Mastering Multiapical Deformity Correction: Advanced Osteotomy & Paley Principles
Key Takeaway
Frontal plane realignment corrects complex multiapical deformities, often in the tibia, using Paley principles. It involves precise analysis of Mechanical Axis Deviation, joint orientation angles, and CORA methodology to plan single or multilevel osteotomies, restoring optimal biomechanics and preventing joint degeneration.
Introduction to Frontal Plane Realignment and Deformity Correction
In the realm of advanced orthopedic surgery, mastering frontal plane realignment is the cornerstone of preserving joint longevity, restoring optimal biomechanics, and preventing early onset osteoarthritis. Historically, deformity correction was more of an art than a science, heavily reliant on the surgeon estimating alignment based on visual inspection. The paradigm shifted definitively with the introduction of Dr Dror Paley and his systematic, mathematically rigorous principles of deformity analysis.
For the orthopedic surgeon in training, understanding the interplay between the Mechanical Axis Deviation, the Center of Rotation of Angulation, and joint orientation angles is absolutely non negotiable. This comprehensive guide dives deep into the complexities of multiapical deformities, specifically in the tibia, and explores why single level osteotomies often fail in the face of sweeping bows or complex, multi level angular deviations.
By deconstructing the biomechanics of single versus multilevel osteotomy solutions, we will illuminate the hidden pitfalls of deformity correction, such as inadvertently uncovering a maloriented joint. Mastery of these concepts elevates the orthopedic surgeon from a mere bone carpenter to an architect of biomechanical restoration.
Foundational Paley Principles for Orthopedic Surgeons
Before analyzing complex multiapical deformities, one must have absolute fluency in the language of Paley deformity correction. The systematic approach removes guesswork, allowing for precise, reproducible surgical planning.
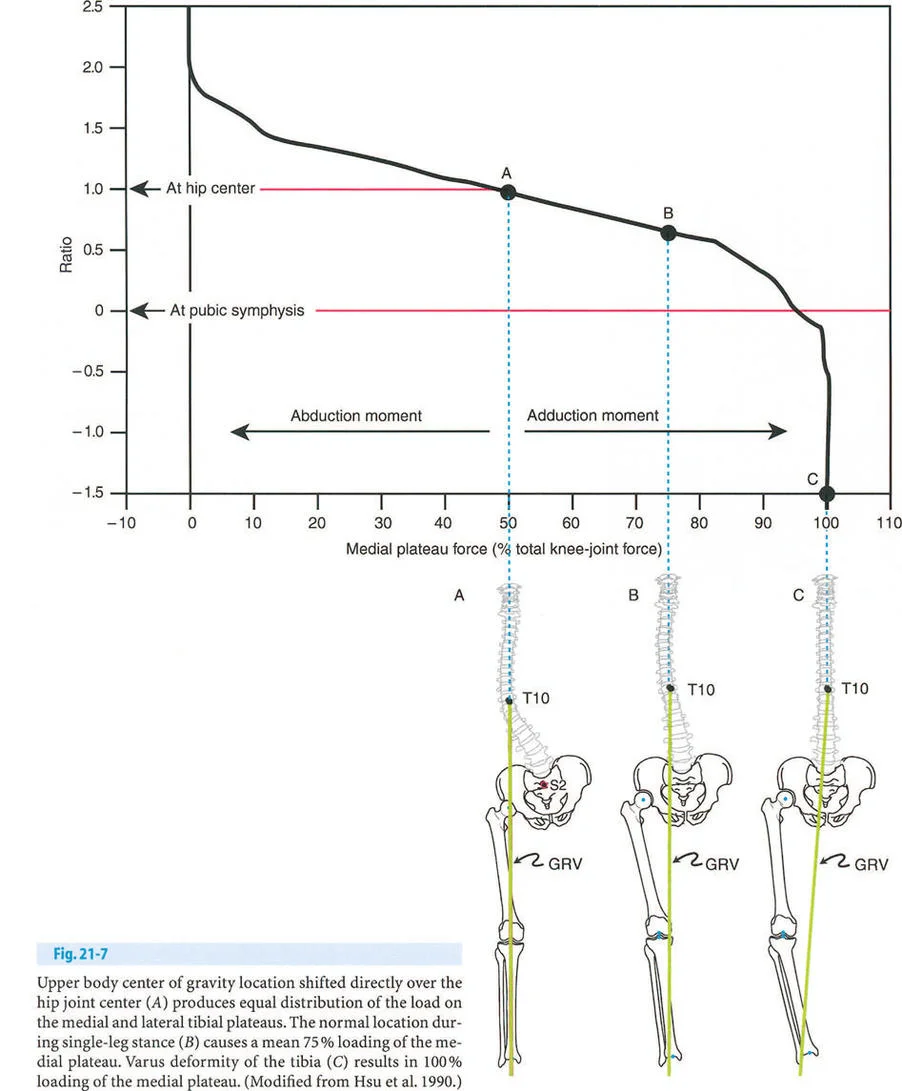
Understanding the Mechanical Axis and MAD
The mechanical axis of the lower extremity is a straight line drawn from the center of the femoral head to the center of the ankle joint at the tibial plafond. In a normally aligned limb, this line passes precisely through the center of the knee joint. When this line deviates medially or laterally from the knee center, we define the magnitude of this shift as the Mechanical Axis Deviation.
Calculating the Mechanical Axis Deviation is the first step in the Malalignment Test. A medial Mechanical Axis Deviation indicates a varus deformity, leading to mechanical overload of the medial compartment of the knee. Conversely, a lateral Mechanical Axis Deviation indicates a valgus deformity, overloading the lateral compartment. Quantifying this deviation in millimeters allows the surgeon to understand the severity of the load shifting and serves as the baseline metric for postoperative success.
Joint Orientation Angles and Biomechanics
Restoring the Mechanical Axis Deviation to neutral is only half the battle. A straight leg with crooked joints will rapidly degenerate due to abnormal sheer forces across the articular cartilage. Joint orientation angles measure the relationship between the mechanical or anatomic axis of a bone and its respective joint line.
Orthopedic surgeons must memorize the normal population averages and standard deviations for these angles to identify joint malorientation accurately.
| Joint Orientation Angle | Abbreviation | Normal Range | Average Value | Clinical Significance |
|---|---|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 85° to 90° | 88° | Determines distal femoral frontal plane alignment. Abnormalities lead to femoral varus or valgus. |
| Medial Proximal Tibial Angle | MPTA | 85° to 90° | 87° | Determines proximal tibial frontal plane alignment. Crucial for High Tibial Osteotomy planning. |
| Lateral Distal Tibial Angle | LDTA | 86° to 92° | 89° | Evaluates ankle joint orientation. Deviations cause massive eccentric loading on the tibial plafond. |
| Joint Line Congruency Angle | JLCA | 0° to 2° | 0° | Measures the parallelism of the knee joint. Increased JLCA indicates ligamentous laxity or cartilage loss. |
When the Mechanical Axis Deviation is abnormal, the surgeon must perform the Malorientation Test, evaluating the mLDFA, MPTA, and LDTA to determine whether the deformity originates in the femur, the tibia, or both.
The CORA Methodology Explained
The Center of Rotation of Angulation is the foundational geometric concept for localizing a deformity. It is defined as the intersection point of the Proximal Mechanical Axis and the Distal Mechanical Axis.
To find the Center of Rotation of Angulation, the surgeon must draw the Proximal Mechanical Axis as a line originating from the center of the proximal joint, oriented at the normal joint orientation angle. Simultaneously, the Distal Mechanical Axis is drawn from the center of the distal joint, oriented at its respective normal joint orientation angle. The intersection of these two lines dictates both the magnitude and the exact location of the deformity.
However, what happens when a bone has more than one deformity. This brings us to the multiapical conundrum, where standard single intersection analysis falls short.
Paley Osteotomy Rules in Deformity Correction
To safely execute a correction once the Center of Rotation of Angulation is identified, surgeons must strictly adhere to the three Paley Osteotomy Rules. These rules dictate the relationship between the osteotomy cut, the hinge point, and the resulting bone movement.
Paley Osteotomy Rule One
When the osteotomy and the hinge are both placed exactly at the Center of Rotation of Angulation, the bone ends will angulate purely without any translation. The mechanical axis of the proximal segment will perfectly align with the mechanical axis of the distal segment. This is the ideal scenario for a simple, uniapical deformity, resulting in a collinear mechanical axis and excellent bone contact.
Paley Osteotomy Rule Two
When the osteotomy is made at a different level than the Center of Rotation of Angulation, but the hinge remains at the Center of Rotation of Angulation, the correction will result in both angulation and translation at the osteotomy site. The mechanical axes will still realign perfectly. This rule is highly useful when the Center of Rotation of Angulation is located near a joint or in poor quality bone, allowing the surgeon to cut diaphyseal bone while still achieving perfect axis realignment through calculated translation.
Paley Osteotomy Rule Three
When the osteotomy and the hinge are both placed away from the Center of Rotation of Angulation, a translation deformity will be created. The proximal and distal mechanical axes will end up parallel but not collinear. This rule highlights a common surgical error when surgeons fail to identify the true Center of Rotation of Angulation, resulting in a zigzag mechanical axis that fails to restore normal load bearing biomechanics.
The Challenge of Multiapical Tibial Deformities
A multiapical deformity exists when a bone has more than one distinct apex of angulation, or when it presents as a sweeping bow. These complex deformities are commonly seen in metabolic bone diseases such as rickets, Paget disease, osteogenesis imperfecta, or following complex malunited segmental fractures.
When analyzing a multiapical deformity, the standard single Center of Rotation of Angulation analysis can lead the unwary surgeon into a devastating trap. If the surgeon only draws a single Proximal Mechanical Axis and a single Distal Mechanical Axis, they will inevitably find a single intersection point. However, executing a single osteotomy at this point can have catastrophic consequences for the adjacent joints.
Defining Compensatory Deformities
In many multiapical scenarios, a primary deformity in the diaphysis is accompanied by a secondary, compensatory deformity near the joint. The body naturally attempts to keep the foot plantigrade and the knee joint horizontal to the ground. If a severe diaphyseal valgus develops, the distal tibia may slowly remodel into varus to keep the ankle joint line parallel to the floor. This compensatory curve masks the true extent of the joint malorientation.
Step by Step Preoperative Planning for Multiapical Deformities
To avoid surgical disasters, orthopedic surgeons must utilize a meticulous, step by step approach to preoperative planning for any suspected sweeping bow or multiapical deformity.
- Obtain standardized, full length, weight bearing standing radiographs of both lower extremities.
- Assess the Mechanical Axis Deviation to quantify the overall limb malalignment.
- Perform the Malorientation Test by measuring the mLDFA, MPTA, and LDTA.
- Draw the Proximal Mechanical Axis using the normal MPTA.
- Draw the Distal Mechanical Axis using the normal LDTA.
- Trace the mid diaphyseal line of the bone.
- Identify intersections between the mid diaphyseal line and the Proximal Mechanical Axis, as well as the Distal Mechanical Axis. Multiple intersections indicate multiple Centers of Rotation of Angulation.
Analyzing the Single Osteotomy Pitfall
Let us examine the catastrophic potential of ignoring multiapical principles visually and mathematically through a classic tibial multiapical deformity scenario.
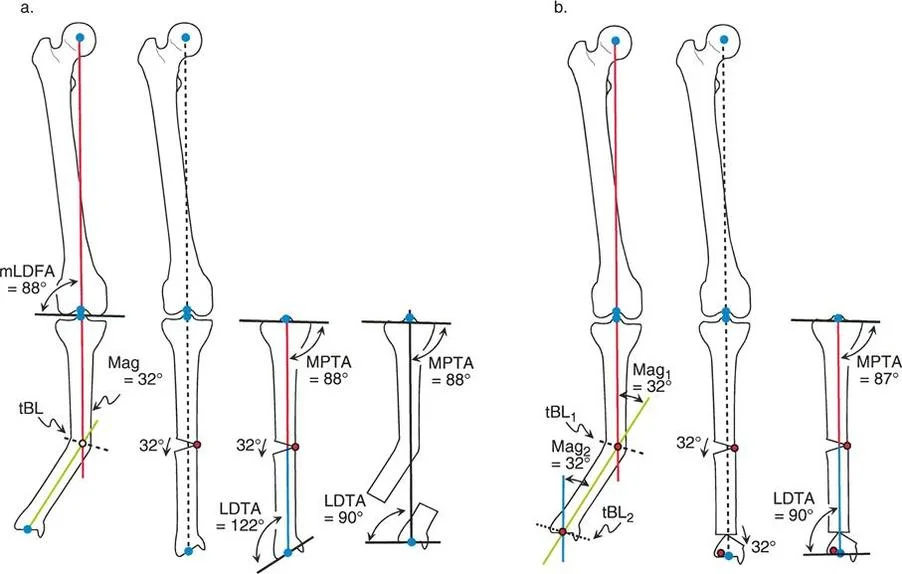
Preoperative Assessment of the Diaphyseal Valgus
Refer to the left side of the diagram illustrating a single osteotomy solution for a multiapical tibial deformity. The patient presents with an obvious diaphyseal valgus deformity. Clinical examination and initial radiographic measurements indicate the magnitude of this overall deformity is 32 degrees.
To plan the correction, the novice surgeon draws the Proximal Mechanical Axis down from the knee, ensuring the MPTA is set to a normal 88 degrees. They then draw the Distal Mechanical Axis up from the ankle. These two lines intersect in the mid diaphysis, perfectly matching the apex of the most obvious clinical deformity. The surgeon concludes that a single 32 degree correction at this diaphyseal Center of Rotation of Angulation will resolve the issue.
Surgical Execution and Unintended Consequences
The surgeon proceeds to the operating room and performs a single opening wedge osteotomy at this mid diaphyseal location, correcting the 32 degree angular deformity.
At first glance on the postoperative anteroposterior radiograph, the result seems highly successful. The mechanical axis of the entire limb is now perfectly realigned. A plumb line dropped from the center of the femoral head passes straight through the center of the knee and the center of the ankle. Furthermore, the knee joint orientation is completely normal, maintaining an MPTA of 88 degrees.
However, a critical evaluation of the distal segment reveals that the ankle joint has been completely destroyed biomechanically. Look closely at the LDTA in the postoperative diagram. The LDTA is now a staggering 122 degrees. The ankle has been forced into severe, unphysiological varus.
Biomechanical Failure of the Single Osteotomy
This scenario represents the classic pitfall of utilizing a single osteotomy in a multiapical deformity. The original tibia did not merely possess a single diaphyseal bend. It also harbored a compensatory, secondary deformity near the ankle joint. By forcing a single intersection point between the extreme proximal and extreme distal axes, the surgeon completely ignored the distal deformity.
The single 32 degree correction successfully realigned the global mechanical axis, but in doing so, it uncovered the varus maloriented ankle. When the distal tibial segment was rotated 32 degrees to correct the diaphyseal valgus, the ankle joint line was simultaneously tilted by 32 degrees.
An ankle with an LDTA of 122 degrees will experience massive eccentric loading on the medial tibial plafond. The sheer forces across the articular cartilage will be immense, leading to rapid, painful, and debilitating osteoarthritis within a few short years, eventually requiring ankle arthrodesis or total ankle arthroplasty.
The Translation Alternative and Its Limitations
Could we fix this multiapical deformity with a single osteotomy utilizing translation based on Paley Osteotomy Rule Two. As theoretical geometry dictates, a single osteotomy utilizing massive medial translation can align the mechanical axis without tilting the joint.
However, while mathematically possible, it is practically impossible in a clinical surgical setting. The amount of translation required at any single diaphyseal level to correct a 32 degree multiapical deformity without altering the joint angle would result in the proximal and distal bone segments losing all cortical contact.
Attempting this massive translation leads to several insurmountable surgical complications. First, the soft tissue envelope cannot accommodate such extreme sheer displacement, leading to high risks of skin necrosis and compartment syndrome. Second, the lack of bone to bone contact virtually guarantees a nonunion, requiring massive bone grafting and prolonged, unstable fixation. Finally, the cosmetic appearance of the leg would be highly deformed, presenting a severe step off contour that is unacceptable to the patient.
Strategies for Multilevel Osteotomy Correction
To properly address a multiapical deformity, the surgeon must abandon the single intersection theory and embrace multilevel deformity analysis. This requires identifying the true anatomical axes of the intermediate bone segments.
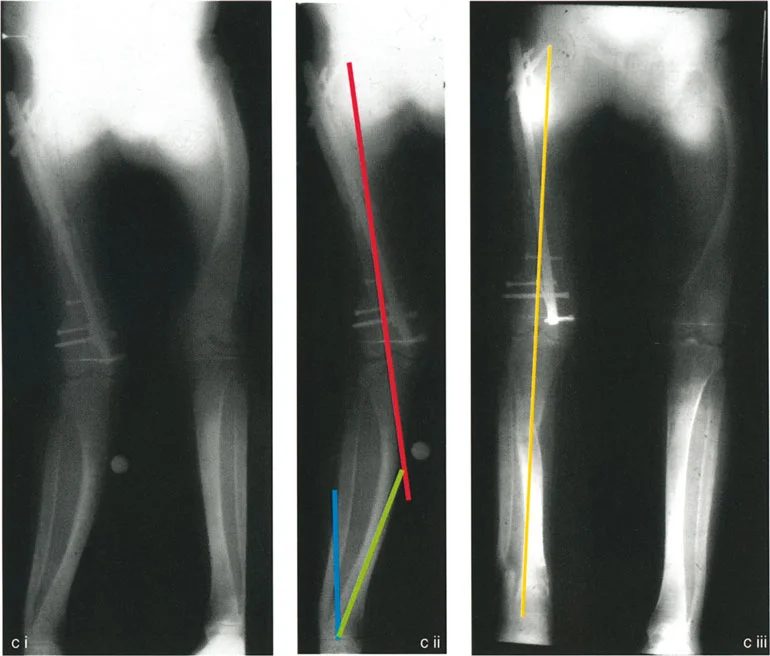
Identifying Multiple Centers of Rotation of Angulation
The correct approach to the sweeping bow or compensatory deformity involves breaking the bone down into its constituent straight segments.
- Draw the Proximal Mechanical Axis based on the normal MPTA.
- Draw the Distal Mechanical Axis based on the normal LDTA.
- Instead of forcing these two lines to intersect, draw the anatomical axis of the middle segment of the diaphysis.
- The Proximal Mechanical Axis will intersect the middle anatomical axis at the Proximal Center of Rotation of Angulation.
- The Distal Mechanical Axis will intersect the middle anatomical axis at the Distal Center of Rotation of Angulation.
By identifying two distinct Centers of Rotation of Angulation, the surgeon has accurately mapped the true nature of the multiapical deformity. The magnitude of the proximal deformity and the magnitude of the distal deformity can now be measured independently.
Executing the Double Level Osteotomy
Once the two Centers of Rotation of Angulation are identified, the surgical plan shifts to a double level osteotomy. The surgeon will perform one osteotomy at or near the proximal Center of Rotation of Angulation, and a second osteotomy at or near the distal Center of Rotation of Angulation.
During the procedure, the proximal osteotomy is executed to correct the proximal angular deformity, bringing the middle segment into alignment with the proximal joint. Subsequently, the distal osteotomy is executed to correct the distal angular deformity, bringing the distal joint into alignment with the middle segment.
Postoperative Alignment and Joint Preservation
The results of a meticulously planned double level osteotomy are profound. By correcting each apex of deformity independently, the surgeon achieves two critical goals simultaneously.
First, the overall Mechanical Axis Deviation is restored to neutral, ensuring that the weight bearing line passes through the center of the knee and the ankle. Second, and most importantly, the joint orientation angles at both the knee and the ankle remain perfectly normal. The MPTA is preserved at 87 degrees, and the LDTA is preserved at 89 degrees.
The ankle joint is not uncovered into severe varus or valgus. The articular cartilage of the tibial plafond remains parallel to the ground during stance phase, ensuring even load distribution, normal biomechanics, and the prevention of early onset osteoarthritis.
Advanced Considerations in Frontal Plane Correction
Executing complex multiapical deformity corrections requires more than just geometric planning. The orthopedic surgeon must manage the biological and mechanical realities of the human limb.
Soft Tissue Management and Neurovascular Structures
Deformity correction is as much a soft tissue procedure as it is a bony procedure. When correcting severe valgus deformities, particularly in the proximal tibia, the common peroneal nerve is at extreme risk of traction injury.
As the lateral side of the tibia is lengthened or the medial side is compressed, the peroneal nerve stretches around the fibular neck. Surgeons must have a low threshold for performing a prophylactic peroneal nerve decompression. This involves releasing the fascial bands of the peroneus longus muscle to allow the nerve to glide freely during the correction.
Furthermore, acute corrections of large magnitude deformities increase the pressure within the fascial compartments of the leg. Prophylactic anterior and lateral compartment fasciotomies should be considered to prevent acute compartment syndrome, a devastating complication that can lead to muscle necrosis and permanent limb dysfunction.
Fixation Choices for Multiapical Deformities
The choice of fixation depends heavily on whether the surgeon chooses an acute correction or a gradual correction.
Acute Correction with Internal Fixation
If the deformities are highly mobile once the osteotomies are made, and the soft tissue envelope allows for immediate realignment without excessive tension, acute correction can be achieved using rigid internal fixation. Locking plates or intramedullary nails can be utilized. Intramedullary nailing of double level osteotomies is technically demanding but offers excellent load sharing biomechanics. Blocking screws, or Poller screws, are essential adjuncts when using intramedullary nails to guide the nail trajectory and prevent malalignment during insertion.
Gradual Correction with External Fixation
For severe, long standing multiapical deformities, or when soft tissue compliance is poor, gradual correction using a circular external fixator is the gold standard. The Ilizarov method, modernized by hexapod technology such as the Taylor Spatial Frame, allows the surgeon to apply Paley principles through a computer generated strut adjustment schedule.
Gradual correction via distraction osteogenesis mitigates the risk of acute neurovascular stretch injuries. It also allows for postoperative fine tuning. If the initial correction leaves a residual 3 degree malalignment, the surgeon simply adjusts the hexapod struts in the clinic, achieving perfect alignment without returning the patient to the operating room.
Managing the Fibula in Tibial Deformity Correction
The fibula must never be ignored during tibial deformity correction. The fibula acts as a lateral strut and will physically block any attempt to correct a severe tibial deformity if it is not addressed.
For proximal tibial corrections, a proximal tibiofibular joint release or a fibular osteotomy at the junction of the middle and distal thirds is required. For multiapical corrections involving the distal tibia, a second fibular osteotomy may be necessary to allow the distal segment to move freely. Care must be taken to stabilize the distal tibiofibular syndesmosis to prevent ankle mortise widening during the correction process.
Clinical Pearls for Deformity Correction Mastery
To synthesize these complex biomechanical and surgical concepts, orthopedic surgeons should internalize the following high yield clinical pearls.
- Never Eyeball Deformity: Always utilize full length standing radiographs and perform rigorous mathematical planning using the Paley Malalignment and Malorientation tests.
- Beware the Sweeping Bow: A long, sweeping deformity almost always hides multiple apices. Forcing a single Center of Rotation of Angulation will lead to joint malorientation.
- The Ankle is Unforgiving: While the knee can tolerate slight malalignment, the ankle joint is highly constrained. Altering the LDTA beyond normal limits guarantees rapid cartilage destruction.
- Respect Paley Osteotomy Rules: If you must cut away from the Center of Rotation of Angulation due to poor bone stock, you must calculate and execute the required translation to maintain a collinear mechanical axis.
- Translation has Biological Limits: While mathematical translation can solve axis deviations, massive clinical translation leads to skin necrosis, nonunion, and unacceptable cosmetic defects. Multilevel osteotomies are the biological solution to mathematical limitations.
- Protect the Peroneal Nerve: Valgus correction stretches the lateral structures. Always consider peroneal nerve decompression and compartment releases in acute corrections exceeding 10 to 15 degrees.
- Hexapod is the Ultimate Salvage: When multiapical deformities are too complex for acute internal fixation, circular hexapod frames offer the safety of gradual correction and the luxury of postoperative adjustability.
Mastering frontal plane realignment requires dedication to geometric principles, respect for soft tissue biology, and a refusal to compromise on joint orientation. By applying the multiapical analysis techniques outlined in this guide, orthopedic surgeons can reliably restore function, eliminate pain, and preserve the native joints of their patients for decades to come.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like