Osteochondral Ridges of the Talus and Tibia: Anterior and Posterior Impingement Syndromes
Key Takeaway
Ankle impingement syndromes, encompassing both anterior and posterior variants, present significant challenges in athletic populations. Characterized by osteochondral ridges and hypertrophic soft tissue, these conditions restrict terminal range of motion and cause debilitating pain. This guide details the pathoanatomy, Scranton and McDermott classification, and advanced arthroscopic management techniques—including osteophyte resection and synovectomy—to restore joint kinematics and facilitate return to elite athletic function.
Introduction and Historical Context
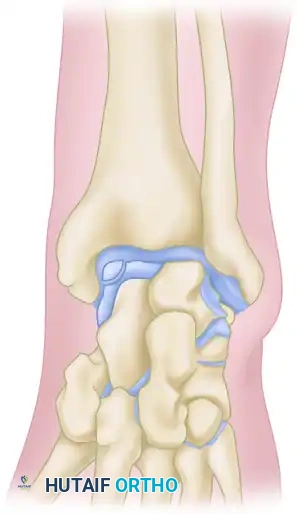
In 1957, O’Donoghue formally directed the orthopedic community's attention to a previously underreported cause of chronic ankle disability: the formation of osteochondral ridges, or exostoses. These bony proliferations typically develop just proximal to the anterior lip of the distal articular surface of the tibia and on the corresponding opposing area of the dorsal surface of the talar neck.
Predominantly observed in athletic populations—particularly footballers, dancers, and runners—these ridges are primarily driven by repetitive biomechanical stress. According to O’Donoghue, the primary etiology is direct mechanical injury sustained during forceful, extreme dorsiflexion of the foot, wherein the neck of the talus is violently thrust against the anterior tibial plafond. Repeated minor microtraumas precipitate a hypertrophic bone response, causing these ridges to enlarge over time. As the exostoses grow, the threshold for collision between the talus and tibia decreases, creating a self-perpetuating cycle of impingement, cartilage abrasion, and further osteophyte formation. These ridges may manifest in isolation on the tibia or the talus, but frequently develop concomitantly on both articular surfaces.
Pathoanatomy and Biomechanics
Anterior Impingement Syndrome
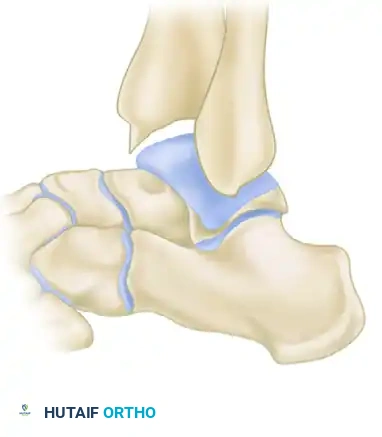
Anterior impingement syndrome is classically an overuse injury of the dorsiflexors, compounded by repetitive microtrauma. The mechanical abutment of the anterior tibial margin against the talar neck leads to the formation of "kissing lesions" or osteophytes.
Clinical Pearl: While historically attributed solely to direct impaction (the "bone-on-bone" theory), modern biomechanical studies suggest that recurrent capsular traction during forced plantar flexion also plays a critical role in the development of anterior tibial osteophytes. Thus, the etiology is likely a combination of direct impaction during dorsiflexion and capsular avulsion during plantar flexion.
Posterior Impingement Syndrome
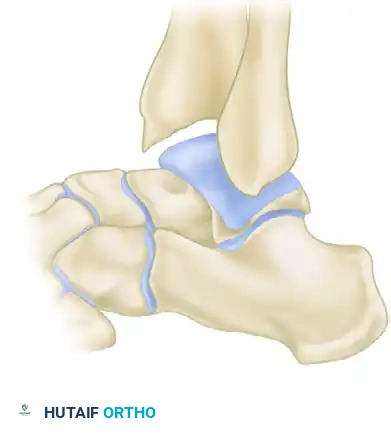
Conversely, posterior impingement syndrome—often termed posterior compression syndrome or os trigonum syndrome—afflicts athletes who repeatedly subject their ankles to extreme plantar flexion (e.g., ballet dancers en pointe, fast bowlers in cricket). The posterior talar process, or an unfused os trigonum, becomes mechanically compressed between the posterior lip of the tibial plafond and the superior surface of the calcaneus, leading to chronic inflammation, bony hypertrophy, and posterior capsulitis.
Soft Tissue Impingement and Synovitis
Impingement is not exclusively a bony phenomenon. Chronic anterolateral ankle pain is frequently driven by soft tissue pathology. Following inversion ankle sprains, chronic synovitis, or nondisplaced fractures, hypertrophic scar tissue can accumulate in the anterolateral gutter.
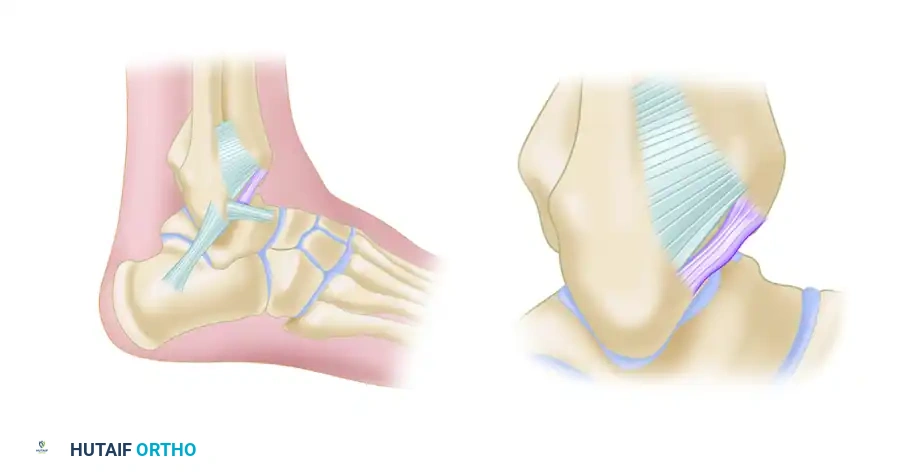
Bassett et al. identified that thickened distal fascicles of the anterior inferior tibiofibular ligament (AITFL) can act as a primary source of impingement. This accessory fascicle, present in the majority of human ankles, runs parallel and distal to the primary AITFL, separated by a fibrofatty septum. During dorsiflexion, this thickened band can impinge on the anterolateral aspect of the talus, causing localized chondromalacia and severe pain.
Clinical Evaluation and Imaging
Clinical Presentation
Patients typically present with a chronic, deep aching pain in the ankle that is acutely exacerbated by terminal ranges of motion—specifically, strong dorsiflexion in anterior impingement, and forced plantar flexion in posterior impingement.
Physical examination usually reveals:
* Palpable tenderness along the anterolateral or anteromedial joint line.
* A positive impingement sign: Pain elicited when the examiner forcefully dorsiflexes the ankle while applying digital pressure over the anterior joint line.
* Mild to moderate joint effusion, particularly after aggravating activities.
Radiographic Assessment
Standard weight-bearing radiographs (anteroposterior, lateral, and mortise views) are mandatory. The lateral view is particularly diagnostic for anterior impingement, revealing a loss of the normal rounded contour of the anterior distal tibia, replaced by a sharp ridge or a distinct anteriorly projecting bony spur. Corresponding dorsal talar spurs may also be visible.


Advanced imaging, such as MRI or CT arthrography, is highly valuable for identifying radiographically occult soft tissue impingement. CT arthrography provides excellent visualization of nodular formations in the lateral groove (often resembling discoid meniscal lesions) and abundant fibrous reactions. Furthermore, MRI can identify "tram track" lesions—parallel linear chondral defects on the talar dome caused by the abrasive action of tibial osteophytes—which aid in pinpointing the exact location of the impingement.
Scranton and McDermott Classification
Scranton and McDermott developed a widely utilized radiographic classification system for anterior ankle spurs, which correlates directly with the degree of joint involvement, treatment complexity, and prognostic recovery:
-
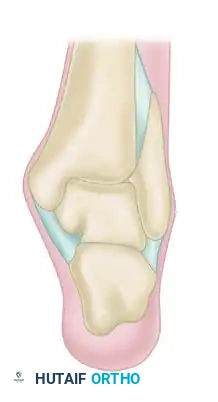
Grade I (Synovial Impingement): Radiographs demonstrate an inflammatory reaction with minor tibial spurs measuring up to 3 mm.
-
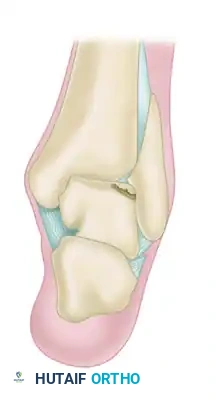
Grade II (Osteochondral Reaction Exostosis): Radiographs show tibial spurs larger than 3 mm. No corresponding talar spur is present.
-
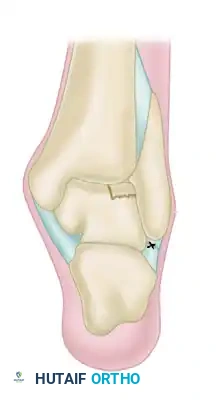
Grade III (Severe Exostosis): A secondary spur is noted on the dorsum of the talus, often accompanied by fragmentation of the osteophytes (kissing lesions).

-
Grade IV (Pantalocrural Osteoarthrotic Destruction): Radiographs suggest diffuse degenerative osteoarthritic changes extending medially, laterally, or posteriorly, indicating global joint deterioration rather than isolated impingement.

Conservative Management
Initial management for both anterior and posterior overuse syndromes should be strictly non-operative for a minimum of 3 to 6 months. The protocol includes:
1. Activity Modification: Curtailment of the specific aggravating activities (e.g., restricting hill running or deep squats).
2. Pharmacotherapy: Scheduled nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce synovial inflammation.
3. Immobilization: Temporary use of a controlled ankle motion (CAM) boot or taping to restrict terminal ranges of motion.
4. Physical Therapy: Heel lifts (for anterior impingement to maintain slight plantar flexion) and targeted strengthening of the dynamic ankle stabilizers.
Surgical Management: Arthroscopic Excision
When conservative measures fail to relieve debilitating symptoms, surgical intervention is indicated. O’Donoghue originally recommended open excision; however, modern techniques heavily favor arthroscopic resection due to decreased morbidity, faster rehabilitation, and excellent visualization of the joint space.
Ogilvie-Harris et al. demonstrated high success rates with arthroscopic resection in patients who failed 6 months of conservative care. Postoperatively, patients exhibited significant pain relief, decreased swelling, and increased dorsiflexion. Notably, plantar flexion is rarely improved by anterior debridement.
Surgical Warning: Patients must be explicitly counseled preoperatively regarding the risk of postoperative numbness over the anterior dorsum of the foot, secondary to neuropraxia or injury to the superficial peroneal nerve during portal placement.
Surgical Technique: Arthroscopic Resection (Ogilvie-Harris Protocol)
1. Anesthesia and Positioning
* Administer general or regional anesthesia.
* Place the patient supine with the operative leg secured in a thigh holder.
* Apply and inflate a pneumatic thigh tourniquet to ensure a bloodless field.
2. Joint Distention and Portal Placement
* Identify the anterior tibial tendon. Insert an 18-gauge needle just medial to this tendon and distend the ankle joint with 15 to 20 mL of sterile normal saline.
* Anteromedial Portal: Make a small longitudinal incision through the skin only, just medial to the anterior tibial tendon. Use a hemostat for blunt dissection down to the capsule to protect the saphenous vein and nerve. Insert a 2.7-mm or 4.0-mm, 30-degree arthroscope.
* Crucial Step: Pass the arthroscope carefully across the anterior aspect of the joint. Do not drag the trocar across the convex dome of the talus to avoid iatrogenic cartilage scuffing.
* Anterolateral Portal: Establish this portal under direct intra-articular visualization. Make the incision just lateral to the peroneus tertius tendon.
* Anatomic Hazard: The superficial peroneal nerve branches cross this region. Transillumination of the skin with the arthroscope can help identify and avoid these neurovascular structures.
3. Joint Distraction and Diagnostic Sweep
* Perform a comprehensive diagnostic sweep of the joint.
* Apply a noninvasive ankle distraction strap to open the joint space.
* Technical Note: While distraction is excellent for viewing the central compartment, it tightens the anterior capsule. To identify and gain access to large anterior osteophytes (especially on the talar neck), the distraction may need to be temporarily released.

4. Soft Tissue Debridement
* Introduce a pressure irrigation system.
* Utilize a 3.5-mm full-radius resector through the anterolateral portal to clear the hypertrophic anterior synovium. This step is critical to unmask the underlying anterior tibial and superior talar bony spurs.
* If a thickened distal fascicle of the AITFL (Bassett's ligament) is identified impinging on the talus during dynamic dorsiflexion, resect it completely. This does not compromise the structural stability of the syndesmosis.
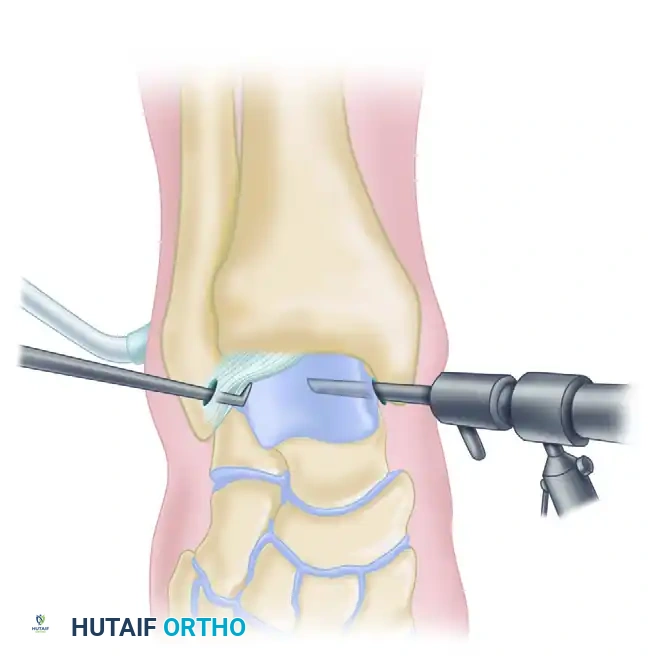
5. Osteophyte Resection
* Introduce a 3.0-mm or 4.0-mm arthroscopic burr.
* Systematically resect the tibial osteophytes back to the level of the normal native cartilage.
* The Davis Modification: To prevent inadvertent damage to the intact articular cartilage, Davis described creating a "trough" with the burr approximately 1 mm proximal and parallel to the anterior edge of the tibia. This trough is taken down to subchondral bone. An arthroscopic bone-biter or osteotome is then used to fracture and remove the isolated bony spur. This provides superior control compared to attempting to gain purchase on the hard, smooth surface of the spur with a shaver.
* Smooth the resected tibial surface with the full-radius resector.
* Repeat the identical procedure for any kissing lesions on the superior neck of the talus.
6. Final Inspection and Closure
* Re-apply manual distraction in mid-plantar flexion to pass the arthroscope gently over the dome of the talus, ensuring no loose bodies or missed chondral flaps remain.
* Thoroughly irrigate the joint to remove all bone debris.
* Inject 20 mL of 0.25% bupivacaine intra-articularly for postoperative analgesia.
* Close the portals with non-absorbable sutures (e.g., 4-0 nylon) and apply a sterile, bulky compressive dressing.
Osteochondritis Dissecans (OCD) of the Talus
During the arthroscopic evaluation of impingement syndromes, the surgeon must meticulously inspect the talar dome for concurrent Osteochondritis Dissecans (OCD) lesions. These lesions are focal areas of subchondral bone necrosis and secondary cartilage damage, frequently resulting from the same traumatic inversion mechanisms that cause soft tissue impingement.
Morphological Characteristics
- Lateral Lesions: Typically traumatic in origin. They characteristically appear shallow, horizontal, and wafer-shaped. They are frequently elevated or completely detached, acting as loose bodies within the lateral gutter.
- Medial Lesions: Often insidious or microtraumatic in origin. They are characteristically deeper and cup-shaped. Although they may appear detached on imaging, they most frequently sit securely within their crater and are less likely to displace.
Staging of Talar OCD Lesions
The progression of OCD lesions is classically categorized into four stages, which dictate the necessity for drilling, fixation, or excision:
-
Normal: Intact cartilage with underlying subchondral stress, often invisible on standard radiographs but detectable on MRI.
-
Stage I: Localized subchondral compression fracture with intact overlying articular cartilage.

-
Stage II: Partially detached osteochondral fragment. A clear radiolucent line begins to separate the fragment from the native bone bed.
-
Stage III: Completely detached osteochondral fragment that remains non-displaced within its native crater.

-
Stage IV: Completely detached and displaced osteochondral fragment, resulting in a loose body within the joint space.
Management of these lesions during impingement surgery ranges from simple debridement and microfracture (for small, symptomatic Stage III/IV lesions) to retrograde drilling or internal fixation for larger, salvageable fragments.
Postoperative Care and Rehabilitation
The success of arthroscopic debridement for impingement syndromes relies heavily on aggressive, early postoperative rehabilitation to prevent the reformation of intra-articular adhesions.
- Phase I (Days 1-7): Immediate weight-bearing as tolerated in a supportive shoe or CAM boot is encouraged. The primary goals are edema control (ice packs, elevation) and the initiation of active and passive range-of-motion (ROM) exercises to prevent capsular contracture.
- Phase II (Weeks 1-4): A vigorous rehabilitation program commences. Emphasis is placed on restoring terminal dorsiflexion. A tilt board or biomechanical ankle platform system (BAPS) is introduced for proprioceptive training. Progressive resistance exercises are utilized to strengthen the anterior (tibialis anterior) and posterior (gastroc-soleus complex) musculature.
- Phase III (Weeks 4-6): Transition to sport-specific dynamic movements.
- Return to Play (6+ Weeks): Sports activities can be resumed in a gradual, protected fashion. It is imperative that the athlete utilizes footwear adequate for their specific biomechanical needs (e.g., properly fitted running shoes with appropriate heel drop) to mitigate the recurrence of extreme dorsiflexion impaction.
By adhering to precise arthroscopic techniques and structured rehabilitation, surgeons can reliably restore joint kinematics, alleviate chronic pain, and return athletes to their pre-injury levels of performance.
You Might Also Like


