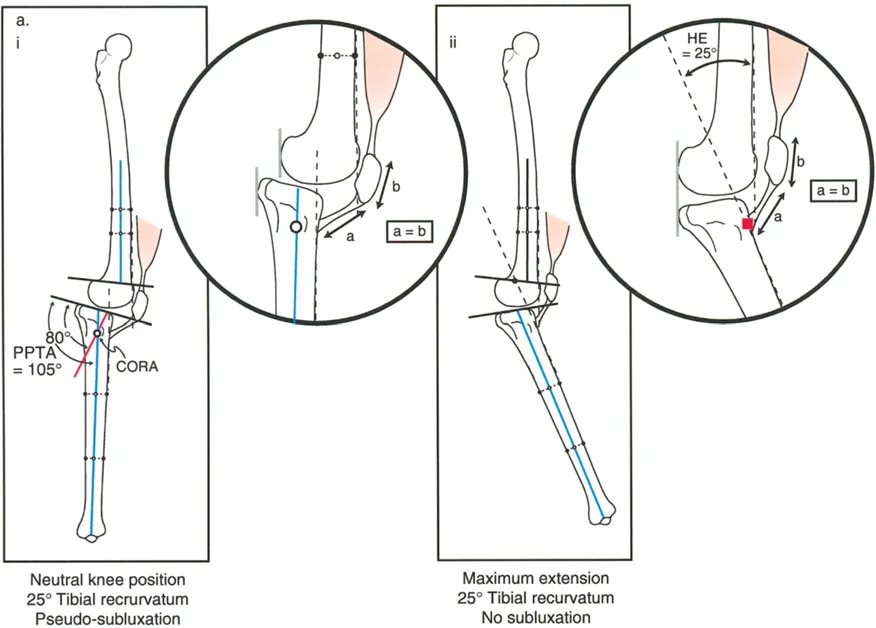
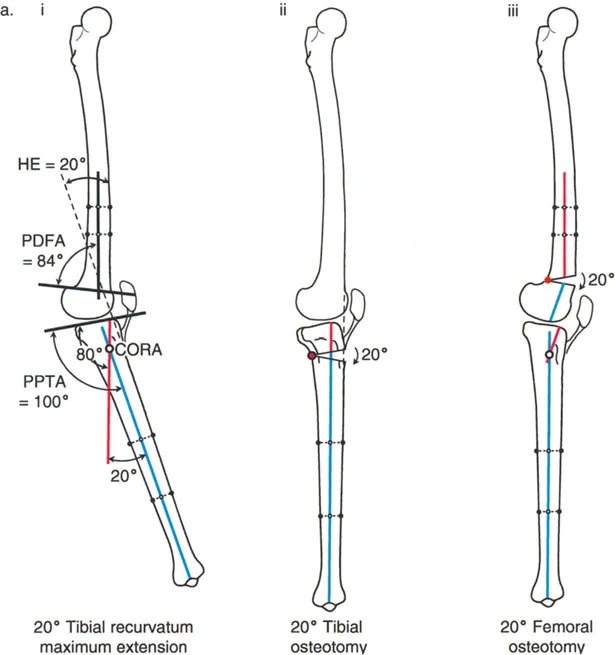
Proximal Tibial Recurvatum and Patellar Tendon Kinematics
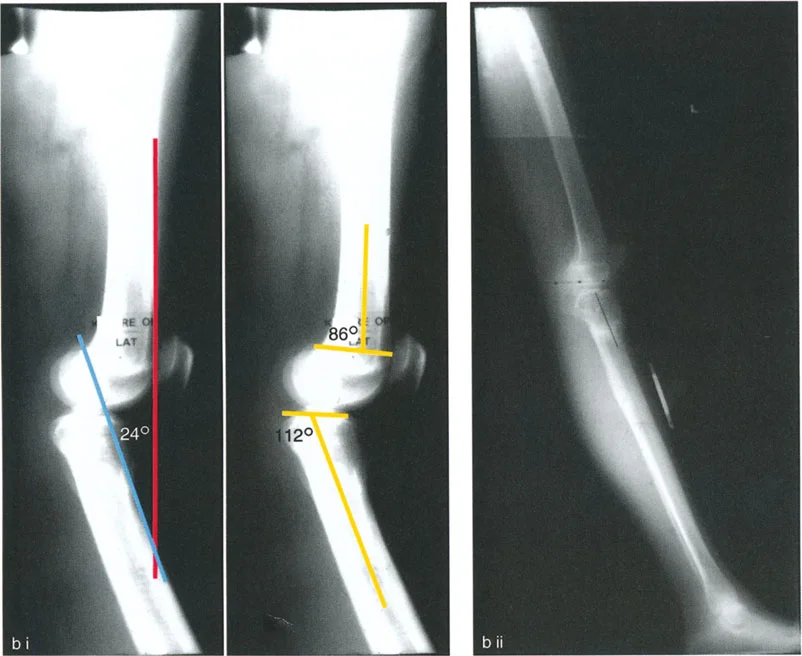
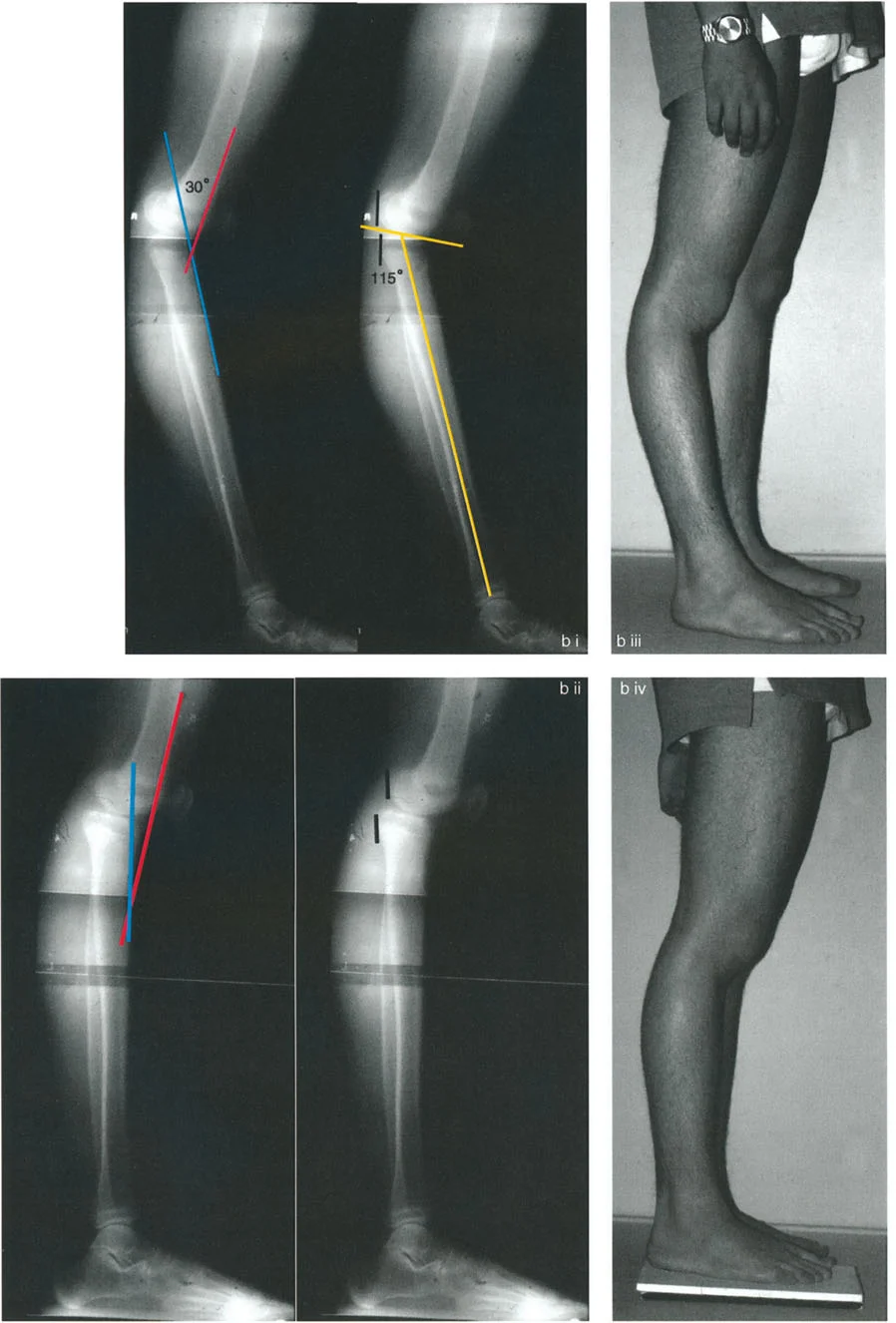
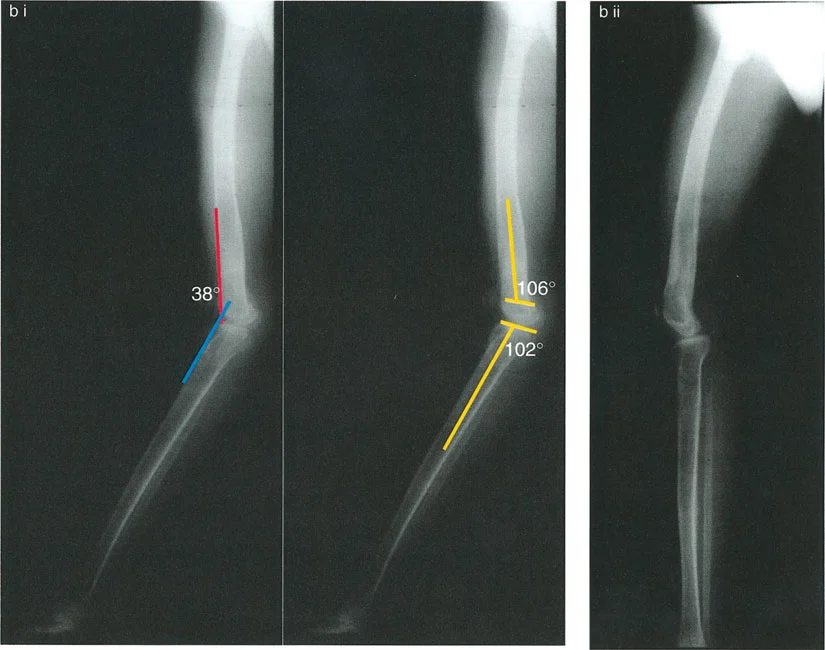
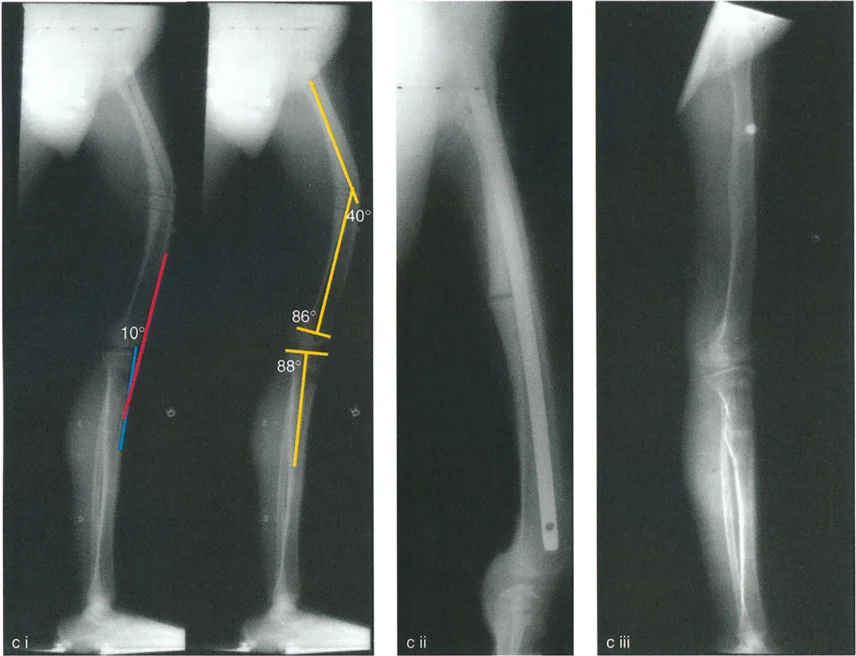
Proximal tibial recurvatum is a challenging deformity characterized by a posteriorly tilted tibial plateau (increased PPTA). Patients typically present with clinical genu recurvatum, anterior knee pain, and an apparent extensor lag due to the altered mechanics of the patellofemoral joint.
Determining the Level of the Osteotomy
When planning an osteotomy to correct proximal tibial recurvatum, the surgeon must critically evaluate the level of the patellar tendon insertion. The relationship between the tibial tuberosity and the joint line dictates the osteotomy level to prevent iatrogenic complications such as patella baja.
Normal Patellar Tendon Insertion
If the patellar tendon insertion is at a normal anatomical level, the osteotomy must be performed distal to the tibial tuberosity. Performing an opening wedge correction proximal to a normally positioned tuberosity would distalize the tuberosity relative to the joint line, creating a severe patella baja. This alters patellofemoral tracking, increases contact pressures, and can lead to debilitating anterior knee pain.
Abnormally Proximal Patellar Tendon Insertion
In many congenital or developmental recurvatum deformities, the patellar tendon insertion migrates proximally. In this specific scenario, the osteotomy should be executed proximal to the tibial tuberosity.
Performing an opening wedge osteotomy proximal to the tuberosity in this patient population provides several distinct biomechanical advantages
* It brings the abnormally proximal patellar tendon back down to its normal anatomical level.
* The tension created on the patellar tendon pulls the tibia forward, indirectly reducing posterior knee subluxation.
* It restores the normal PPTA without compromising the extensor mechanism.
Indirect Reduction via Fibular Transport
A powerful adjunctive technique in correcting tibial recurvatum with posterior subluxation is the manipulation of the fibula. The Lateral Collateral Ligament (LCL) connects the lateral femoral epicondyle to the fibular head and is oriented in an anteroposterior direction.
By combining the recurvatum correction with distal transport of the fibula, the surgeon places tension on the LCL. This tension pulls the lateral side of the tibia anteriorly, aiding in the indirect reduction of the subluxed knee joint. The combined tension on the LCL and the patellar tendon creates a robust anterior vector, restoring joint congruency.
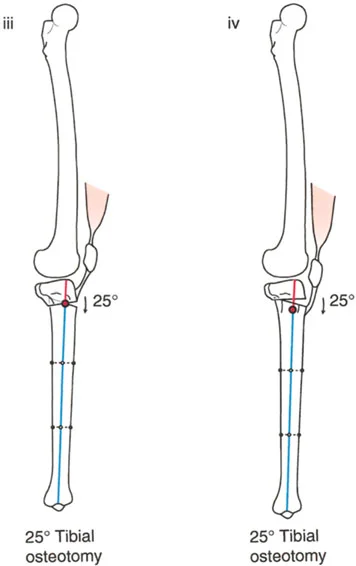
Unmasking Flexion Contractures in Tibial Osteotomies
Surgeons must be acutely aware of preoperative soft tissue status. If a patient has a true posterior subluxation and an associated soft tissue flexion contracture of the knee, performing an osteotomy proximal to the tuberosity will achieve indirect bony reduction but will simultaneously unmask the flexion contracture. The bone is corrected, but the posterior soft tissues (capsule, gastrocnemius, hamstrings) remain tight, resulting in a postoperative inability to fully extend the knee.
Femoral Recurvatum Deformities
Distal femoral recurvatum is characterized by an increased PDFA. Unlike tibial deformities which directly affect the plateau slope, femoral recurvatum alters the arc of motion of the knee joint, shifting the entire arc into hyperextension.
To understand the treatment algorithms, we must analyze the interplay between the bony deformity and the compensatory soft tissue adaptations. Dr. Paley categorizes these into distinct clinical scenarios based on the presence and magnitude of associated flexion contractures.
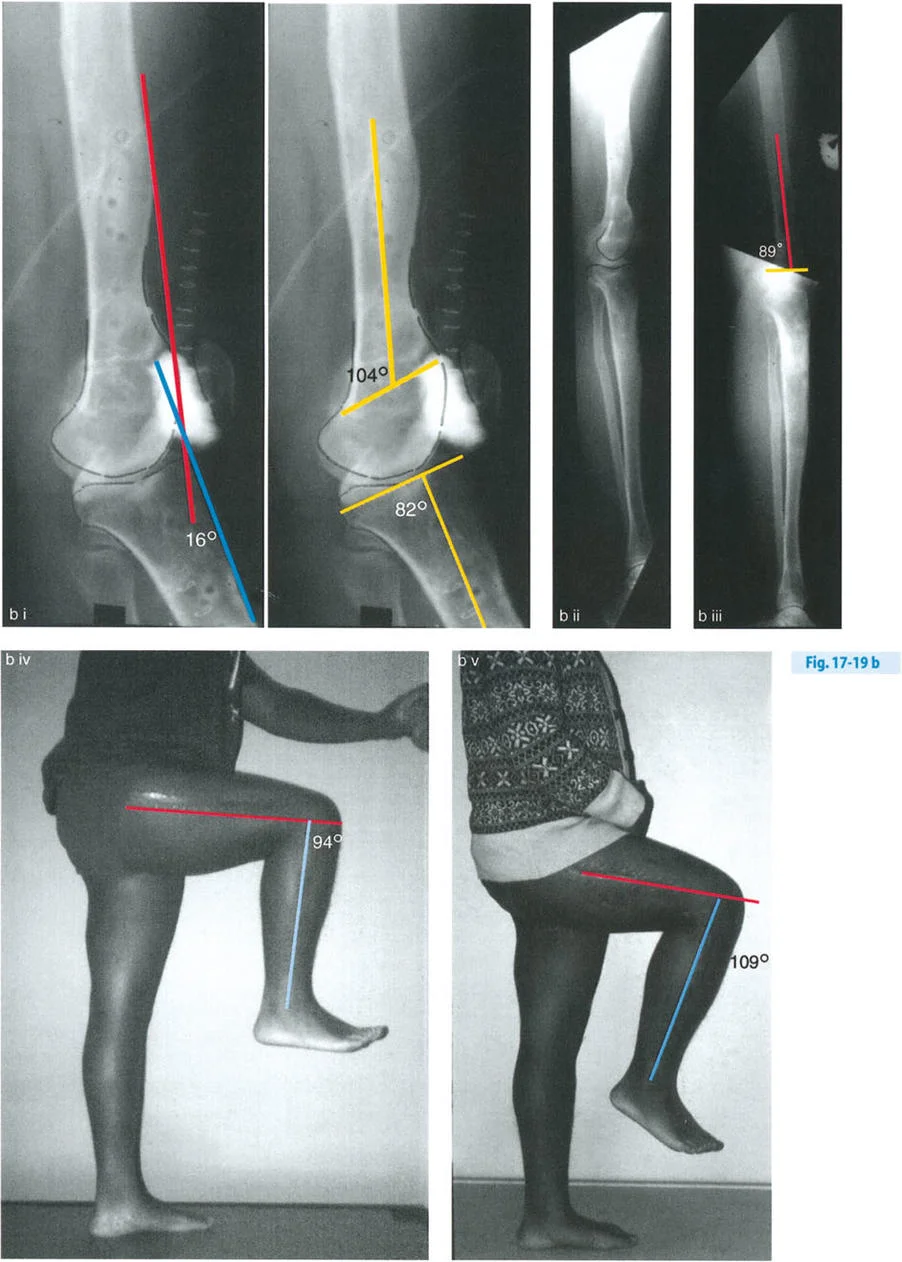
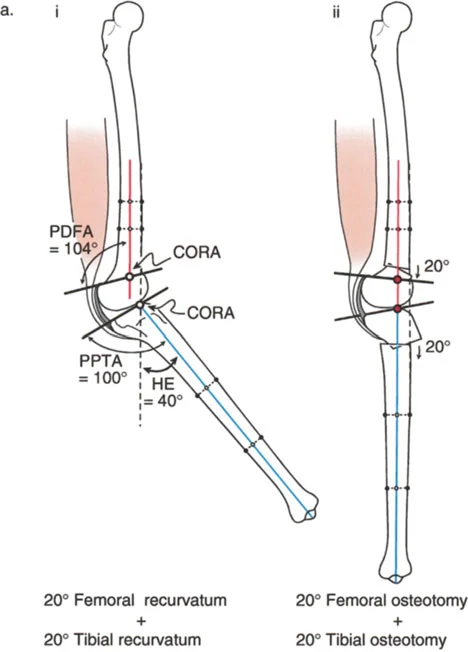
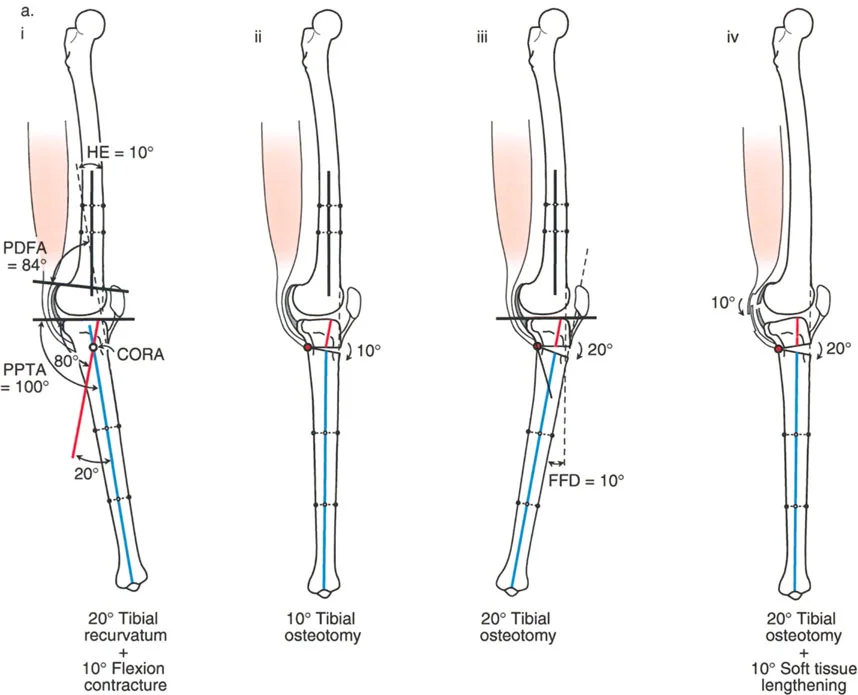
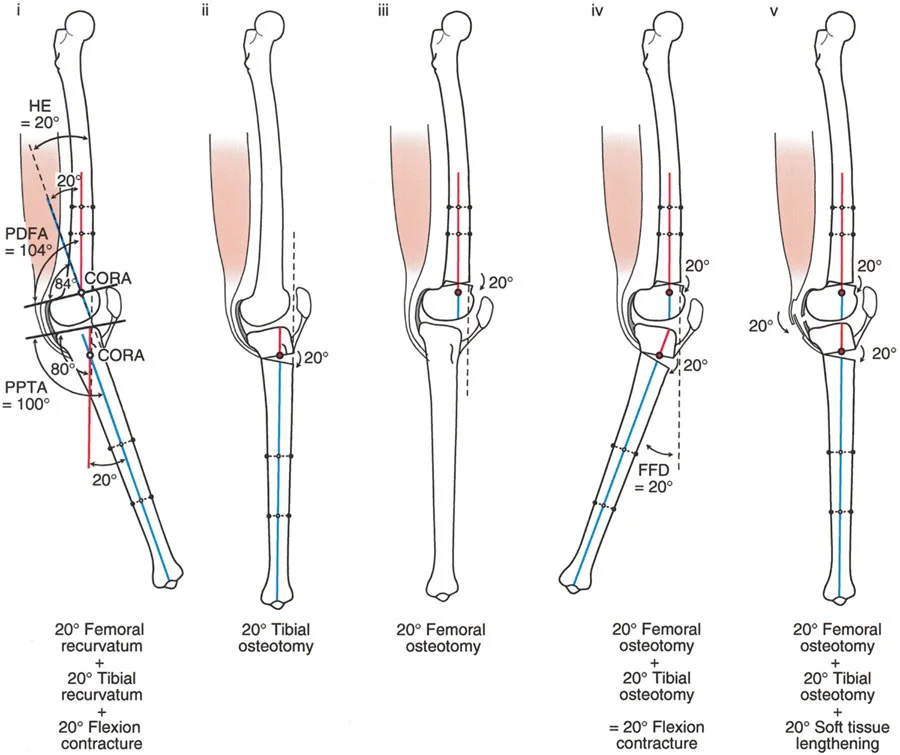
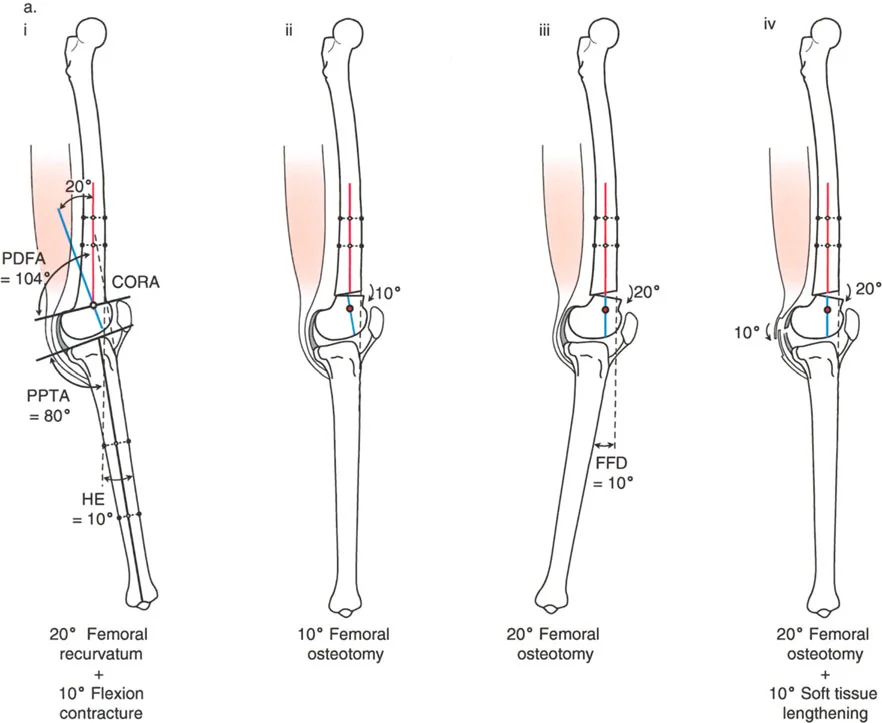
Pure Bony Femoral Recurvatum
In this scenario, the clinical hyperextension (HE) of the knee exactly matches the magnitude of the bony deformity in the femur.
Clinical Presentation
* Maximum knee extension position reveals 20 degrees of HE.
* Radiographic analysis shows a PDFA of 104 degrees (normal ~83 degrees) and a normal PPTA of 80 degrees.
* The CORA is located in the distal femur.
* The magnitude of the femoral recurvatum is exactly 20 degrees.
Because the femoral recurvatum deformity equals the knee HE deformity, the hyperextension is entirely due to the bone deformity of the femur. There is no soft tissue contracture.
Surgical Strategy
The ideal treatment is a distal femoral flexion osteotomy of 20 degrees with the correction axis placed around the CORA. After correction, the HE will be reduced to 0 degrees, restoring normal alignment and gait.
Alternative Treatment Pitfall Attempting to treat a distal femoral recurvatum with a proximal tibial flexion osteotomy is a severe error. While it may mathematically eliminate the clinical hyperextension, the tibia will appear anteriorly translated relative to the femur. This creates a "subluxed" appearance, drastically increases patellofemoral contact pressures, and leads to early arthritis.
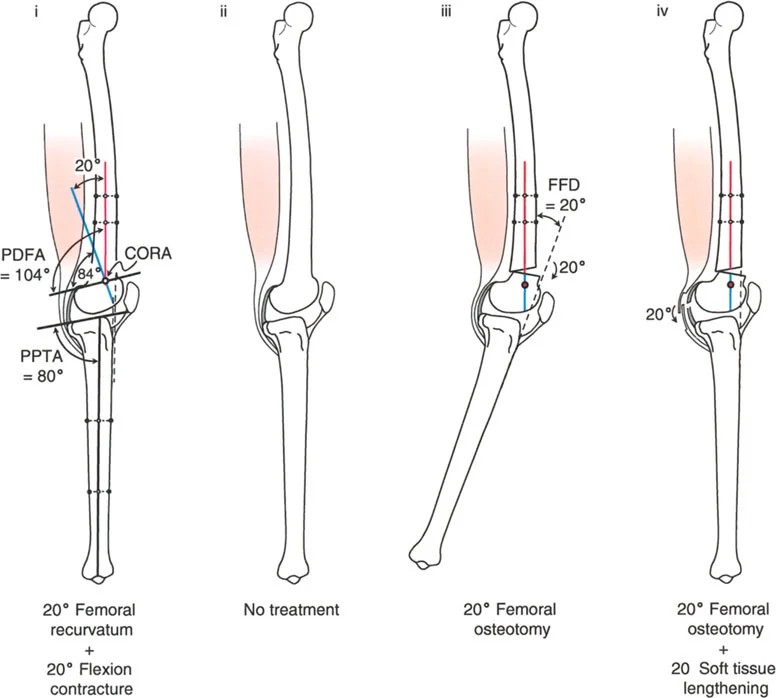
Femoral Recurvatum with Compensatory Flexion Contracture
The human body frequently compensates for bony deformities by adapting the surrounding soft tissues. A 20-degree femoral recurvatum can be entirely masked by a 20-degree soft tissue flexion contracture.
Clinical Presentation
* The knee comes into neutral full extension clinically (0 degrees HE).
* Radiographic analysis reveals a PDFA of 104 degrees (20 degrees of bony recurvatum) and a normal PPTA.
* Despite the 20-degree bony recurvatum, there is no clinical HE deformity.
Therefore, there must be a compensatory posterior soft tissue flexion contracture of exactly 20 degrees holding the knee out of hyperextension.
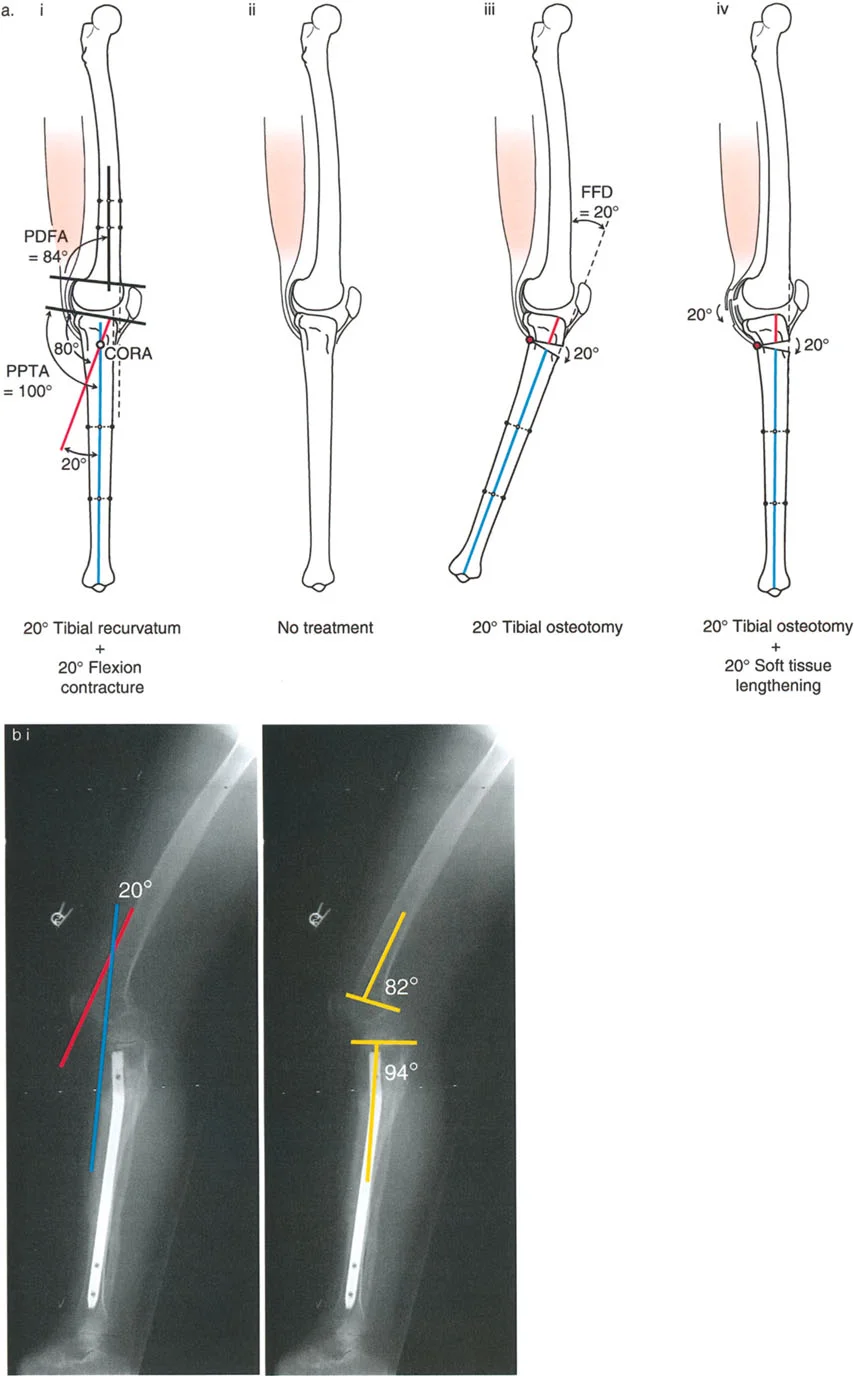
Surgical Strategy
The ideal treatment for this specific scenario is often no surgery. The knee achieves full clinical extension and is usually asymptomatic during the stance phase of gait. The only functional deficit is a 20-degree loss of terminal deep flexion due to the recurvatum deformity of the distal femur (the calf collides with the posterior thigh prematurely).
The Worst Possible Treatment Performing a 20-degree distal femoral flexion osteotomy based solely on the radiographs is a catastrophic error. Correcting the bone by 20 degrees will unmask the 20-degree soft tissue flexion contracture. The patient will wake up with a 20-degree Fixed Flexion Deformity (FFD), severely impairing their ability to walk. If an osteotomy is absolutely indicated (e.g., for severe joint pain or other complex multi-planar deformities), it must be accompanied by extensive soft tissue lengthening and posterior capsular release to achieve full extension.
Femoral Recurvatum with Partial Flexion Contracture
This is a hybrid scenario where the soft tissue contracture only partially compensates for the bony deformity.
Clinical Presentation
* Maximum knee extension position reveals 10 degrees of HE.
* Radiographic analysis shows a PDFA of 104 degrees (20 degrees of bony recurvatum).
* Because the clinical HE (10 degrees) is less than the bony deformity (20 degrees), there is an associated partial knee flexion contracture of 10 degrees.
Surgical Strategy
The ideal treatment is a compromise a distal femoral osteotomy of only 10 degrees with the correction axis around the CORA. By under-correcting the bone to match the soft tissue envelope, the postoperative FFD is 0 degrees, and the clinical HE is eliminated.
If the surgeon were to correct the full 20 degrees of bony deformity, a 10-degree FFD would result, which is highly detrimental to gait. Complete radiographic realignment (correcting the full 20 degrees) would mandate a simultaneous soft tissue release.
The Golden Rule of Sagittal Knee Deformity
The critical factor in managing sagittal plane knee deformities is to maintain full extension of the knee. A stable, fully extended knee is an absolute prerequisite for an energy-efficient stance phase during gait. Gaining terminal flexion is always secondary. A patient can function exceptionally well lacking 20 degrees of deep flexion, but a 10-degree Fixed Flexion Deformity will cause profound quadriceps fatigue, an antalgic gait, and eventual joint decompensation.
Summary of Femoral Recurvatum Treatment Strategies
| Clinical Hyperextension | Radiographic Deformity | Soft Tissue Contracture | Recommended Treatment Strategy |
|---|---|---|---|
| 20 Degrees | 20 Degrees | 0 Degrees | 20° Femoral Flexion Osteotomy |
| 0 Degrees | 20 Degrees | 20 Degrees | Observation OR Osteotomy + Soft Tissue Release |
| 10 Degrees | 20 Degrees | 10 Degrees | 10° Femoral Flexion Osteotomy (Under-correction) |

Step by Step Preoperative Planning Guide
Meticulous preoperative planning is the difference between a successful realignment and an iatrogenic disaster. Follow these steps when evaluating a sagittal plane knee deformity.
- Clinical Assessment of Range of Motion
- Measure maximum extension with the patient supine. Elevate the heel and allow the knee to fall into maximum hyperextension. Document this value.
- Assess for any Fixed Flexion Deformity (FFD).
- Evaluate patellar tracking and the presence of patella alta or baja.
- Acquire Standardized Radiographs
- Obtain standing, full-length, lateral radiographs of the lower extremity. The knee must be in its maximum extended position during the radiograph to accurately capture the dynamic deformity.
- Determine Joint Orientation Angles
- Draw the mid-diaphyseal line of the femur and the tibia.
- Draw the joint orientation lines for the distal femur and proximal tibia.
- Calculate the PDFA and PPTA. Compare these to normal values (PDFA ~83°, PPTA ~81°).
- Locate the CORA
- Identify where the abnormal mechanical/anatomical axis intersects the normal mechanical/anatomical axis. This is the CORA.
- Calculate the Soft Tissue Component
- Subtract the clinical hyperextension from the radiographic bony deformity. The difference is the magnitude of the soft tissue flexion contracture.
- Plan the Osteotomy Level and Type
- For the tibia, assess the patellar tendon insertion to decide between a supra-tuberosity or infra-tuberosity osteotomy.
- For the femur, decide whether to perform a full correction, a partial correction (compromise), or a full correction with soft tissue lengthening.
- Select Fixation Hardware
- Determine if the correction will be acute (using plates/screws or intramedullary nails) or gradual (using circular external fixation).
Surgical Execution and Fixation Strategies
Once the plan is established, the execution relies on precise surgical technique. The choice of fixation depends on the magnitude of the deformity, the quality of the bone, and the need for simultaneous lengthening.
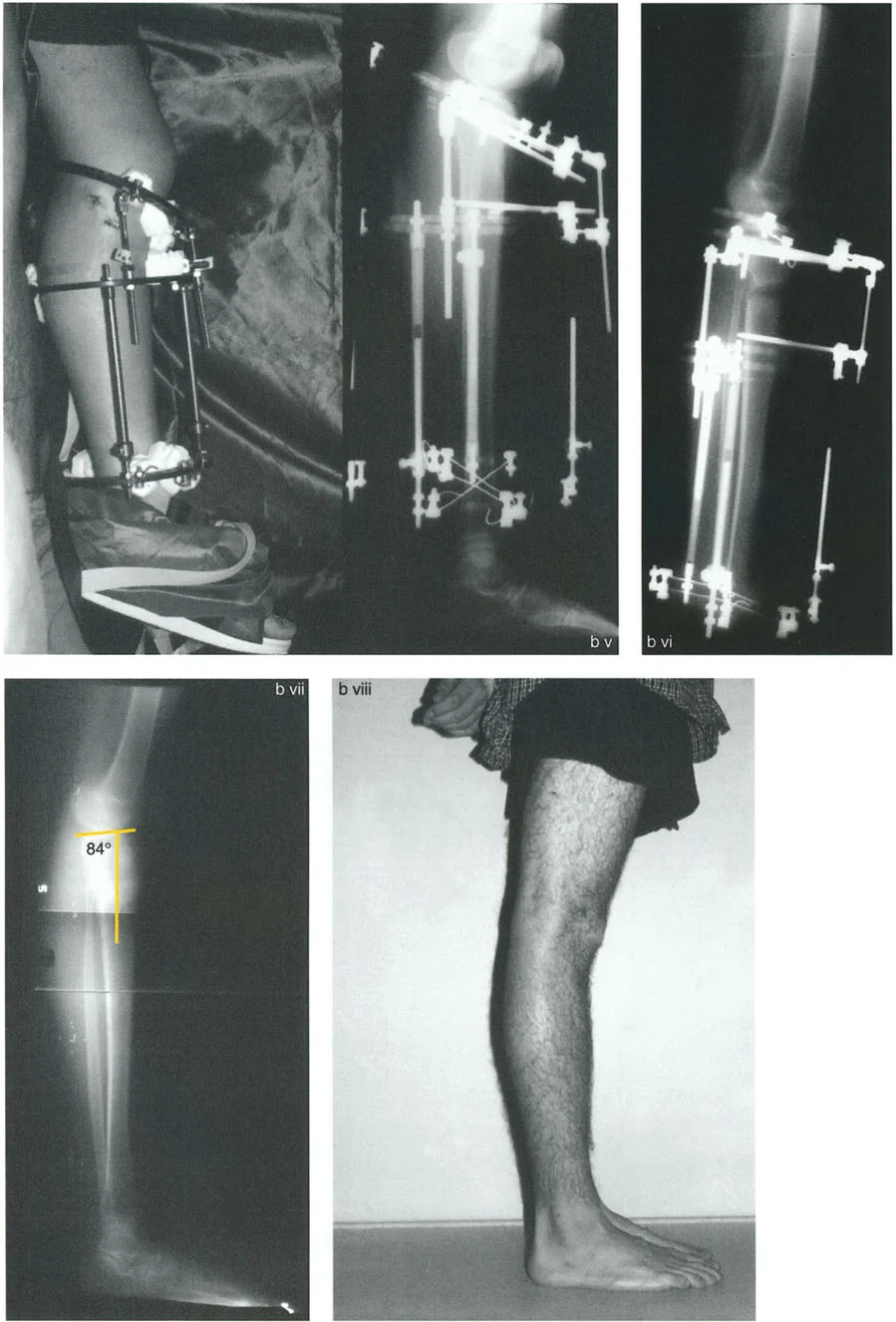
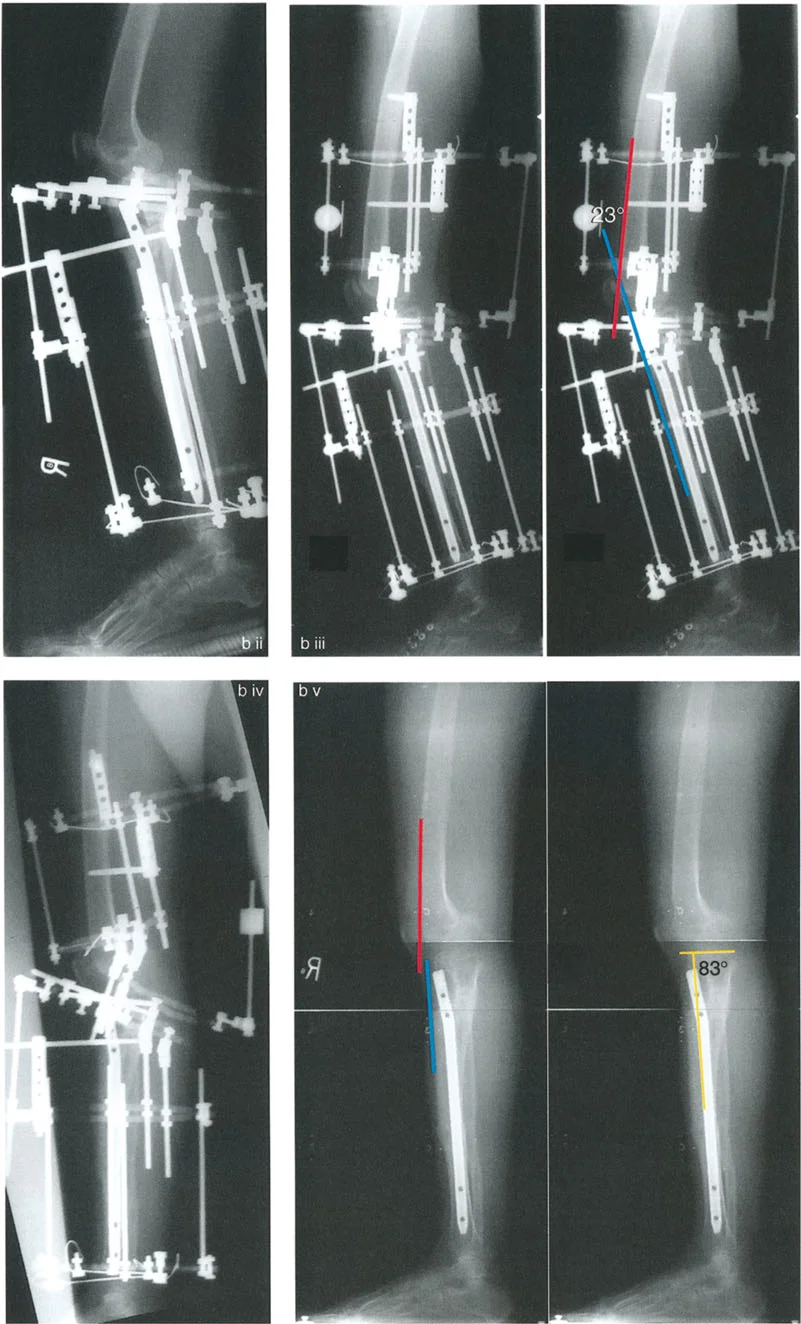
Lengthening Over Nail (LON)
For symptomatic recurvatum deformities of the femur (such as those seen in post-polio patients), Lengthening Over Nail (LON) is an excellent strategy. A flexion osteotomy is performed, and the bend of the intramedullary nail is utilized to flex the distal femur.
During LON, an external fixator is applied temporarily to control the bone segments during the gradual lengthening and deformity correction phase. Once the desired correction and length are achieved, the intramedullary nail is locked distally, and the external fixator is removed. This technique minimizes the time the patient spends in an external fixator while providing robust stabilization of the sagittal plane correction.
Circular External Fixation
For complex, multi-planar deformities involving both recurvatum and coronal plane malalignment (valgus/varus), circular external fixation (such as the Taylor Spatial Frame or Ilizarov apparatus) remains the gold standard.
External fixation allows for gradual correction, which is particularly beneficial when massive soft tissue adaptations are present. Gradual correction stretches the posterior neurovascular structures safely, reducing the risk of sciatic or peroneal nerve palsy that can occur with acute massive corrections. Furthermore, it allows the surgeon to fine-tune the sagittal plane alignment postoperatively based on standing radiographs.
Acute Correction with Internal Fixation
For isolated, moderate sagittal plane deformities without the need for lengthening, acute correction with rigid internal fixation (locking plates) is highly effective.
When performing an acute opening wedge flexion osteotomy of the distal femur, bone grafting (autograft or allograft) is typically required to fill the void and promote union. The surgeon must meticulously protect the posterior structures (popliteal artery and vein) during the osteotomy, as the posterior cortex is breached and the gap is opened posteriorly.
Surgical Pearls and Pitfalls
- Pearl Always measure clinical hyperextension with the patient awake and relaxed. Muscle guarding can mask the true extent of the recurvatum.
- Pitfall Failing to account for a soft tissue flexion contracture when planning a femoral osteotomy. Correcting the bone without addressing the soft tissue will leave the patient with a devastating Fixed Flexion Deformity.
- Pearl In proximal tibial osteotomies, if the patellar tendon insertion is normal, stay distal to the tuberosity to avoid creating patella baja.
- Pitfall Treating a distal femoral recurvatum with a proximal tibial osteotomy. This creates a severe translational mismatch at the joint line, leading to subluxation and rapid joint degeneration.
- Pearl Maintaining full knee extension is infinitely more important for functional gait than restoring the last 15 to 20 degrees of deep knee flexion. Never sacrifice full extension for flexion.
- Pearl Utilizing fibular transport distally during a proximal tibial osteotomy is an elegant way to use the LCL to indirectly reduce a posteriorly subluxed tibia.
Conclusion
Mastering sagittal plane knee considerations requires a paradigm shift from simple two-dimensional thinking to a comprehensive understanding of bone and soft tissue kinematics. By applying Dr. Paley's principles of CORA, meticulously evaluating the joint orientation angles (PDFA and PPTA), and respecting the profound impact of compensatory soft tissue contractures, orthopedic surgeons can execute precise, life-altering deformity corrections. Whether utilizing internal plates, intramedullary nails, or circular external fixators, the ultimate goal remains constant: restore the mechanical axis, optimize the extensor mechanism, and, above all, preserve full knee extension for a functional, energy-efficient gait.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like

