Surgical Mastery of Angulation-Translation Deformities: Paley Principles
Key Takeaway
Angulation-translation deformities combine angular and parallel bone displacement, severely altering limb biomechanics. Surgical correction, guided by Paley's principles, is essential. It requires identifying the Center of Rotation of Angulation (CORA) and applying osteotomy rules to restore the mechanical axis and functional integrity of the limb.
Pathoepidemiology of Complex Lower Extremity Deformities
The management of complex lower extremity deformities involving a combination of translation and angulation represents one of the most intellectually and technically demanding challenges in orthopedic surgery. Translation and angulation translation deformities rarely occur in isolation. They are typically the sequelae of high energy trauma, segmental bone loss, or the failure of initial fracture fixation constructs. When a fracture heals with both angular and translational malalignment, the mechanical axis of the limb is profoundly altered, leading to a cascade of biomechanical derangements that extend far beyond the localized bony deformity.
Understanding the precise pathoepidemiology of these deformities is the fundamental first step toward executing a successful surgical correction and restoring both the mechanical integrity and the functional capacity of the affected limb.
Pathophysiologically, translation deformities occur when the anatomical axis of the proximal bone segment is displaced parallel to the anatomical axis of the distal segment. When this translation is coupled with angulation, often in orthogonal or oblique planes, the spatial geometry of the bone is severely distorted. The energy imparted during the initial trauma dictates the degree of soft tissue stripping, periosteal damage, and subsequent bone healing capacity. High energy diaphyseal fractures of the tibia and femur are particularly susceptible to these complex malunions due to the robust and asymmetric pull of the surrounding musculature, which exacerbates initial displacements if not rigidly neutralized by internal or external fixation.
Epidemiologically, the incidence of angulation translation deformities is highest among patients who have sustained open segmental fractures, those treated with non operative modalities that subsequently failed, or those who experienced premature weight bearing leading to hardware failure. The tibia is the most frequently involved long bone, largely due to its subcutaneous anteromedial border and relatively tenuous precarious blood supply. This anatomic vulnerability predisposes the tibia to delayed union, nonunion, and asymmetric cortical consolidation. Femoral deformities, while less common, present significant challenges due to the massive soft tissue envelope and the powerful deforming forces of the adductor and abductor muscle groups.
Soft Tissue Considerations in Translation Deformities
The soft tissue implications of angulation translation deformities cannot be overstated and must be a primary consideration during preoperative planning. The localized prominence of the malunited bone, often referred to clinically as the bump, can cause severe subcutaneous irritation, recurrent skin breakdown, and chronic pain, particularly in the lower leg.
This bump is not merely a cosmetic issue. It represents a focal area of high soft tissue tension that complicates surgical approaches and wound closure. In the setting of a nonunion with combined angulation and translation, the pathoanatomy is further complicated by the presence of atrophic or hypertrophic fibrous tissue, altered local vascularity, and the potential for subclinical osteomyelitis. The orthopedic surgeon must approach these deformities with a comprehensive understanding of both the osseous geometry and the surrounding soft tissue envelope to ensure a durable and biologically sound reconstruction. Failure to respect the soft tissue envelope inevitably leads to wound dehiscence, deep infection, and failure of the reconstructive effort.
Biomechanics and Surgical Anatomy
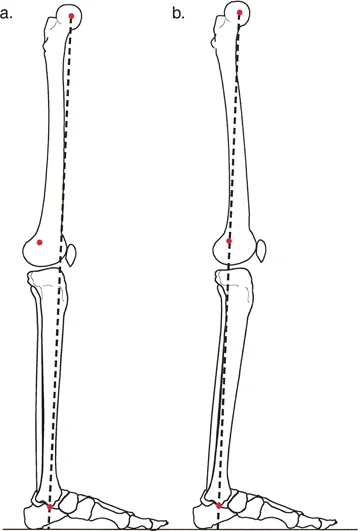
A rigorous mastery of surgical anatomy and lower extremity biomechanics is non negotiable when addressing angulation translation deformities. The mechanical axis of the lower extremity, defined as a line drawn from the center of the femoral head to the center of the ankle joint, must normally bisect the knee joint just medial to the tibial spines.
Mechanical Axis Deviation and Joint Reactive Forces
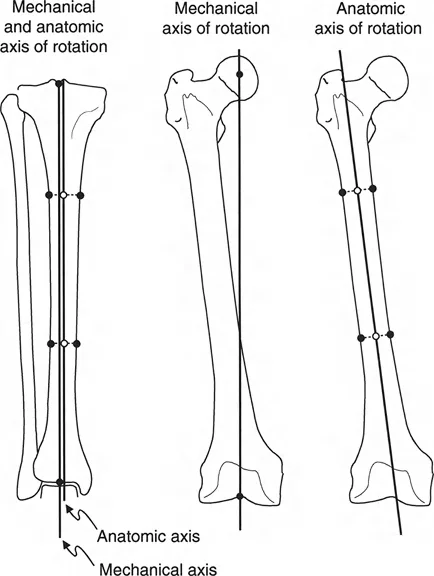
Any deviation from this axis results in Mechanical Axis Deviation. Mechanical Axis Deviation alters the load distribution across the medial and lateral compartments of the knee and ankle. In the presence of a pure translational deformity, the anatomical axes of the proximal and distal segments remain parallel. Because parallel lines never intersect, the Center of Rotation of Angulation is theoretically located at infinity.
However, when angulation is superimposed upon translation, the anatomical axes intersect at a finite point. This intersection is displaced proximally or distally from the actual fracture site or nonunion level. The clinical impact of these deformities is profound. Even minor degrees of uncorrected translation and angulation can shift the Mechanical Axis Deviation outside the central zone of the adjacent joints. This shift exponentially increases joint reactive forces, precipitating early onset, asymmetric osteoarthritis. Cartilage wear is accelerated due to the abnormal shear stresses placed upon the articular surfaces, making precise restoration of the mechanical axis a limb saving necessity.
Oblique Plane Geometry in Multiplanar Deformities
The biomechanical analysis of multiplanar deformities requires an advanced understanding of oblique plane geometry. Deformities rarely confine themselves to the pure coronal or sagittal planes. Instead, a combination of varus or valgus angulation and procurvatum or recurvatum creates a maximal deformity in an oblique plane.
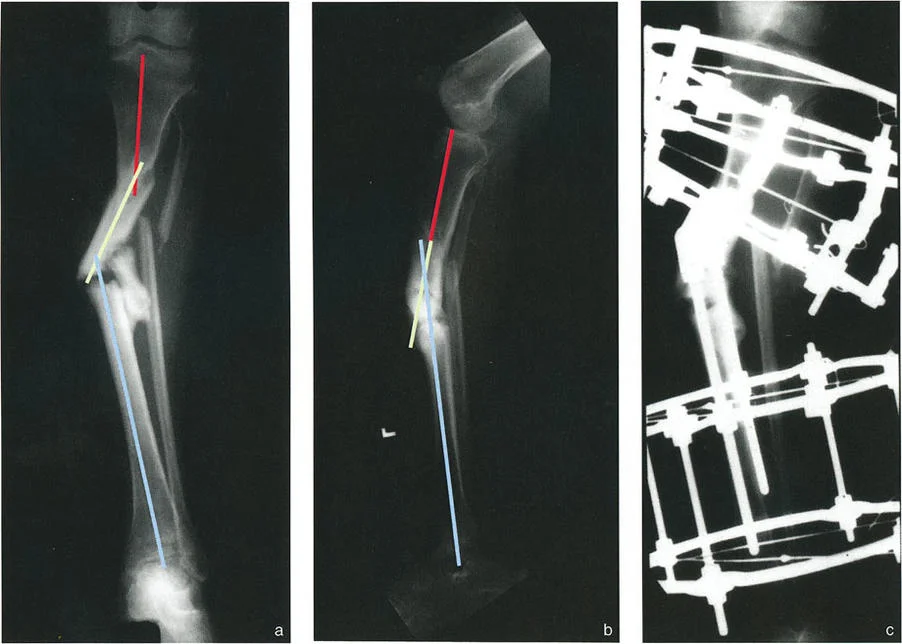
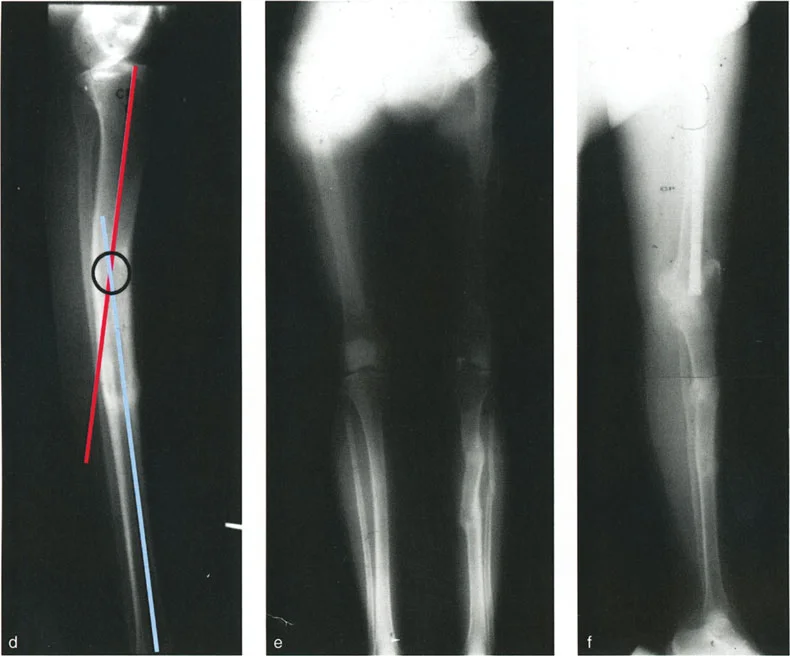
When translation is added to this complex spatial arrangement, the deformity may exhibit two distinct centers of rotation on opposite sides of the nonunion or malunion. For example, an anteroposterior radiograph may demonstrate varus angulation with lateral translation, while the lateral radiograph shows procurvatum angulation with posterior translation. In such cases, the anteroposterior and lateral centers of rotation do not align at the same transverse level. This discrepancy necessitates highly sophisticated preoperative mathematical modeling to determine the true magnitude and orientation of the deformity.
Paley Principles in Angulation Translation Deformities
The cornerstone of modern deformity correction is the systematic approach developed by Dr. Dror Paley. Mastering these principles is the only reliable method for consistently achieving anatomical restoration without inducing iatrogenic secondary deformities.
Defining the Center of Rotation of Angulation
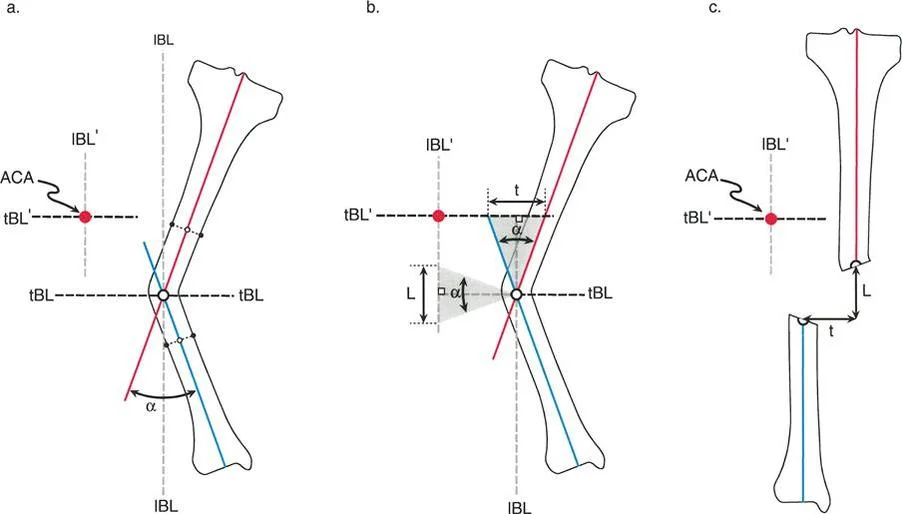
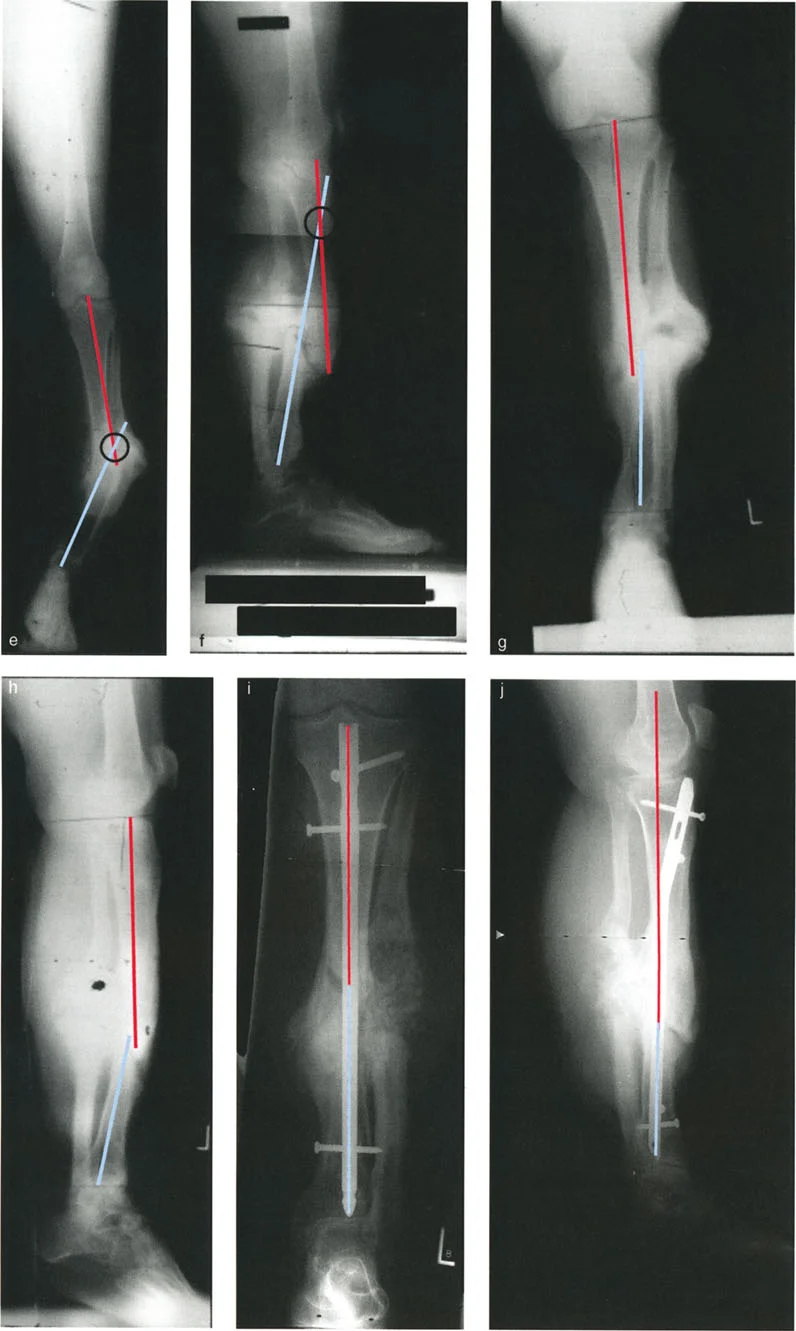
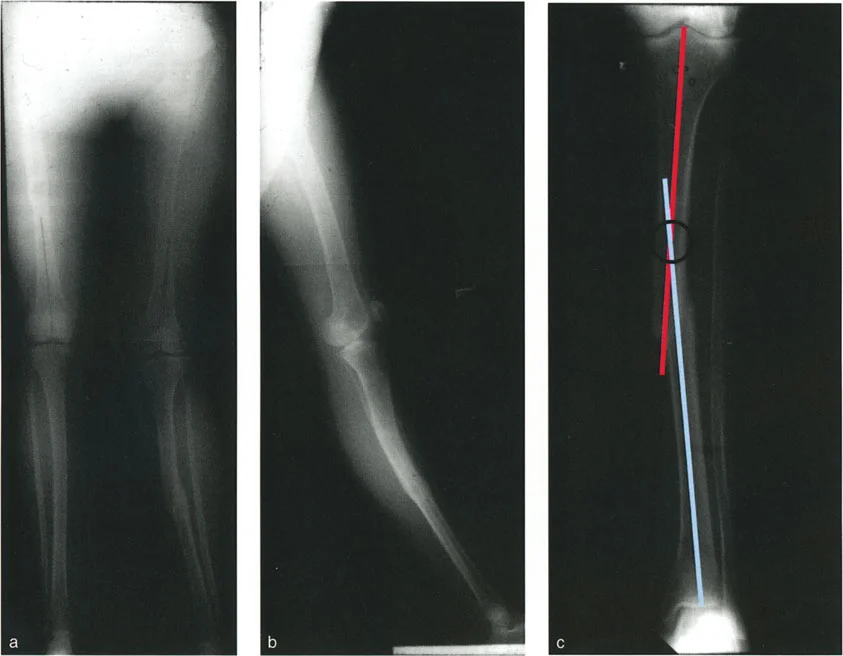
The Center of Rotation of Angulation is the point at which the proximal and distal anatomical or mechanical axes intersect. In a simple angular deformity, the Center of Rotation of Angulation lies directly at the apex of the deformity. However, the defining characteristic of an angulation translation deformity is that the Center of Rotation of Angulation is displaced away from the anatomical apex of the deformity.
This displacement is a critical concept. Failure to recognize the shifted Center of Rotation of Angulation inevitably leads to the creation of secondary iatrogenic deformities during attempted correction. If an osteotomy is performed at the anatomical apex rather than the true Center of Rotation of Angulation, and the bone ends are simply angulated to correct the alignment, a new translation deformity will be created. Conversely, if an osteotomy is performed outside the Center of Rotation of Angulation, the surgeon must purposefully translate the bone ends to achieve a straight axis.
Joint Orientation Angles and Normal Values
To accurately determine the anatomical and mechanical axes, the surgeon must rely on standardized Joint Orientation Angles. These angles define the relationship between the joint lines and the axes of the femur and tibia. Deviations from these normative values indicate the presence and magnitude of a deformity.
| Joint Orientation Angle | Abbreviation | Normal Range | Mean Value |
|---|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 85° - 90° | 87° |
| Medial Proximal Tibial Angle | MPTA | 85° - 90° | 87° |
| Lateral Proximal Femoral Angle | LPFA | 85° - 95° | 90° |
| Lateral Distal Tibial Angle | LDTA | 86° - 92° | 89° |
| Joint Line Convergence Angle | JLCA | 0° - 2° | 1° |
Utilizing these angles allows the surgeon to perform the Malalignment Test and the Malorientation Test. The Malalignment Test determines if the Mechanical Axis Deviation is abnormal. If abnormal, the Malorientation Test isolates whether the source of the deviation is femoral, tibial, or intra articular based on the mLDFA, MPTA, and JLCA.
Applying the Osteotomy Rules
Dr. Paley established three fundamental Osteotomy Rules that govern how a bone responds to surgical cuts and realignments. Understanding these rules is absolutely essential for managing angulation translation deformities.
Osteotomy Rule One
When the osteotomy and the hinge are both placed at the Center of Rotation of Angulation, pure angular correction is achieved without any translation. The anatomical axes will realign perfectly. In angulation translation deformities, the Center of Rotation of Angulation is often in the soft tissues or at a diaphyseal level that is biologically unfavorable for an osteotomy.
Osteotomy Rule Two
When the osteotomy is placed at a different level than the Center of Rotation of Angulation, but the hinge remains at the Center of Rotation of Angulation, the anatomical axes will realign, but the bone ends at the osteotomy site will translate. This is the most frequently utilized rule for angulation translation deformities. The surgeon deliberately uses the translation at the osteotomy site to correct the preexisting translation of the deformity.
Osteotomy Rule Three
When the osteotomy and the hinge are both placed outside the Center of Rotation of Angulation, the anatomical axes will become parallel but will be translated relative to one another. This creates a secondary translation deformity and is generally considered a planning error unless deliberately used to bypass a compromised soft tissue envelope.
Preoperative Planning Step by Step
Meticulous preoperative planning is the difference between a successful reconstruction and a catastrophic failure. The planning process must be systematic, reproducible, and mathematically sound.
Radiographic Evaluation
The foundation of deformity planning is high quality, standardized imaging. Full length, weight bearing, anteroposterior and lateral radiographs of both lower extremities must be obtained. The patella must be positioned facing strictly forward to ensure true orthogonal views of the distal femur and proximal tibia.
Scanograms or standing orthoroentgenograms are utilized to assess leg length discrepancy, which frequently accompanies complex malunions. In cases of severe multiplanar deformity, a computed tomography scan with three dimensional reconstruction is highly recommended to assess rotational malalignment, which cannot be accurately quantified on standard two dimensional radiographs.
Identifying the Apex of Deformity
The planning process follows a strict algorithmic approach to identify the true apex of the deformity and the required correction.
- Draw the Joint Lines: Establish the joint lines of the hip, knee, and ankle based on standardized radiographic landmarks.
- Draw the Proximal Axis: Using the normal joint orientation angles (e.g., mLDFA or MPTA), draw the normal mechanical or anatomical axis of the proximal bone segment extending distally.
- Draw the Distal Axis: Using the normal joint orientation angles for the distal joint, draw the normal axis of the distal bone segment extending proximally.
- Locate the Intersection: The point where these two lines intersect is the Center of Rotation of Angulation.
- Measure the Deformity: The angle formed by the intersection of these two lines represents the true magnitude of the angular deformity.
Calculating the True Deformity Magnitude
In angulation translation deformities, the apparent translation on a radiograph is often deceptive. The magnitude of translation must be measured as the perpendicular distance between the parallel axes of the proximal and distal segments once the angular component has been theoretically neutralized.
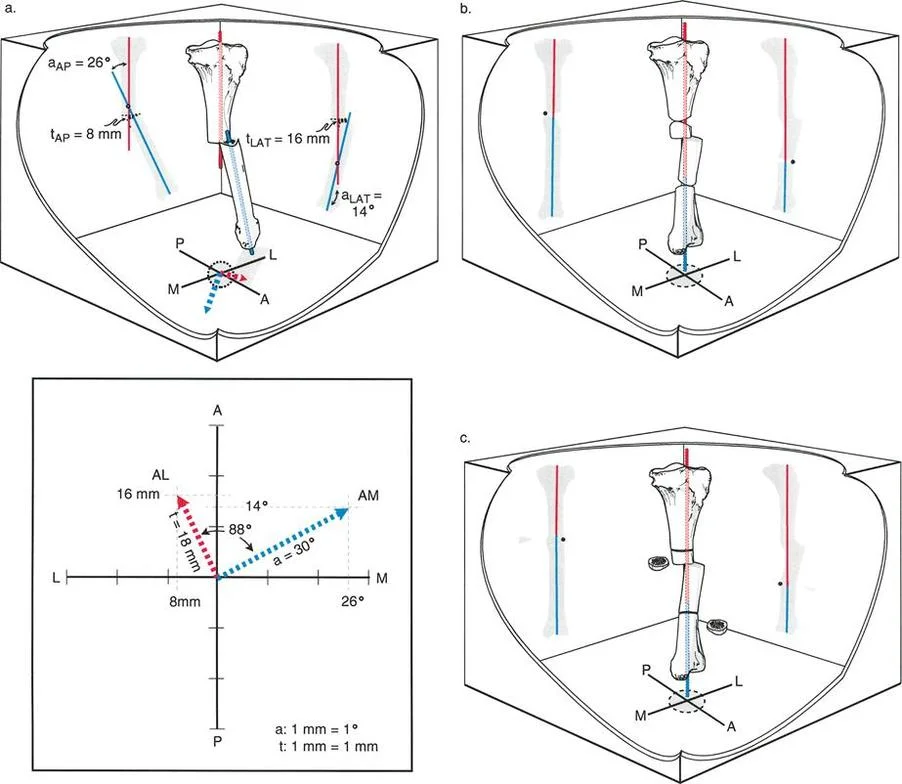
For oblique plane deformities, the surgeon must calculate the true magnitude and orientation of the deformity using trigonometric principles or graphical methods. The true deformity lies in a plane that is rotated away from the standard coronal and sagittal planes. The angle of this plane is determined by calculating the arctangent of the lateral deformity divided by the anteroposterior deformity. Modern digital templating software has simplified this process, but the surgeon must intuitively understand the underlying mathematics to verify the software outputs.
Surgical Execution and Correction Strategies
The transition from preoperative planning to surgical execution requires meticulous soft tissue handling, precise osteotomy techniques, and robust fixation strategies. The choice of surgical technique depends heavily on the magnitude of the deformity, the quality of the surrounding soft tissue, and the presence of any leg length discrepancy.
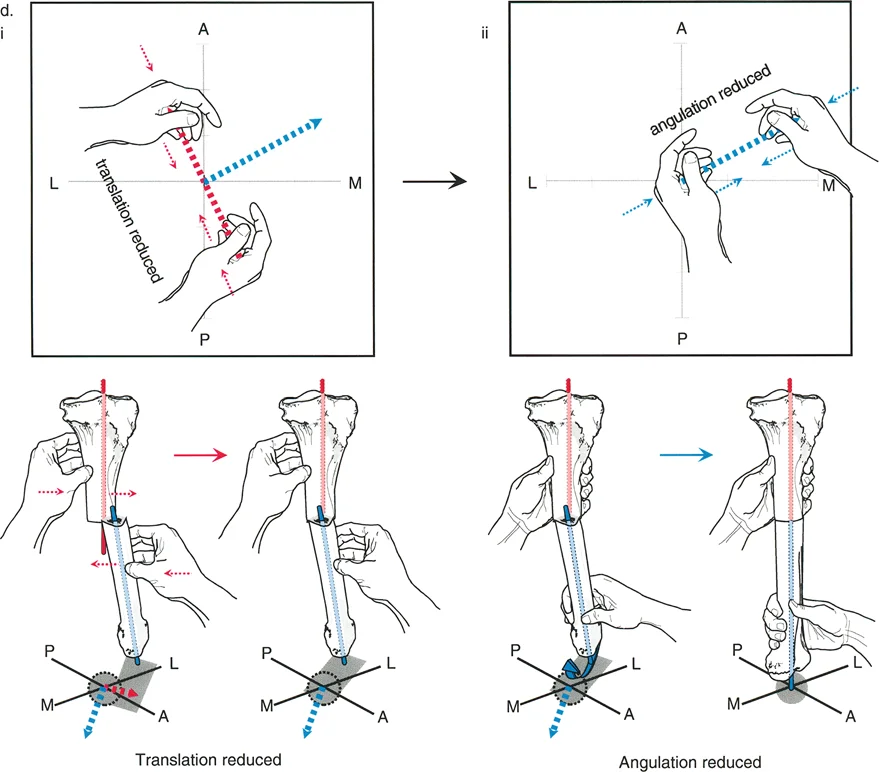
Acute versus Gradual Correction
The decision to correct a deformity acutely or gradually is one of the most critical intraoperative choices.
Acute Correction
Acute correction is typically reserved for mild to moderate deformities where the soft tissue envelope is compliant and can tolerate the sudden change in limb geometry. Acute correction of severe translation can lead to catastrophic neurovascular compromise due to tethering of the vessels and nerves. When performing acute correction, a focal dome osteotomy or a closing wedge osteotomy may be utilized. However, a transverse or oblique osteotomy is often required to allow for the necessary translation to satisfy Osteotomy Rule Two.
Gradual Correction
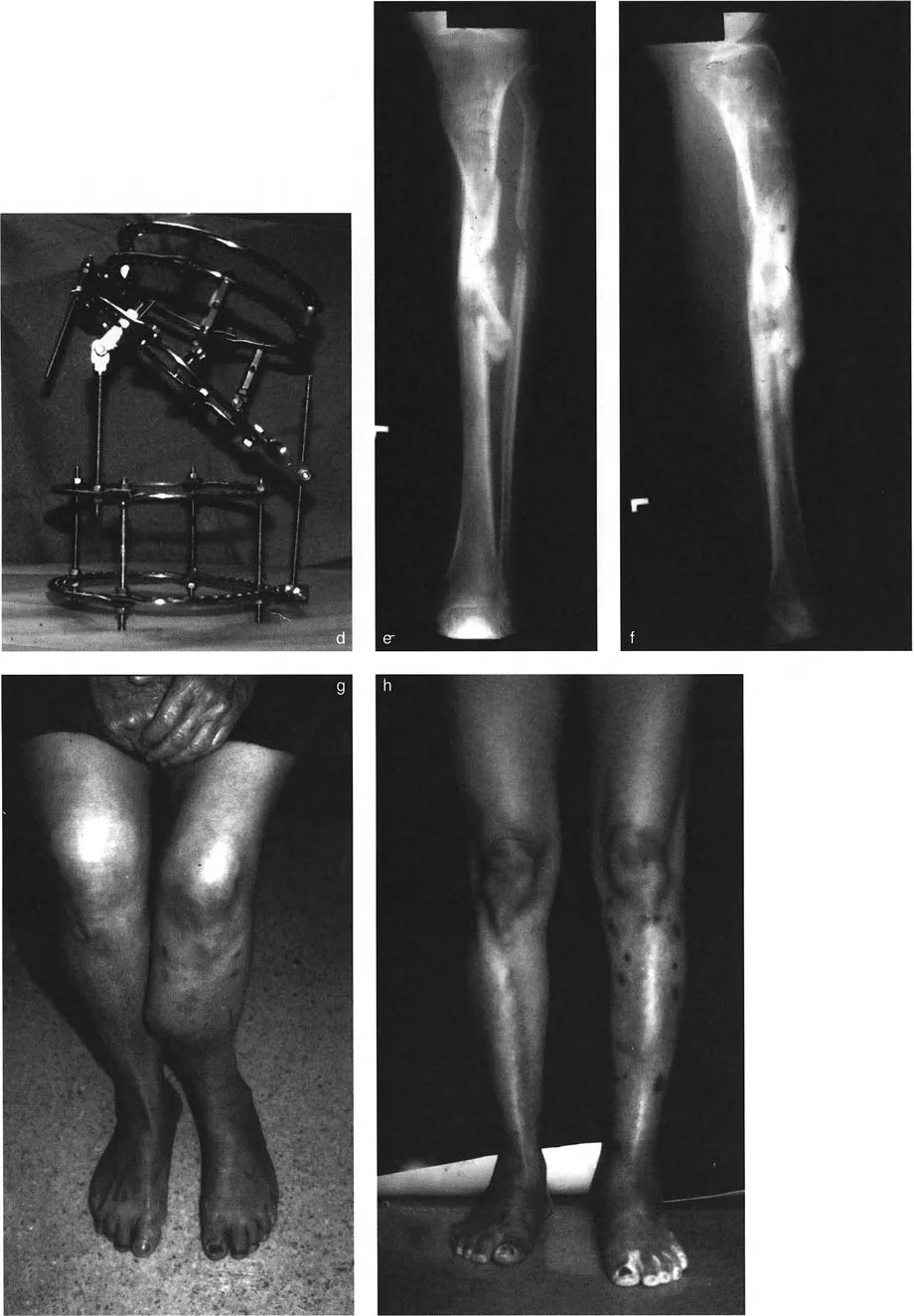
Gradual correction via distraction osteogenesis is the gold standard for severe angulation translation deformities, especially those associated with significant shortening, poor soft tissue quality, or active infection. Gradual correction allows for the simultaneous management of angulation, translation, rotation, and length. The slow distraction process protects the neurovascular structures and generates high quality regenerate bone through the principles of tension stress.
Fixation Constructs and Biomechanical Stability
The choice of fixation construct dictates the biomechanical environment of the osteotomy and influences the rate and quality of bone healing.
Hexapod Circular External Fixators
Hexapod fixators, such as the Taylor Spatial Frame, have revolutionized the management of complex multiplanar deformities. These devices utilize a Stewart Gough platform and sophisticated software to simultaneously correct angulation, translation, rotation, and length. The surgeon inputs the deformity parameters, the mounting parameters, and the frame dimensions into the software, which generates a daily prescription for strut adjustments. This technology is particularly advantageous for angulation translation deformities because it effortlessly manages the displaced Center of Rotation of Angulation and the required translational shifts without requiring complex intraoperative hinge adjustments.
Intramedullary Nailing and Internal Lengthening Devices
Advances in internal fixation have allowed for the acute correction of complex deformities followed by rigid intramedullary stabilization. Techniques such as blocking screws (Poller screws) are essential when using intramedullary nails to correct translation. Blocking screws artificially narrow the medullary canal, forcing the nail into the desired trajectory and preventing the bone segments from translating back into their deformed positions.
More recently, motorized internal lengthening nails have been utilized in conjunction with acute deformity correction. The surgeon acutely corrects the angulation and translation, stabilizes the bone with the internal nail, and then gradually distracts the osteotomy to restore limb length. This hybrid approach minimizes external fixator time and significantly improves patient comfort.
Surgical Pearls for Complex Reconstructions
- Respect the Periosteum: The periosteum is the primary source of osteoprogenitor cells. Perform osteotomies with low energy techniques, such as multiple drill holes connected by an osteotome or a Gigli saw, to minimize thermal necrosis and preserve the periosteal sleeve.
- Prophylactic Fasciotomies: When acutely correcting severe translation or angulation, the fascial compartments can become acutely tensioned. Have a low threshold for performing prophylactic single or double incision fasciotomies to prevent compartment syndrome.
- Neurovascular Monitoring: Always assess distal pulses and nerve function immediately after acute correction. If signals degrade, the correction must be backed off, and a gradual correction strategy must be employed.
- The Reverse Rule Two Concept: If the Center of Rotation of Angulation is located at a poor site for an osteotomy (e.g., near a joint line), perform the osteotomy at the diaphyseal level. To achieve a straight mechanical axis, you must purposefully translate the bone at the osteotomy site. The magnitude and direction of this translation must be precisely calculated during preoperative planning.
Postoperative Management and Clinical Outcomes
The surgical procedure is only the midpoint of the deformity correction journey. Rigorous postoperative management is essential to ensure bone consolidation, maintain joint range of motion, and prevent complications.
Rehabilitation Protocols
Early mobilization is critical. Patients treated with rigid internal fixation or circular external fixators should be encouraged to bear weight as tolerated immediately postoperatively, unless specific bone quality issues dictate otherwise. Weight bearing stimulates axial micromotion at the osteotomy site, which is a potent stimulator of bone healing and callus formation.
Physical therapy must focus on maintaining joint range of motion, particularly in the joints adjacent to the osteotomy. In tibial lengthenings or corrections, aggressive prevention of equinus contractures via splinting and stretching of the Achilles tendon is mandatory.
Managing Complications
Complications in complex deformity correction are frequent and must be anticipated.
- Pin Site Infections: In external fixation, pin site infections are almost universal. They should be managed aggressively with local wound care and oral antibiotics. Intravenous antibiotics or pin removal are reserved for deep infections or pin loosening.
- Premature Consolidation: If distraction is initiated too late or proceeds too slowly, the osteotomy may consolidate prematurely. This requires a return to the operating room for an osteoclasis.
- Delayed Union or Nonunion: Poor regenerate formation can occur due to thermal necrosis during the osteotomy, instability of the fixation construct, or poor patient biology (e.g., smoking). Management includes frame dynamization, autologous bone grafting, or the application of orthobiologics.
The successful management of translation and angulation translation deformities requires a profound understanding of biomechanics, meticulous preoperative planning utilizing Paley's principles, and precise surgical execution. By restoring the mechanical axis and respecting the soft tissue envelope, the orthopedic surgeon can predictably restore function, alleviate pain, and prevent the devastating long term consequences of joint malalignment.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like