Orthopedic Deformity Correction: Mastering Paley's Principles for Angulation & Translation

Key Takeaway
Dr. Paley's principles provide a systematic method for complex orthopedic deformity correction. They focus on Mechanical Axis Deviation, CORA, and joint orientation angles to accurately analyze and correct angulation-translation deformities, preventing joint degeneration.
Understanding Angulation and Translation Deformities
The correction of complex lower extremity deformities requires a profound understanding of three-dimensional geometry, biomechanics, and radiographic analysis. In orthopedic surgery, deformities rarely present as simple, single-plane angulations. More commonly, surgeons encounter a combination of angulation and translation, often complicated by rotational and length discrepancies. Mastering the principles of Dr Dror Paley is essential for orthopedic surgeons, residents, and fellows who wish to accurately analyze and surgically correct these multidimensional malunions and congenital deformities.
Angulation refers to the deviation of the mechanical or anatomic axis from its normal alignment, creating an apex of deformity. Translation, on the other hand, is the parallel displacement of the distal bone segment relative to the proximal segment without a change in the axis angle. When these two elements combine, they create angulation-translation deformities. These complex deformities can occur in anatomic planes (frontal and sagittal) or in oblique non-anatomic planes.
Failure to recognize and address both components will lead to incomplete correction, persistent mechanical axis deviation, and ultimately, early joint degeneration. This comprehensive guide will deconstruct the variants of angulation-translation deformities, applying Paley’s principles to ensure surgical success.
The Core Principles of Dr Dror Paley
Dr Dror Paley revolutionized orthopedic deformity correction by introducing a systematic, reproducible method for analyzing and treating limb malalignment. At the heart of this system are several foundational concepts that every deformity surgeon must internalize.
The first is the Mechanical Axis Deviation. The mechanical axis of the lower extremity is a line drawn from the center of the femoral head to the center of the ankle joint. In a normally aligned limb, this line passes slightly medial to the center of the knee joint. Mechanical Axis Deviation occurs when this line shifts medially (varus) or laterally (valgus).
The second foundational concept is the Center of Rotation of Angulation. The CORA is the point at which the proximal and distal mechanical or anatomic axes intersect. Identifying the CORA is the most critical step in preoperative planning, as it dictates the location of the osteotomy and the placement of the corrective hinge.
Mechanical Axis Deviation and Joint Degeneration
It is a common misconception that only angular deformities cause clinically significant Mechanical Axis Deviation. However, translation alone can profoundly alter the mechanical axis. For example, a pure lateral translation of the distal tibia, even in the absence of frontal plane angulation, will shift the mechanical axis laterally.
This lateral Mechanical Axis Deviation increases the load on the lateral compartment of the knee. Over time, the altered biomechanics lead to cartilage wear, subchondral sclerosis, and the development of lateral compartment osteoarthritis. Clinical follow-ups have demonstrated that patients with uncorrected lateral translation deformities can develop severe degenerative changes decades after the original injury, underscoring the necessity of correcting translation just as aggressively as angulation.
Joint Orientation Angles in Deformity Analysis
To accurately identify the presence and magnitude of a deformity, the surgeon must evaluate the joint orientation angles. These angles define the relationship between the anatomic or mechanical axes of the bone and the joint lines of the hip, knee, and ankle.
In the frontal plane, the key angles include the Mechanical Lateral Distal Femoral Angle, the Medial Proximal Tibial Angle, and the Lateral Distal Tibial Angle. In the sagittal plane, the Posterior Distal Femoral Angle and the Posterior Proximal Tibial Angle are evaluated.
By comparing the patient's measured angles against established normal population values, the surgeon can pinpoint exactly which bone segment is contributing to the Mechanical Axis Deviation.
Normal Values for Lower Extremity Alignment
Understanding the normal reference ranges is critical for templating and planning the correction. The table below summarizes the standard joint orientation angles used in Paley's analysis.
| Joint Orientation Angle | Abbreviation | Normal Range | Average Value |
|---|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 85° - 90° | 87° |
| Medial Proximal Tibial Angle | MPTA | 85° - 90° | 87° |
| Lateral Distal Tibial Angle | LDTA | 86° - 92° | 89° |
| Posterior Distal Femoral Angle | PDFA | 79° - 87° | 83° |
| Posterior Proximal Tibial Angle | PPTA | 77° - 84° | 81° |
| Joint Line Congruency Angle | JLCA | 0° - 2° | 0° |
When evaluating a malunion, if the MPTA is measured at 75 degrees, the surgeon immediately recognizes a 12-degree varus deformity originating in the proximal tibia. However, identifying the angulation is only the first step; the surgeon must then locate the CORA.
The Concept of the Center of Rotation of Angulation
The Center of Rotation of Angulation is the geometric cornerstone of deformity correction. To find the CORA, the surgeon draws the mid-diaphyseal line of the proximal bone segment and the mid-diaphyseal line of the distal bone segment. The point where these two lines intersect is the CORA.
In a simple angular deformity, the CORA corresponds exactly to the apex of the deformity, which is usually the site of the old fracture or the apex of the bent bone. However, when translation is introduced, the relationship between the fracture site and the CORA becomes more complex.
Identifying the CORA in Complex Malunions
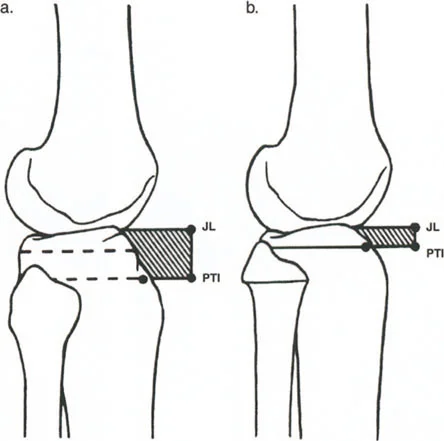
When a bone heals with both angulation and translation, the anatomic axes of the proximal and distal segments will still intersect, but the intersection point (the CORA) will no longer sit precisely at the level of the fracture. The translation shifts the distal axis parallel to itself, which effectively moves the intersection point proximally or distally along the proximal axis.
This phenomenon is the key to diagnosing translation on a radiograph. If the calculated CORA does not align with the obvious level of the fracture or the apex of the angular deformity, the surgeon must suspect a translational component. The distance between the fracture level and the CORA is directly proportional to the magnitude of the translation.

Variants of Angulation and Translation Deformities
Dr Paley classifies angulation-translation deformities into specific variants based on the relationship between the plane of angulation and the plane of translation. Understanding these variants is crucial for visualizing the deformity in three dimensions and planning the appropriate radiographic views for analysis.
Variant One Anatomic Planes Ninety Degrees Apart
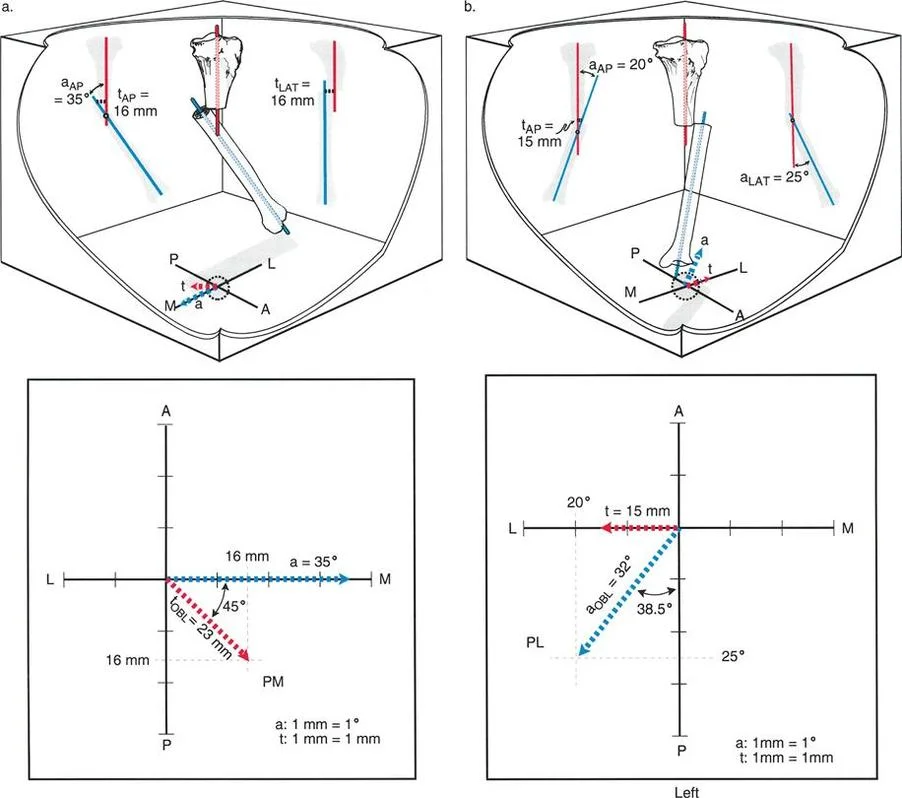
In the first variant, the deformity presents with angulation in one anatomic plane and translation in the orthogonal anatomic plane. The planes are perpendicular to each other, meaning the angle between the plane of angulation and the plane of translation is exactly 90 degrees.
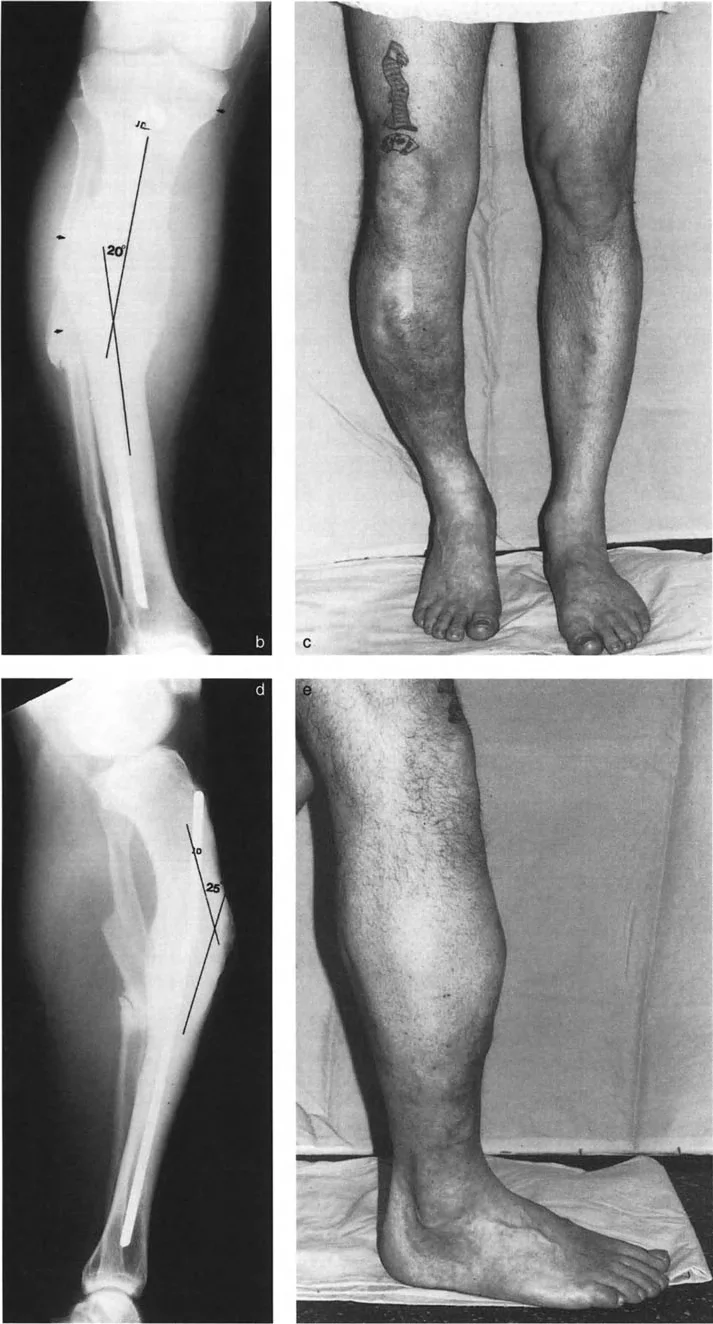
For example, consider a left tibial malunion with varus angulation in the frontal (anteroposterior) plane and pure anterior translation in the sagittal (lateral) plane.
When evaluating the anteroposterior radiograph, the surgeon will observe the varus angulation. Because there is no translation in the frontal plane, the proximal and distal anatomic axes will intersect exactly at the level of the fracture. The CORA is at the fracture site.
When evaluating the lateral radiograph, the surgeon will observe anterior translation but no recurvatum or procurvatum angulation. The proximal and distal axes are parallel.
If we plot this graphically, with angulation on the x-axis and translation on the y-axis, the angle between the two lines is 90 degrees. The clinical significance of Variant One is that the deformity can be fully analyzed using standard orthogonal anteroposterior and lateral radiographs, as the deformity components align perfectly with the anatomic planes.
Variant Two Oblique Planes Ninety Degrees Apart
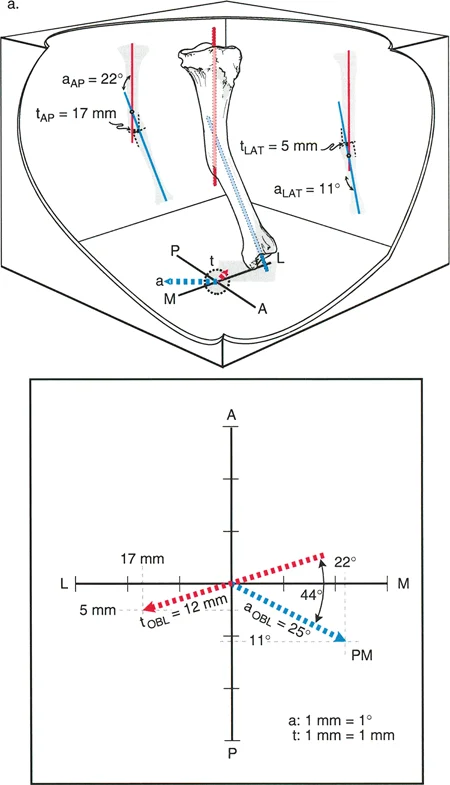
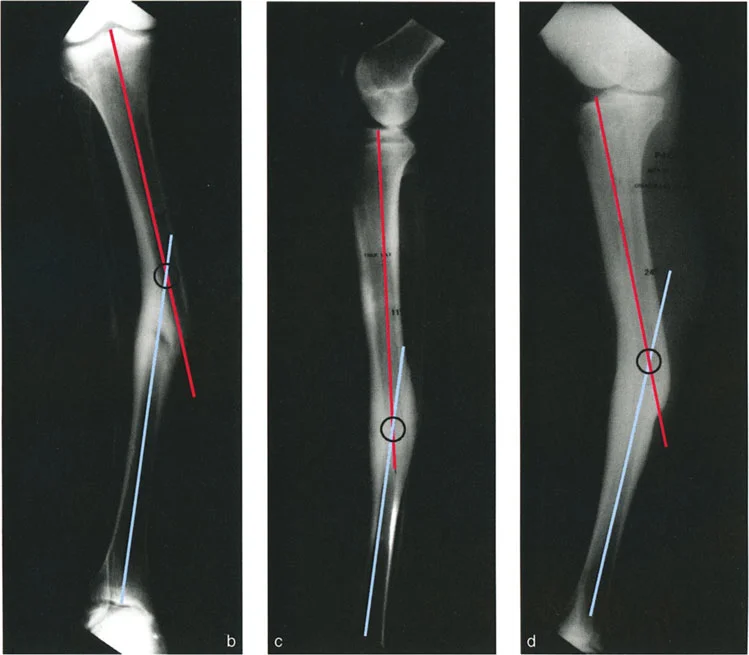
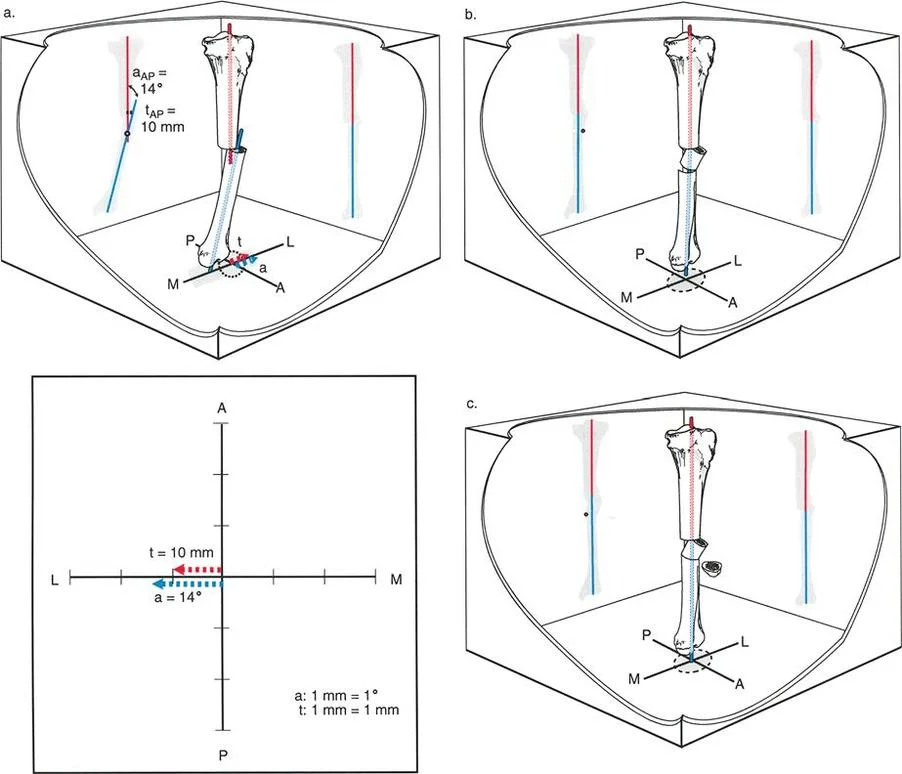
Variant Two represents a significant increase in complexity. In this scenario, the angulation and translation are still 90 degrees apart, but they exist in oblique, non-anatomic planes.
Because the deformity planes are oblique to the standard radiographic beams, both the anteroposterior and lateral radiographs will display a combination of angulation and translation. This is a classic projectional phenomenon. A single oblique angular deformity will project a component of that angulation onto both the AP and lateral films. Similarly, the oblique translation will project onto both films.
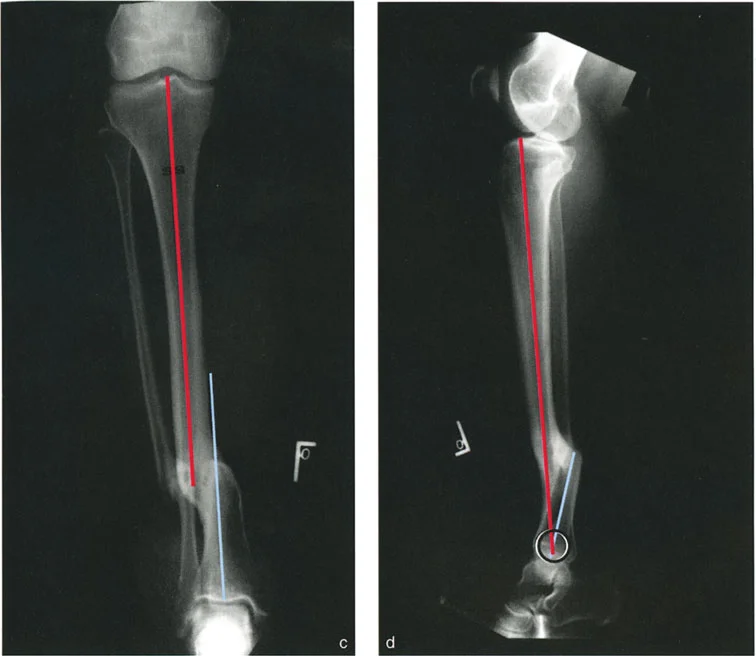
The hallmark of Variant Two is the behavior of the CORA. When the surgeon draws the axes on the anteroposterior radiograph, the CORA will be found at a level different from the fracture site (for example, proximal to the fracture). When the axes are drawn on the lateral radiograph, the CORA will also be at a different level, but in the opposite direction (for example, distal to the fracture).
The fact that the CORAs on the orthogonal views are at different levels is the absolute diagnostic indicator that the angulation and translation exist in different oblique planes.
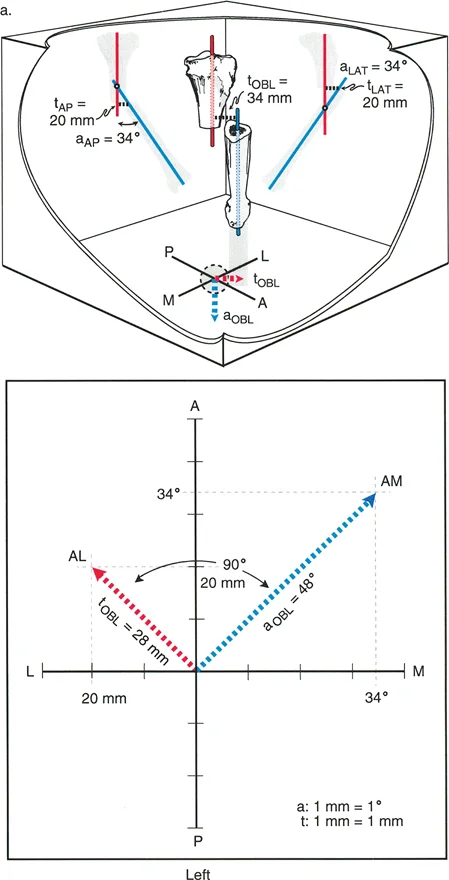
To accurately assess the true magnitude of the angulation in Variant Two, the surgeon must obtain an oblique radiograph perpendicular to the plane of maximum angulation. On this specific oblique view, the surgeon will see the maximum angulation, but zero translation. Furthermore, on this view, the CORA will map perfectly to the fracture level. Conversely, an orthogonal oblique radiograph taken 90 degrees to the first will show the maximum translation with zero angulation.
Variant Three Planes Less Than Ninety Degrees Apart
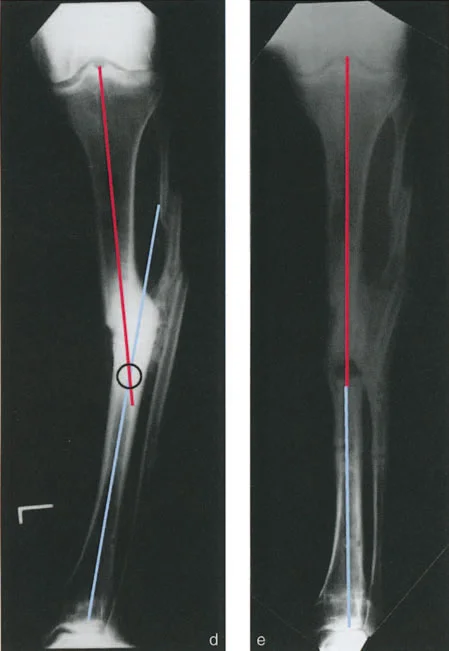
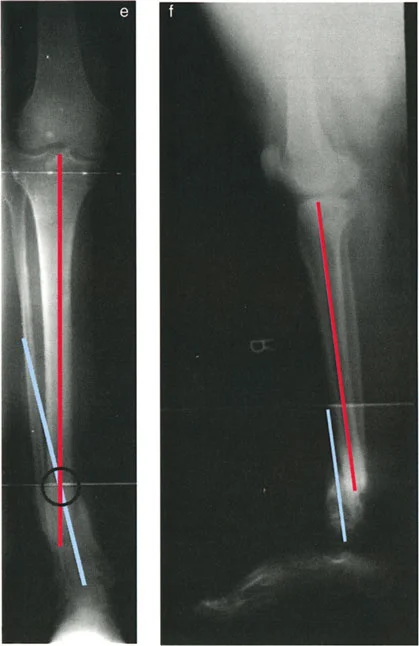
In Variant Three, the planes of angulation and translation are different, but the angle between them is less than 90 degrees. This occurs when one component of the deformity (either angulation or translation) lies in an anatomic plane, while the other component lies in an oblique plane.
Radiographically, this presents uniquely. On one of the standard anatomic reference radiographs (either the AP or the lateral), the surgeon will observe both angulation and translation. However, on the orthogonal standard radiograph, the surgeon will observe only angulation or only translation.
For instance, the AP radiograph might show both varus angulation and lateral translation. The lateral radiograph, however, might show only anterior translation with no sagittal angulation. Because the translation appears on both the AP and lateral views, it must exist in an oblique plane. Because the angulation appears only on the AP view and not on the lateral view, the angulation exists purely in the frontal (anatomic) plane.
When plotted graphically, the planes of angulation and translation are distinct but separated by an angle of less than 90 degrees. Analyzing Variant Three requires trigonometric calculation or specialized software to determine the true magnitude and plane of the oblique component before applying the osteotomy rules.
Applying Paleys Osteotomy Rules to Complex Deformities
Once the CORA has been identified and the planes of angulation and translation have been mapped, the surgeon must plan the surgical correction. Dr Paley established three fundamental Osteotomy Rules that dictate how the bone will behave based on where the bone is cut (the osteotomy) and where the correction pivots (the hinge).
Understanding these rules is non-negotiable for correcting angulation-translation deformities, as the strategic placement of the hinge can be used to intentionally create translation to counteract an existing translational deformity.
Rule One The Osteotomy and Hinge at the CORA
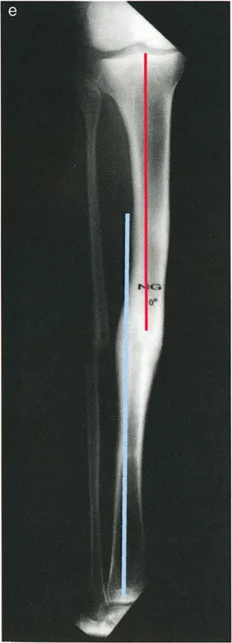
Paley's First Osteotomy Rule states that if the osteotomy and the corrective hinge are both placed at the CORA, the angular deformity will be corrected without introducing any new translation. The anatomic axes of the proximal and distal segments will become collinear.
In the context of an angulation-translation deformity, Rule One is often insufficient. If a patient has a malunion with both varus angulation and lateral translation, performing a Rule One osteotomy at the CORA will correct the varus, but the lateral translation will remain. The axes will be parallel but not collinear, leaving the patient with a persistent Mechanical Axis Deviation.
Rule Two The Osteotomy Away From the CORA
Paley's Second Osteotomy Rule states that if the osteotomy is performed at a level different from the CORA, but the corrective hinge is placed exactly on the CORA, the angulation will be corrected, and the anatomic axes will become collinear.
This is a highly useful rule in clinical practice. Often, the CORA is located in the diaphysis where bone healing is slower, or near a joint where fixation is difficult. By using Rule Two, the surgeon can place the osteotomy in well-vascularized metaphyseal bone while keeping the hinge at the diaphyseal CORA.
Crucially, when a Rule Two correction is executed, the bone ends at the osteotomy site will translate relative to each other. The surgeon must anticipate this translation and ensure the fixation construct (such as an intramedullary nail or a circular frame) can accommodate it.
Rule Three The Osteotomy and Hinge Away From the CORA
Paley's Third Osteotomy Rule states that if both the osteotomy and the corrective hinge are placed away from the CORA, the angular deformity will be corrected, but a new translation deformity will be created. The proximal and distal axes will end up parallel, but not collinear.
In standard angular corrections, Rule Three is an error that leads to iatrogenic translation and Mechanical Axis Deviation. However, in the treatment of angulation-translation deformities, Rule Three becomes a powerful tool.
If a patient presents with an existing translation deformity, the surgeon can intentionally design a Rule Three osteotomy. By calculating the exact distance to place the hinge away from the CORA, the surgeon can force the osteotomy to generate a translation that is equal and opposite to the patient's existing translation. As the hinge is turned, the angulation corrects, and the iatrogenic translation perfectly cancels out the pathologic translation, resulting in a perfectly aligned limb.

Step by Step Preoperative Planning for Correction
Successful deformity correction is won or lost in the preoperative planning phase. Surgeons must approach planning with meticulous attention to detail, utilizing both clinical examination and advanced imaging.
Clinical and Radiographic Evaluation
- Clinical Assessment: Evaluate the patient's gait, rotational profile, and leg length discrepancy. Assess joint range of motion and ligamentous stability. Remember that apparent translation can sometimes be masked or exaggerated by rotational deformities.
- Full-Length Radiographs: Obtain weight-bearing, full-length, 51-inch anteroposterior radiographs of both lower extremities with the patellae oriented strictly forward. Obtain full-length lateral radiographs.
- Identify the Mechanical Axis: Draw the mechanical axis from the center of the femoral head to the center of the ankle mortise. Measure the Mechanical Axis Deviation in millimeters.
- Measure Joint Orientation Angles: Calculate the mLDFA, MPTA, LDTA, and joint line congruency angles. Compare these to normal values to localize the source of the deformity.
Graphical Analysis and Templating
- Draw the Axes: On both the AP and lateral radiographs, draw the mid-diaphyseal lines for the proximal and distal segments of the deformed bone.
- Locate the CORA: Mark the intersection of these axes. Note the relationship between the CORA and the fracture site/apex of deformity.
- Determine the Variant: Evaluate the AP and lateral CORAs. If they are at the same level as the fracture, it is a pure angular deformity. If they are at different levels, map the planes to determine if it is Variant One, Two, or Three.
- Plan the Osteotomy: Select the osteotomy site based on bone quality, soft tissue envelope, and planned fixation.
- Position the Hinge: Apply Paley's Osteotomy Rules. If using a circular external fixator, plan the placement of the physical hinges. If using an intramedullary nail or plate, plan the virtual hinge point and calculate the required translation at the osteotomy site.

Surgical Pearls for Deformity Correction
Executing a complex angulation-translation correction in the operating room requires technical precision and the right choice of hardware.
- Respect the Soft Tissues: Translation maneuvers place significant stress on the neurovascular structures. When planning a correction that involves substantial translation, consider a gradual correction using a circular frame rather than acute correction with internal fixation to prevent neurovascular compromise or compartment syndrome.
- The Taylor Spatial Frame: For complex oblique plane deformities (Variant Two and Three), hexapod circular fixators like the Taylor Spatial Frame (TSF) are invaluable. The TSF utilizes a virtual hinge, allowing the software to calculate the simultaneous correction of angulation, translation, rotation, and length in all six degrees of freedom.
- Fibular Osteotomy: In tibial deformity correction, the fibula acts as a tether. A fibular osteotomy is almost always required. Ensure the fibular cut is made at a different level than the tibial cut to minimize the risk of cross-union.
- Prophylactic Fasciotomy: Acute correction of translation, particularly in the tibia, drastically changes the volume of the fascial compartments. Have a low threshold for performing a prophylactic anterior and lateral compartment fasciotomy.
- Intramedullary Nailing Techniques: If correcting acutely with an intramedullary nail, use blocking screws (Poller screws) strategically placed in the concavity of the deformity. Blocking screws narrow the medullary canal, forcing the nail to translate the bone fragments into the desired alignment and preventing the nail from following the path of the original deformity.
Fixation Strategies and Postoperative Management
The choice of fixation depends on the magnitude of the deformity, the presence of leg length discrepancy, and patient compliance.
Internal fixation (plates or nails) is preferred for acute corrections where the soft tissue envelope allows for immediate translation. It offers better patient comfort and avoids pin-site infections. However, it is unforgiving; the correction must be perfect on the operating table.
External fixation (Ilizarov or Hexapod frames) is the gold standard for gradual correction. It allows for postoperative adjustments, making it ideal for severe angulation-translation deformities where acute correction would stretch the peroneal or tibial nerves beyond their tolerance.
Postoperatively, patients undergoing gradual correction require close monitoring. Radiographs should be obtained every 7 to 14 days to ensure the bone is translating and angulating exactly as planned by the software or the mechanical hinge placement. Physical therapy is mandatory to prevent joint contractures, particularly equinus contractures of the ankle during tibial lengthening and translation.
By rigorously applying Dr Paley's principles of the CORA, understanding the geometric variants of angulation and translation, and strictly adhering to the Osteotomy Rules, orthopedic surgeons can confidently tackle the most challenging lower extremity deformities, restoring mechanical alignment and preserving joint longevity.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like