Paley's Principles: Advanced Deformity Correction for Lower Extremity Malalignment
Key Takeaway
Paley's Principles offer a systematic, mathematical approach to lower extremity deformity correction. They analyze mechanical axis deviation, joint orientation angles (mLDFA, MPTA), and the CORA to precisely plan osteotomies, restore alignment, and prevent progressive arthrosis.
Biological and Mechanical Foundations of Lower Extremity Aging
All living organisms are limited to a finite life span, and the human musculoskeletal system is no exception. As with any complex mechanical system, the cumulative, debilitating effects of time, wear, and gravity result in an almost imperceptible, gradual degradation in performance. While tissues like skin and bone possess an astonishing capacity for healing and regeneration—serving as the very foundation of modern reconstructive orthopedics and osteogenesis—articular cartilage represents a profoundly different biological reality.
The Chondrocyte and Extracellular Matrix Under Stress
Although articular cartilage is subjected to some of the highest mechanical demands in the human body, its capacity for repair and regeneration is notoriously limited due to its avascular, aneural, and alymphatic nature. Chondrocytes, the resident cells of cartilage, are locked within a dense extracellular matrix of Type II collagen and proteoglycans, severely restricting their ability to mount a reparative response to microtrauma. Consequently, articular cartilage is often among the first tissues to manifest the clinical effects of aging.
Remarkably, this relatively fragile tissue is responsible for transmitting loads exceeding several times our body weight for an estimated one billion cycles during the course of an average lifetime.
It is not surprising, therefore, that any disturbance of the normal anatomic and biomechanical relationships in the lower limb can result in an aggressive acceleration of this gradual degradation. Because the lower extremities are normally weight-bearing throughout our lives, the axial alignment of the lower extremities is the single most critical factor in determining the mechanical demands to which articular cartilage is repeatedly exposed during the dynamic phases of human gait.
Pathogenesis of Arthrosis Mechanical Overload Versus Inflammation
At present, there is a broad, evidence-based consensus within the orthopedic community that the primary cause of degenerative arthropathy is mechanical, not inflammatory.
While commonly referred to in layman's terms as degenerative arthritis, this terminology is technically and pathologically inaccurate. Inflammation in the osteoarthritic joint is a secondary cascade—a biochemical result of cartilage breakdown products irritating the synovium, not the principal instigating cause. Therefore, arthrosis is the preferred terminology for describing the purely degenerative, mechanically driven pathological abnormalities of the joint.
Unicompartmental knee arthrosis affecting either the medial or lateral compartment in isolation is frequently associated with malalignment resulting from congenital anomalies, developmental conditions like Blounts disease, or post-traumatic deformity such as malunited fractures. While the association between malalignment and arthrosis is universally acknowledged, the exact pathogenic relationship requires a deep understanding of joint biomechanics.
For decades, researchers debated a fundamental chicken-or-egg scenario. Does arthrosis represent the response of abnormal cartilage to normal physiological forces, or does it reflect the response of normal cartilage to excessive biomechanical stress?
Substantial evidence from the orthopedic literature supports the latter hypothesis. Malalignment alters stress distribution across the joints of the lower extremity, creating eccentric focal overloading that destroys normal cartilage.
When the mechanical axis shifts, the ground reaction force vector moves away from the center of the joint. This concentrates massive compressive forces onto a much smaller surface area of cartilage. The chondrocytes, unable to withstand this focal overloading, undergo apoptosis. The extracellular matrix breaks down, leading to fibrillation, fissuring, and eventual full-thickness cartilage loss down to the subchondral bone.
Biomechanics of the Load Bearing Axis
Central to understanding lower limb deformity is the concept of the weight-bearing axis, universally termed the mechanical axis.
Historical Contributions of Pauwels and Maquet
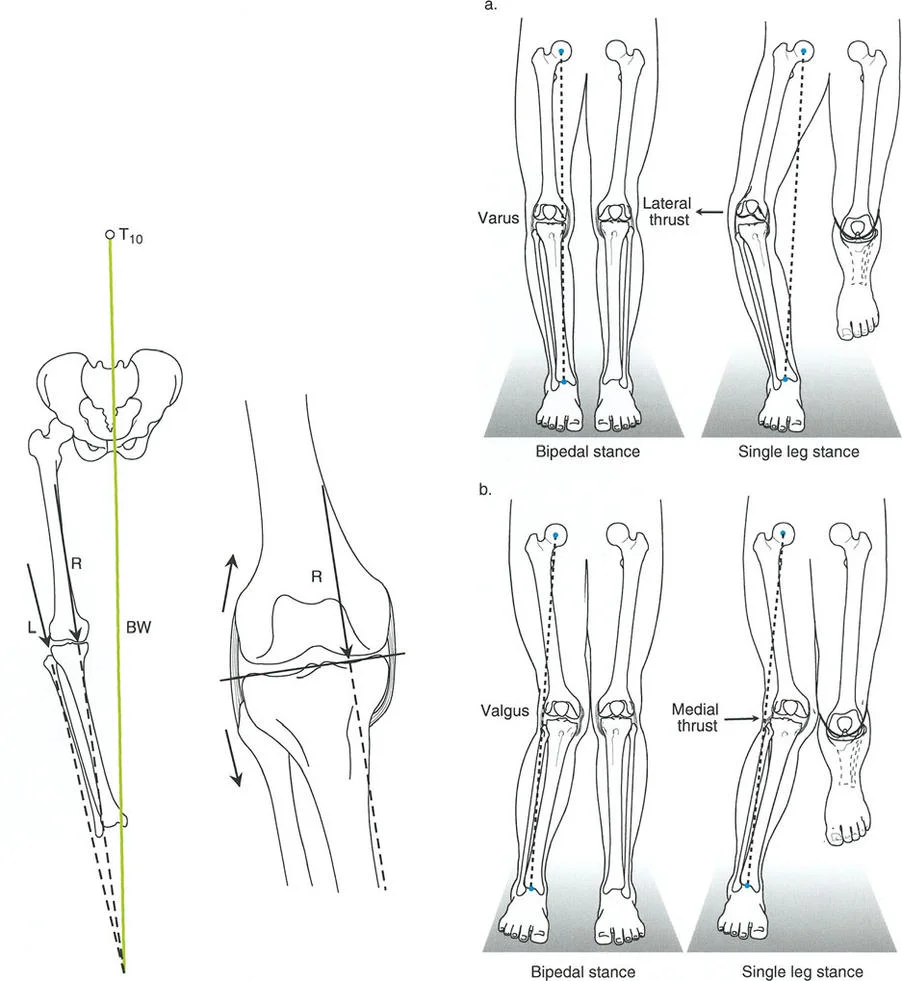
Pioneered by the visionary biomechanist Friedrich Pauwels in the 1980s, the mechanical axis of the lower extremity is depicted as a straight line passing from the center of the ankle to the center of the hip. This line represents the path of transmission of the load-bearing force relative to the lower extremity during a static, two-legged stance.
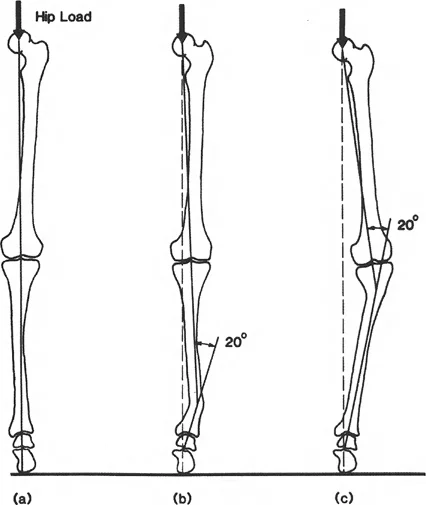
Any deformity in the coronal plane that alters the alignment of the joints of the lower extremity disturbs this load-bearing axis. When the load-bearing axis passes medial or lateral to the center of the knee, it creates a moment arm. This moment arm acts as a lever, exponentially increasing the force transmitted across either the medial or lateral tibiofemoral compartment.
Pauwels was one of the first surgeons to recognize the profound importance of biomechanics and its direct relationship to surgical planning for deformity correction via osteotomy. He recognized that realignment was not just a cosmetic endeavor, but an absolute biological necessity to restore normal force transmission across the knee and provide a mechanical environment where cartilage could survive.
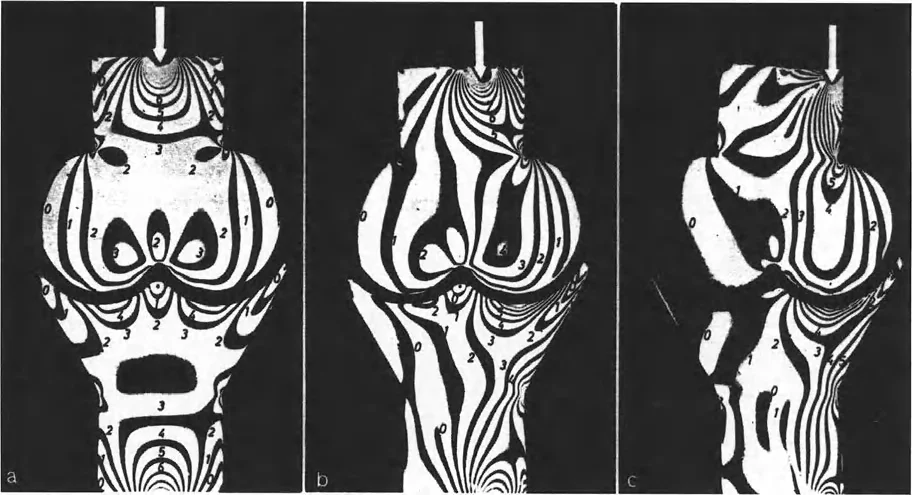
Paul Maquet later expanded on Pauwels groundbreaking ideas. He elegantly demonstrated the alteration in stress transmitted across simulated joints using polarized light and photoelastic models.
These landmark photoelastic studies visually verified what mathematicians had calculated. Restoring or correcting the mechanical axis is the only definitive way to alter load transmission across the knee, thereby halting or slowing the progression of unicompartmental arthrosis.
Paley Principles of Deformity Correction
Dr. Dror Paley revolutionized orthopedic surgery by transforming deformity correction from an intuitive art into a highly reproducible, mathematically precise science. The Paley Principles provide a universal language and a systematic algorithm for analyzing and correcting any lower extremity deformity, regardless of its complexity. To master deformity correction, the orthopedic surgeon must become intimately familiar with the following core concepts.
Mechanical Axis Deviation MAD
The Mechanical Axis Deviation is the foundational metric of lower extremity alignment. On a standing 51-inch anteroposterior radiograph, the mechanical axis of the lower extremity is a line drawn from the center of the femoral head to the center of the tibial plafond.
In a normally aligned limb, this line passes slightly medial to the exact center of the knee joint, typically 8 to 10 millimeters medial to the midpoint of the tibial plateau.
When the mechanical axis line deviates further medially, the patient has a varus deformity, and the MAD is measured in millimeters medial to the center of the knee. When the line deviates laterally, the patient has a valgus deformity, and the MAD is measured in millimeters lateral to the center. Quantifying the MAD is the first step in determining whether a clinically significant deformity exists that warrants surgical intervention.
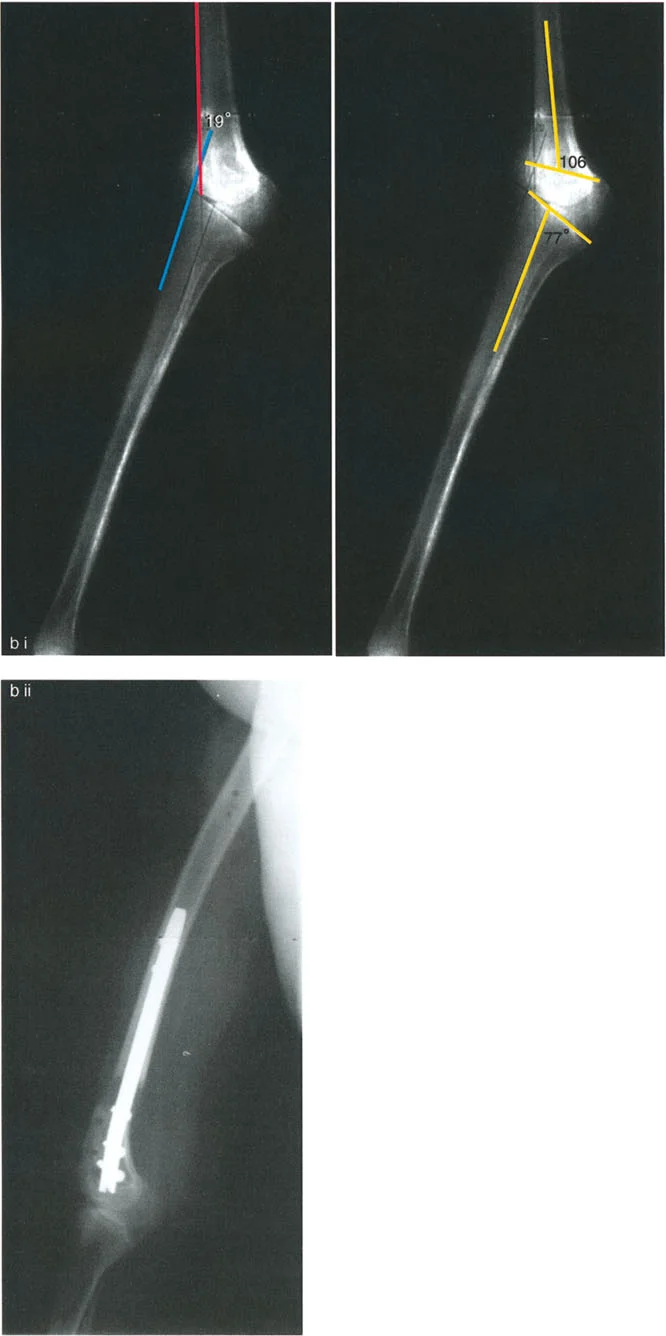
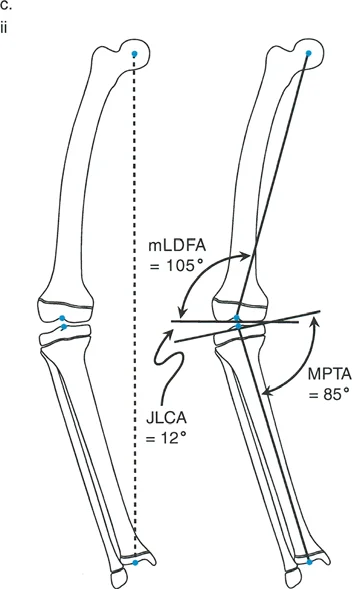
Joint Orientation Angles mLDFA MPTA and JLCA
To determine exactly where the deformity originates—whether in the femur, the tibia, or within the joint itself—the surgeon must measure the joint orientation angles. These angles define the relationship between the mechanical axis of a bone and its articular surface.
Paley established standard normative values for these angles, which are essential for preoperative templating.
| Angle Abbreviation | Full Name | Normal Value Range | Clinical Significance |
|---|---|---|---|
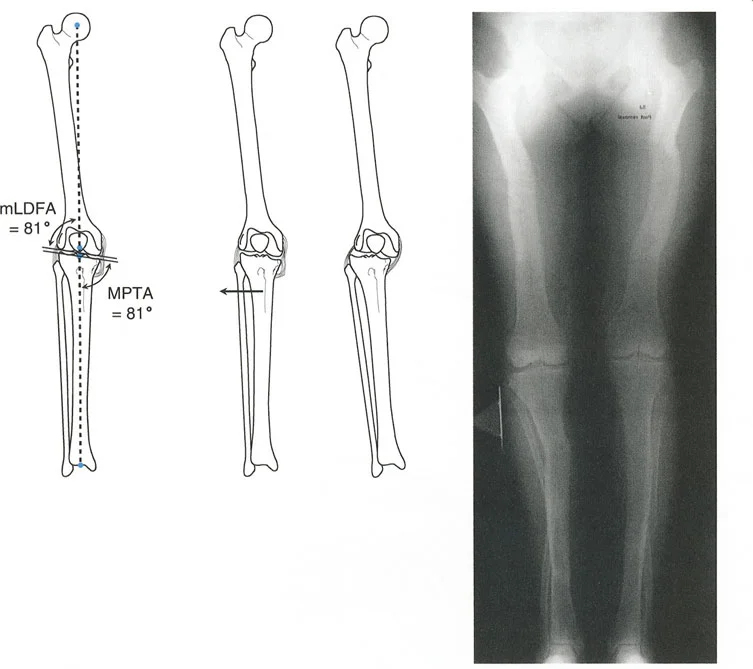
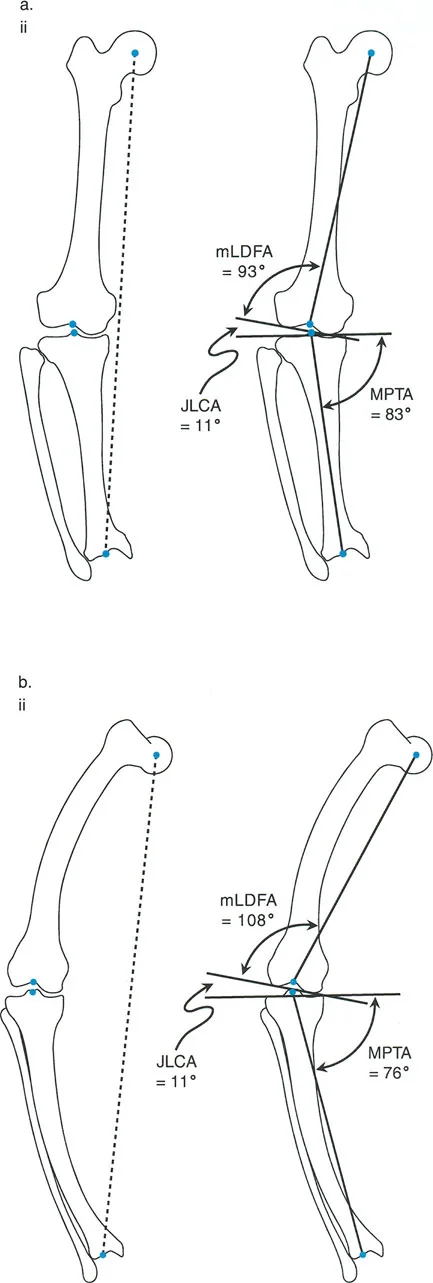
| mLDFA | Mechanical Lateral Distal Femoral Angle | 85 to 90 degrees (Avg 87) | Determines distal femoral coronal alignment. Abnormal values indicate femoral varus or valgus. |
| MPTA | Medial Proximal Tibial Angle | 85 to 90 degrees (Avg 87) | Determines proximal tibial coronal alignment. Abnormal values indicate tibial varus or valgus. |
| LDTA | Lateral Distal Tibial Angle | 87 to 91 degrees (Avg 89) | Determines ankle joint orientation. Crucial for supramalleolar osteotomies. |
| JLCA | Joint Line Convergence Angle | 0 to 2 degrees | Measures the convergence of the distal femoral and proximal tibial articular surfaces. High values indicate intra-articular deformity or ligamentous laxity. |
Understanding the JLCA is particularly critical. If a patient presents with a severe varus deformity, but the mLDFA and MPTA are entirely normal, the deformity is not osseous. Instead, an abnormally high JLCA indicates that the deformity is driven by lateral ligamentous laxity or profound medial cartilage loss. Osteotomizing a bone to correct a purely ligamentous deformity violates Paley's principles and leads to joint line obliquity.
Center of Rotation of Angulation CORA
The Center of Rotation of Angulation is the cornerstone of Paley's preoperative planning method. The CORA represents the exact point where the proximal mechanical axis line and the distal mechanical axis line of a deformed bone intersect.
Defining the CORA and the Bisector Line
To find the CORA, the surgeon draws the mechanical axis of the proximal segment of the deformed bone and the mechanical axis of the distal segment. The point at which these two lines cross is the CORA.
Once the CORA is established, the surgeon must draw the bisector line. The bisector line perfectly divides the angle formed by the intersection of the proximal and distal axes.
The transverse bisector line is critical because it dictates the transverse plane of the osteotomy. If an osteotomy is performed along this bisector line, the bone ends will perfectly match up without creating unwanted step-offs or secondary deformities.
Paley Osteotomy Rules
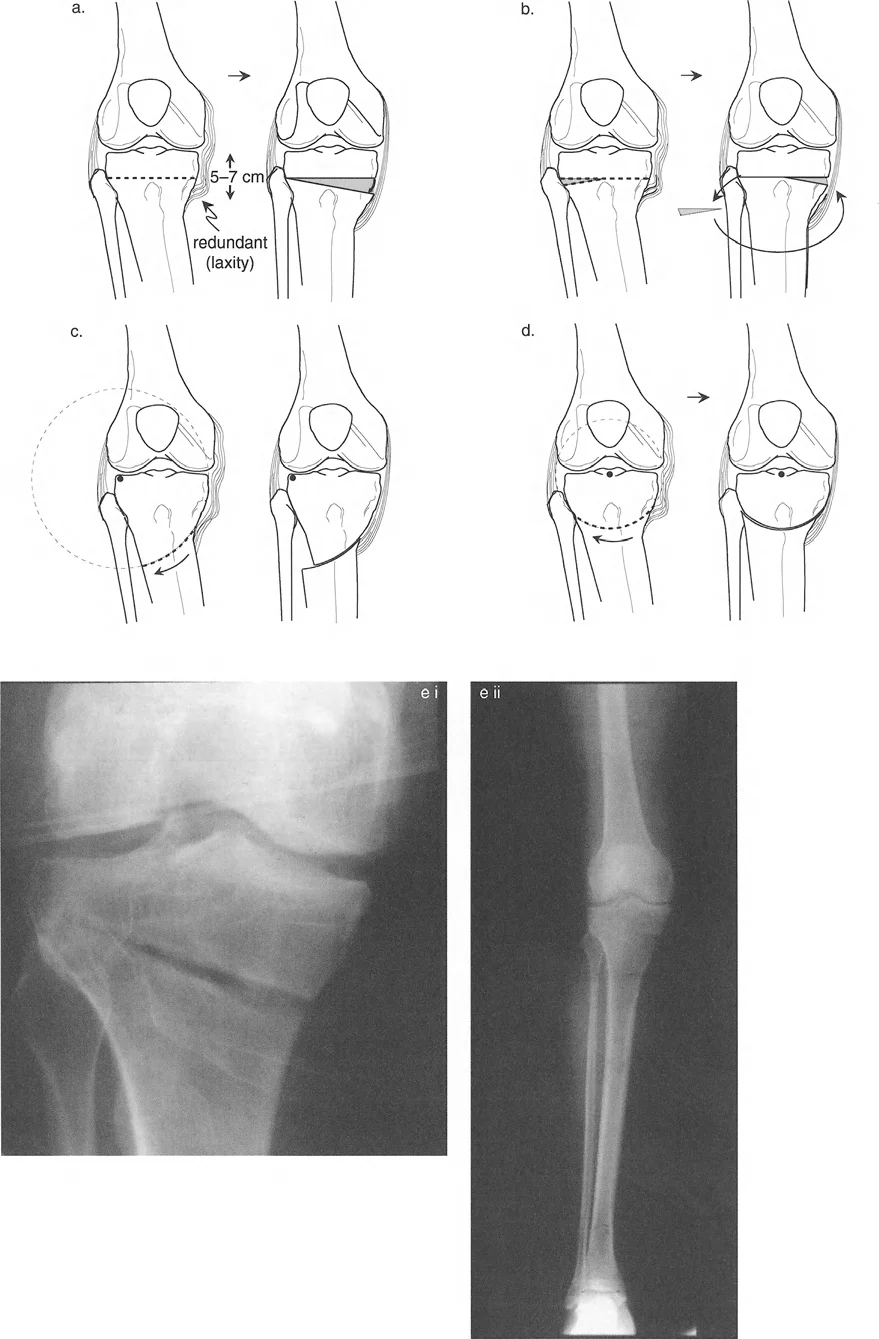
Identifying the CORA is only half the battle. The surgeon must then decide where to make the bone cut (the osteotomy) and where to place the hinge (the Axis of Correction of Angulation, or ACA). Paley codified three fundamental osteotomy rules that dictate the biomechanical outcome of a correction.
Osteotomy Rule One Pure Angulation
Rule One: When the osteotomy and the ACA (hinge) both pass through the CORA, pure angulation occurs without any translation.
This is the most biomechanically sound and biologically favorable method of correction. Because the bone ends pivot directly around the apex of the deformity, the mechanical axis is perfectly restored, and the bone ends remain in excellent cortical contact, promoting rapid osteogenesis and healing.
Osteotomy Rule Two Angulation and Translation
Rule Two: When the ACA (hinge) passes through the CORA, but the osteotomy is performed at a different level, the correction will result in both angulation and translation of the bone ends.
Clinically, this rule is utilized when the CORA is located very close to a joint line, making a Rule One osteotomy impossible due to the lack of adequate bone stock for fixation. By making the osteotomy further down the diaphysis but keeping the hinge at the CORA, the mechanical axis is still perfectly restored. However, the surgeon must anticipate and allow for the resulting translation at the osteotomy site. Attempting to force the translated bone ends back together will result in a failure to correct the mechanical axis.
Osteotomy Rule Three Iatrogenic Translation
Rule Three: When the osteotomy and the ACA (hinge) are both placed outside the CORA, the result is a massive iatrogenic translation and a failure to correct the mechanical axis.
This rule defines what happens when deformity correction is planned poorly. If a surgeon simply cuts the bone at a convenient location and bends it without respecting the CORA, a secondary translation deformity is created. The mechanical axis will remain deviated, and the joint will continue to experience eccentric focal overloading. Rule Three is a warning of what to avoid in clinical practice.
Step by Step Preoperative Planning
Successful deformity correction requires meticulous preoperative templating. Paley's method relies on two standardized tests performed on long-leg standing radiographs.
The Malalignment Test
The Malalignment Test is the initial screening tool to determine if the mechanical axis is deviated.

- Draw a line from the center of the femoral head to the center of the ankle joint.
- Observe where this line passes through the knee joint.
- Measure the Mechanical Axis Deviation in millimeters from the center of the tibial plateau.
- If the MAD is greater than 10 millimeters medial or lateral, a clinically significant malalignment exists, prompting the next step.
The Malorientation Test
If the Malalignment Test is positive, the Malorientation Test is performed to isolate the source of the deformity.
- Draw the mechanical axis of the femur (center of femoral head to center of femoral notch).
- Measure the mLDFA. If it falls outside the normal 87-degree range, a femoral deformity is present.
- Draw the mechanical axis of the tibia (center of tibial spines to center of tibial plafond).
- Measure the MPTA. If it falls outside the normal 87-degree range, a tibial deformity is present.
- Measure the JLCA. If it is greater than 2 degrees, an intra-articular or ligamentous component is contributing to the deformity.
Executing the Preoperative Templating
Once the deformed bone is identified, the surgeon locates the CORA and applies the Osteotomy Rules to plan the surgical cut.
The surgeon must draw the anticipated correction on the digital radiograph, ensuring that the postoperative mechanical axis will pass through the center of the knee joint. This templating dictates the exact wedge size for an opening or closing wedge osteotomy, or the exact strut adjustments required for a hexapod external fixator.
Multi Apical Deformities and Sagittal Plane Considerations
Not all deformities are simple, single-apex angulations in the coronal plane. Many patients present with complex, multi-apical deformities that require advanced planning.
When a bone has sustained multiple fractures or has a developmental bowing condition, there may be more than one CORA.
In these instances, the surgeon must perform a segmental analysis, drawing mechanical axis lines for the proximal, middle, and distal segments of the bone. Correcting a multi-apical deformity with a single osteotomy will invariably violate Paley's rules, resulting in a residual translational deformity. Therefore, multi-apical deformities generally require multi-level osteotomies.
Furthermore, deformity correction is a three-dimensional endeavor. While coronal plane alignment is critical for mediolateral load distribution, sagittal plane alignment is equally important for gait mechanics and joint stability.
Sagittal plane deformities, such as procurvatum (anterior bowing) or recurvatum (posterior bowing), alter the tension on the cruciate ligaments and change the patellofemoral tracking dynamics. The surgeon must measure the Posterior Distal Femoral Angle (PDFA) and the Posterior Proximal Tibial Angle (PPTA) on a lateral radiograph to ensure that the sagittal mechanical axis is restored alongside the coronal axis.
Surgical Execution and Fixation Strategies
Once the preoperative plan is finalized, the surgeon must select the appropriate fixation construct. The choice of fixation depends on the location of the CORA, the quality of the soft tissue envelope, and the magnitude of the correction required.
Internal Fixation Plates and Intramedullary Nails
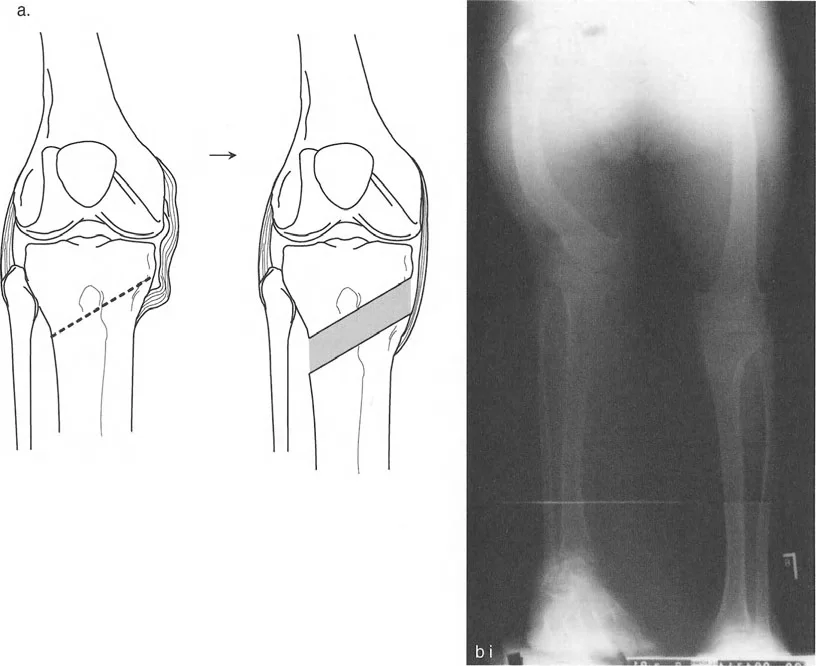
For acute corrections of single-apex deformities, internal fixation is often preferred due to patient comfort and rapid rehabilitation.
Opening wedge or closing wedge osteotomies can be rigidly stabilized with modern locking plate technology. When the CORA is diaphyseal, an intramedullary nail is an excellent biomechanical option. However, correcting a deformity with a straight nail in a curved tube presents unique challenges. The surgeon must frequently employ blocking screws, also known as Poller screws, to intentionally narrow the medullary canal and force the nail to follow the corrected mechanical axis, preventing the bone from sliding back into deformity.
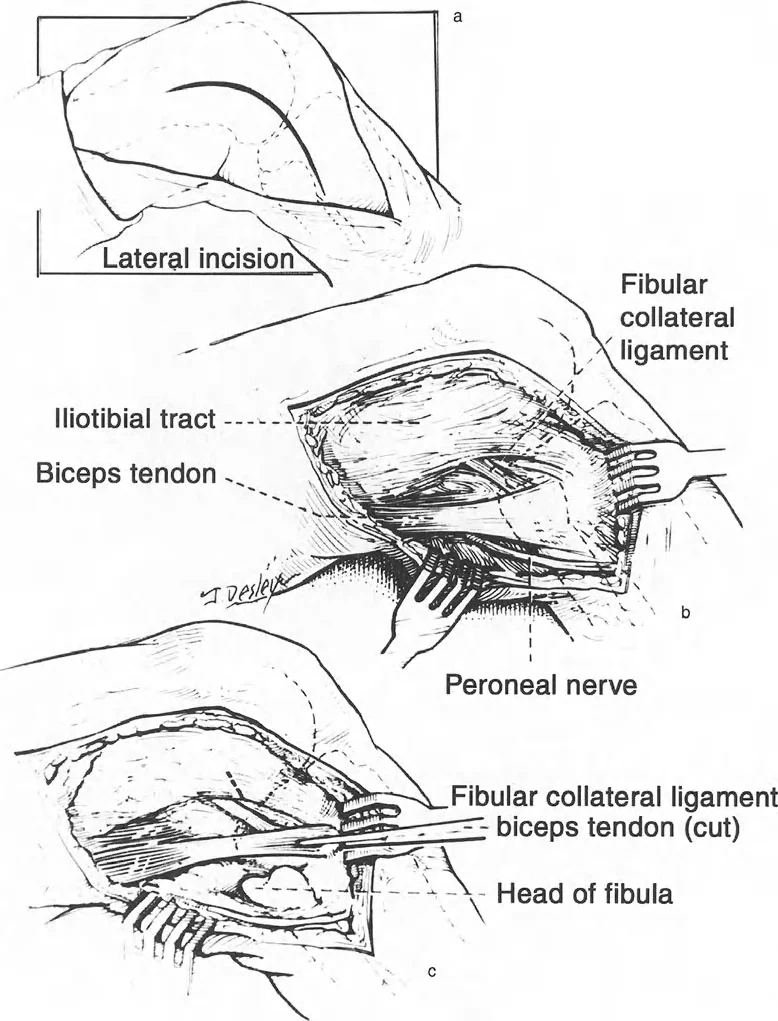
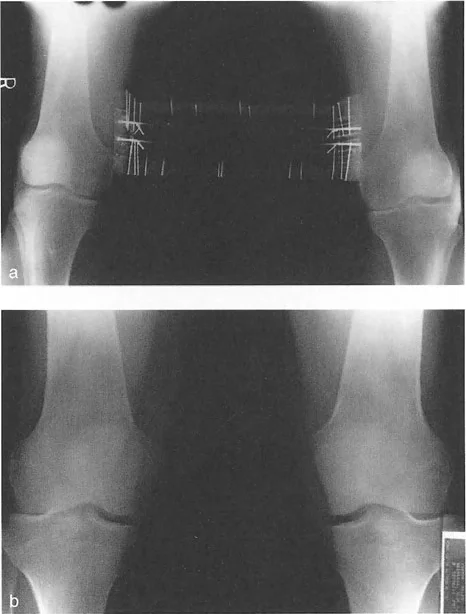
Circular External Fixation and Hexapod Systems
For complex, multi-planar deformities, multi-apical deformities, or deformities associated with significant limb length discrepancy, circular external fixation remains the gold standard.
Modern hexapod systems, such as the Taylor Spatial Frame, utilize the principles of a Stewart platform. By inputting the exact radiographic parameters, the CORA location, and the mounting parameters into a software program, the computer generates a daily schedule of strut adjustments. This allows for the gradual, simultaneous correction of angulation, translation, rotation, and length. Gradual correction also protects neurovascular structures, which can be stretched and damaged during large acute corrections.
Clinical Pearls for the Orthopedic Surgeon
To achieve mastery in deformity correction, the orthopedic surgeon should internalize these high-yield clinical pearls.
- Always Assess the JLCA First: Before planning an osteotomy, ensure the deformity is osseous. A high JLCA suggests ligamentous laxity or cartilage loss. An intra-articular problem cannot be solved with an extra-art
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like