Surgical Management of the Spastic Upper Extremity: Brachioradialis Rerouting and Wrist Flexion Deformities
Key Takeaway
Brachioradialis rerouting is a powerful surgical intervention designed to correct severe supination deformities and restore forearm balance in spastic paralysis. By meticulously mobilizing the brachioradialis and rerouting it through the interosseous membrane, surgeons can convert its deforming force into a functional pronator. This guide details the operative steps, Zancolli classification for wrist flexion deformities, and evidence-based postoperative protocols for optimal functional recovery.
INTRODUCTION TO SPASTIC UPPER EXTREMITY DEFORMITIES
The management of the spastic upper extremity—frequently seen in patients with cerebral palsy, traumatic brain injury, or post-stroke hemiplegia—presents a formidable reconstructive challenge to the orthopaedic surgeon. The overarching goals of surgical intervention are to improve functional capacity (such as grasp and release), facilitate activities of daily living (ADLs), and enhance hygiene and cosmesis in non-functional limbs.
Among the most debilitating presentations are severe rotational deformities of the forearm (pronation or supination contractures) and flexion deformities of the wrist and fingers. These contractures are often accompanied by elbow flexion and a thumb-in-palm deformity, creating a complex cascade of biomechanical imbalances. This comprehensive guide details the advanced surgical techniques required to address these pathologies, specifically focusing on the brachioradialis rerouting procedure described by Ozkan et al., and the systematic management of wrist and finger flexion deformities based on the Zancolli classification.
BRACHIORADIALIS REROUTING
The brachioradialis is a unique muscle; while primarily an elbow flexor, its line of pull allows it to act as a supinator when the forearm is pronated, and a pronator when the forearm is supinated. In the spastic upper extremity, an overactive brachioradialis can contribute to severe, rigid supination deformities. The brachioradialis rerouting procedure, popularized by Ozkan et al., aims to dynamically correct this imbalance by altering the muscle's biomechanical vector, effectively converting it into a consistent pronator.
Indications and Preoperative Planning
Brachioradialis rerouting is indicated in patients with a fixed or dynamic supination deformity of the forearm where the brachioradialis is identified as a primary deforming force. Preoperative clinical evaluation must assess passive range of motion to ensure the distal radioulnar joint (DRUJ) and interosseous membrane are not rigidly contracted. If fixed osseous or severe capsular contractures exist, soft tissue rerouting alone will fail, and osteotomies or joint releases must be considered.
Surgical Anatomy and Biomechanics
To successfully reroute the brachioradialis, the surgeon must navigate the complex neurovascular anatomy of the radial forearm. The superficial branch of the radial nerve (SBRN) and the radial artery run in close proximity to the deep surface of the brachioradialis. The rerouting relies on passing the tendon through the interosseous space, changing its insertion vector from the radial styloid (a supinating force in this context) to a dorsal-to-palmar pull that actively pronates the radius around the intact ulna.
Step-by-Step Surgical Technique (Ozkan et al.)
🔪 Surgical Pearl: Incision Planning
Make a generous longitudinal incision on the radial aspect of the forearm. This provides extensile access to the brachioradialis, pronator teres, and pronator quadratus muscles. If concomitant procedures—such as fractional flexor tendon lengthening—are planned, utilize a curvilinear incision on the palmar surface of the forearm to allow comprehensive access to the flexor compartment.
1. Exposure and Deep Dissection
Develop full-thickness skin flaps and retract them carefully to avoid devascularizing the subcutaneous tissues. Identify the pronator quadratus muscle in the distal forearm. Using monopolar diathermy, release the pronator quadratus by cutting directly through its muscle belly. This eliminates a secondary deforming force and exposes the distal interosseous space.
2. Pronator Teres Lengthening
Isolate the pronator teres tendon at its insertion on the lateral convexity of the radius. Divide the tendon in a Z-fashion to allow for controlled lengthening.
Suturing: Reapproximate the tendon ends with the forearm held in a neutral rotation position, ensuring there is absolutely no tension within the tendon construct.
🚨 Surgical Warning: Pronator Teres Tensioning
It is crucial not to overlengthen the pronator teres tendon. Overlengthening will completely ablate pronator function, potentially leading to a devastating iatrogenic supination deformity.
3. Neurovascular Protection
Identify the superficial branch of the radial nerve and the radial artery in the distal forearm. Gently mobilize and retract these structures to protect them during the subsequent tendon transfer and interosseous window creation.
4. Brachioradialis Mobilization
Prepare the brachioradialis tendon and muscle belly for transfer. The distal attachment on the radial styloid must be preserved initially to maintain tension for dissection.
Fascial Release: It is imperative that the brachioradialis muscle is completely freed from all its fascial attachments proximally. Failure to perform a radical fascial release will result in insufficient muscle excursion, rendering the transfer functionally useless. Preserve the proximal neurovascular pedicle (branches from the radial nerve and radial recurrent artery) entering the proximal third of the muscle belly.
5. Tendon Division and Interosseous Window Creation
Divide the brachioradialis tendon using a long Z-plasty technique. This provides the maximal tendon length required for the rerouting trajectory.
Next, create a generous window in the interosseous membrane just proximal to the released pronator quadratus muscle. Ensure the window is large enough to prevent adhesions or tethering of the transferred tendon.
6. Rerouting and Fixation
Pass the distal tendon end of the brachioradialis through the created interosseous window in a dorsal to palmar direction.
Arterial Protection: Retract the radial artery and carefully pass the tendon deep to the artery to avoid any risk of vascular compression or occlusion during muscle contraction.
Weave: Suture the proximal and distal tendon ends to each other using a robust Pulvertaft weave technique.
7. Final Tensioning and Closure
Perform the final tendon reattachment with the forearm held strictly in neutral rotation. There should be no tension on the tendon ends at this resting posture. Close the skin with absorbable subcutaneous and subcuticular sutures.
Postoperative Care Protocol
The success of a tendon transfer relies heavily on meticulous postoperative rehabilitation.
* Immediate Post-op: Apply an above-elbow plaster cast in the operating room. The elbow must be immobilized in 90 degrees of flexion, with the forearm in neutral rotation. If additional procedures (e.g., wrist/finger flexor lengthening) were performed, extend the cast to include the wrist and fingers in the corrected position.
* First 48 Hours: The hand is strictly elevated to minimize edema. Peripheral circulation and capillary refill must be closely monitored, especially given the proximity of the transfer to the radial artery.
* Weeks 0-4: The patient remains in the rigid above-elbow cast to allow for primary tendon healing at the Pulvertaft weave site.
* Weeks 4-12: The cast is removed and replaced with a custom thermoplastic splint. This splint is removed periodically throughout the day for active and active-assisted physical therapy, focusing on cortical re-education of the transferred muscle.
* Weeks 12-16: The daytime splint is discontinued, allowing the patient to integrate the extremity into activities of daily living (ADLs). A nighttime resting splint is maintained for an additional 4 weeks to prevent contracture recurrence.
FLEXION DEFORMITIES OF THE WRIST AND FINGERS
Flexion deformities of the wrist and fingers are the most ubiquitous upper extremity contractures encountered in spastic paralysis. These deformities severely impair hand function, rendering grasp and release mechanisms ineffective, and are classically accompanied by forearm pronation, elbow flexion, and a thumb-in-palm deformity.
Surgical decision-making is dictated by the severity of the contracture, the presence of voluntary motor control, and the phase of muscle activity. The Zancolli classification remains the gold standard for categorizing these deformities and guiding operative interventions.
Zancolli Classification of Spastic Flexion Deformities
Zancolli et al. classified spastic flexion deformities of the wrist and hand into three distinct patterns based on the patient's ability to actively extend the fingers and wrist.
Pattern 1: Mild Deformity
Clinical Presentation: The patient can actively extend the fingers with the wrist held in less than 20 degrees of flexion. Extension of the wrist is impossible when the fingers are in full extension due to flexor tightness.
Functional Status: This is a relatively mild deformity. Both grasp and release functions are preserved, though mechanically disadvantaged.
Surgical Management:
The goal is to reduce the spastic flexor tone without sacrificing grip strength.
* Flexor Carpi Ulnaris (FCU) Tenotomy: Often considered to eliminate the primary deforming force at the wrist.
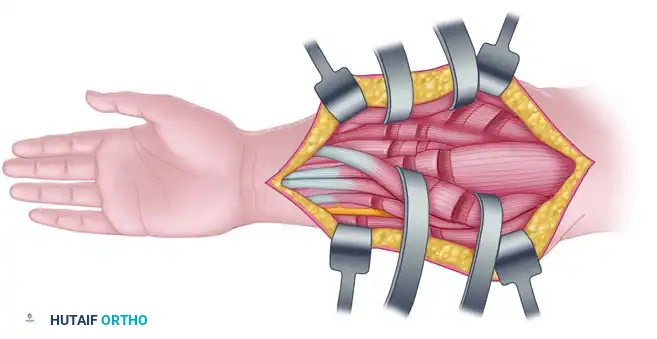
* Fractional Lengthening: Lengthening of the finger flexors is preferably performed via tenotomy at the musculotendinous junction (fractional lengthening). This allows for selective, controlled lengthening of the spastic units while maintaining the continuity of the muscle-tendon unit.
Figure 72-6: Fractional lengthening of the flexor carpi radialis muscle and finger flexors. Note the careful isolation and protection of the ulnar nerve during the approach to the deep flexor compartment.
- Flexor Slide: In cases of more diffuse flexor tightness, a proximal flexor muscle slide (e.g., Page-Scaglietti procedure) may be selected to advance the flexor origin distally, thereby relatively lengthening the entire flexor mass.
Pattern 2: Moderate to Severe Deformity
Clinical Presentation: Active finger extension is possible only when the wrist is flexed to more than 20 degrees (the tenodesis effect is required to achieve finger extension).
This pattern is subdivided based on the presence of active wrist extension:
* Pattern 2a: The patient has voluntary active wrist extension when the fingers are flexed. This indicates that the wrist extensors (ECRL, ECRB, ECU) are active and under voluntary control, and the finger flexors are not overwhelmingly spastic.
* Pattern 2b: The patient is completely unable to extend the wrist, even with the fingers in full flexion. This indicates that the wrist extensors are paralyzed or profoundly weak, requiring surgical augmentation to restore functional wrist extension.
Surgical Management for Pattern 2:
Management requires a combination of flexor lengthening and tendon transfers to augment extension.
* Tendon Transfers: The classic transfer for Pattern 2b is the transfer of the Flexor Carpi Ulnaris (FCU) to the Extensor Carpi Radialis Brevis (ECRB) (Green's transfer). This powerful transfer removes a deforming wrist flexor and converts it into a wrist extensor, simultaneously improving supination and facilitating finger flexion (grasp) through the tenodesis effect.
* Release Augmentation: If the primary functional deficit is weakness in finger extension (release), the FCU can alternatively be transferred into the Extensor Digitorum Communis (EDC).
* Alternative Transfers: Another robust alternative involves fractionally lengthening the FCU and Flexor Carpi Radialis (FCR) to reduce volar tone, followed by transferring the Extensor Carpi Ulnaris (ECU) into the ECRB to centralize and augment wrist extension power.
💡 Clinical Pearl: The Role of Electromyography (EMG)
Preoperative dynamic electromyography (EMG) is highly valuable in Pattern 2 deformities. It determines the exact phase in which the potential donor muscle (e.g., FCU) is active—whether during the grasp phase or the release phase. Transferring a muscle that is naturally active in the desired phase of the target function significantly enhances postoperative cortical integration and functional outcomes.
Pattern 3: Severe, Non-Functional Deformity
Clinical Presentation: The patient exhibits severe, rigid flexion deformities and is completely unable to extend the fingers or wrist actively, even when starting from a position of maximal passive wrist flexion.
Functional Status: Hand sensibility is usually poor, and voluntary motor control is negligible. The limb is non-functional.
Surgical Management:
In Pattern 3, surgery will not restore dynamic function. The primary goals are to improve hygiene, prevent skin maceration in the palm, alleviate pain, and improve cosmesis.
* Soft Tissue Salvage: Radical tenotomy of the wrist flexors combined with a sublimis-to-profundus (STP) transfer, as described by Braun and Vice, is highly effective. This involves suturing the distal stumps of the flexor digitorum profundus (FDP) to the proximal stumps of the flexor digitorum superficialis (FDS), effectively lengthening the flexor apparatus massively while maintaining a passive tether to prevent hyperextension.
* Bony Procedures: In the most severe, rigid deformities, soft tissue procedures alone are inadequate. Wrist arthrodesis (fusion) in a neutral or slightly extended position provides a stable, cosmetic correction. If severe carpal contractures are present, a proximal row carpectomy (PRC) may be performed concomitantly to decompress the joint and allow for tension-free correction of the deformity prior to fusion.
Summary of Surgical Strategy
The surgical correction of the spastic upper extremity demands a profound understanding of altered biomechanics and neuroanatomy. Whether performing a complex brachioradialis rerouting to restore forearm rotation or executing a staged tendon transfer based on the Zancolli classification, the surgeon must balance the release of spastic deforming forces with the augmentation of weak antagonists. Strict adherence to meticulous surgical technique, precise tensioning, and rigorous postoperative rehabilitation are the cornerstones of achieving meaningful functional improvement in this challenging patient population.
📚 Medical References
- Brachioradialis rerouting for the restoration of active supination and correction of forearm pronation deformity in cerebral palsy, J Hand Surg 29B:265, 2004.
- Page CM: An operation for the relief of fl exion-contracture in the forearm, J Bone Joint Surg 21:233, 1923.
- Rayan GM, Young BT: Arthrodesis of the spastic wrist, J Hand Surg 24A:944, 1999.
- Sakellarides HT, Mital MA, Lenzi WD: Treatment of
You Might Also Like