Mastering the Spine Posterior Approach: Surgical Essentials
Key Takeaway
For anyone wondering about Mastering the Spine Posterior Approach: Surgical Essentials, The spine posterior approach is the most common surgical access to the lumbar spine, typically through the midline. It provides direct access to the cauda equina, intervertebral discs, and posterior elements like spinous processes and facet joints. This approach is used for procedures such as herniated disc excision, nerve root exploration, spinal fusion, and tumor removal.
Mastering the Spine Posterior Approach Surgical Essentials
Introduction and Epidemiology
The posterior approach represents the cornerstone of surgical intervention for a vast spectrum of lumbar spine pathologies. Its ubiquity stems from its direct anatomical access to critical posterior spinal elements, including the spinous processes, laminae, facet joints, and pedicles, as well as indirect access to the intervertebral discs and the contents of the spinal canal, particularly the cauda equina and traversing nerve roots. This surgical corridor facilitates a diverse array of procedures, making it the most frequently employed approach in lumbar spinal surgery.
Historically, the posterior midline approach evolved from early laminectomy procedures for decompression, progressing to contemporary techniques incorporating sophisticated instrumentation for stabilization and fusion. Early pioneers like Albee and Hibbs popularized posterolateral fusion techniques in the early 20th century. The advent of pedicle screw fixation in the latter half of the century revolutionized spinal stabilization, providing robust segmental fixation. Its prevalence in modern practice is underscored by the high incidence of degenerative spinal conditions, such as lumbar disc herniation, spinal stenosis, and degenerative spondylolisthesis, which are primary indications for posterior surgical management. Traumatic injuries, spinal deformities, and oncologic conditions further broaden the utility of this fundamental approach. The ongoing advancements in surgical techniques, including muscle-sparing and minimally invasive variations, continue to refine the posterior approach, emphasizing its enduring relevance in orthopedic spine surgery. The global burden of low back pain and its associated disability drives the continuous demand for effective surgical solutions, often delivered via the posterior corridor.
Surgical Anatomy and Biomechanics
A thorough understanding of the anatomical landscape and biomechanical principles governing the lumbar spine is paramount for safe and effective posterior surgical intervention.
Bony Anatomy
The lumbar vertebral column consists of five vertebrae, characterized by large, kidney-shaped vertebral bodies, robust pedicles, and broad laminae. Key posterior elements include:
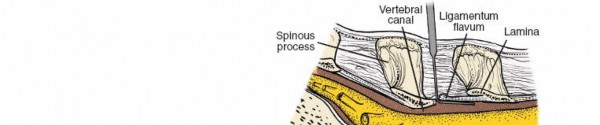
* Spinous processes: These project posteriorly and inferiorly, serving as crucial landmarks for midline incision and initial surgical orientation. Their morphology varies, with L5 being typically the smallest and L3/L4 often the most prominent. They provide attachment for supraspinous and interspinous ligaments and several muscle groups.
* Laminae: Broad, flat plates forming the posterior wall of the vertebral canal, connecting the pedicles to the spinous process. Laminectomy or laminotomy involves resection of these structures for decompression.
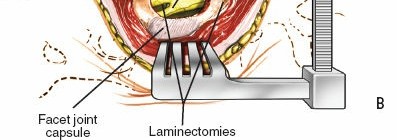
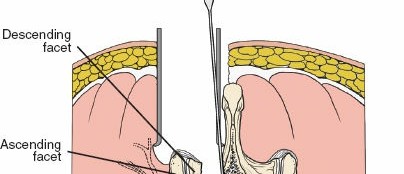
* Facet joints (zygapophyseal joints): Synovial joints formed by the superior and inferior articular processes. Their orientation in the lumbar spine is primarily sagittal, allowing for flexion and extension but limiting rotation. Medial facetectomy is often performed for nerve root decompression, while complete facetectomy is sometimes necessary for interbody cage placement. These joints are a significant source of chronic low back pain and targets for fusion.
* Pedicles: Short, stout processes extending posteriorly from the vertebral body, connecting to the lamina and transverse process. They are the primary conduits for pedicle screw placement, providing excellent biomechanical fixation due to their cortical shell and cancellous core. The pedicle wall offers significant resistance to screw pullout.
* Transverse processes: Project laterally from the junction of the pedicle and lamina, providing attachment points for the erector spinae muscles and serving as targets for posterolateral fusion.
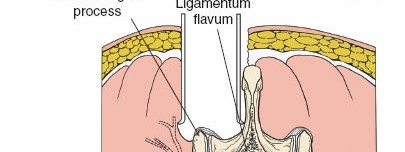
Ligamentous Anatomy
The stability of the posterior lumbar spine is significantly reinforced by a complex array of ligaments:
* Supraspinous ligament: Connects the tips of the spinous processes, resisting flexion.
* Interspinous ligaments: Connect adjacent spinous processes, also resisting flexion. They are less robust than the supraspinous ligament.
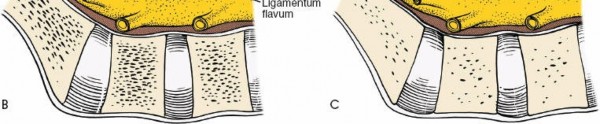
* Ligamentum flavum: A highly elastic ligament connecting adjacent laminae. It forms the posterior wall of the spinal canal, protecting the dura mater and nerve roots. Hypertrophy of the ligamentum flavum is a common cause of spinal stenosis. Careful dissection of this ligament is essential during laminectomy to avoid dural injury.
* Intertransverse ligaments: Connect adjacent transverse processes, limiting lateral bending.
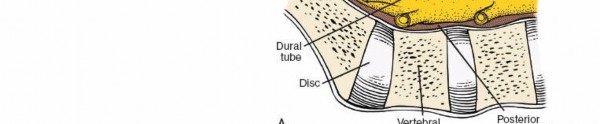
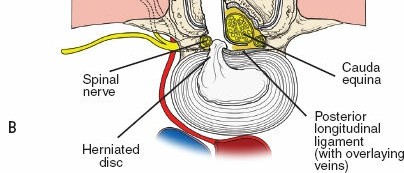
* Posterior longitudinal ligament (PLL): Located on the posterior surface of the vertebral bodies within the spinal canal, anterior to the dura. It helps prevent disc herniation and hyperflexion.
Muscular Anatomy
The posterior lumbar muscles are critical for spinal stability and movement. Surgical disruption can lead to significant postoperative pain and functional impairment.
* Superficial Layer: Latissimus dorsi, trapezius (in upper lumbar/thoracic levels).
* Intermediate Layer: Serratus posterior inferior.
* Deep Layer (Erector Spinae Group):
* Iliocostalis: Most lateral, involved in extension and lateral flexion.
* Longissimus: Intermediate, powerful extensor.
* Spinalis: Most medial, adjacent to spinous processes.
* The erector spinae muscles are typically detached subperiosteally from the spinous processes and laminae during traditional open approaches, often leading to muscle denervation, atrophy, and fatty infiltration.
* Deep Intrinsic Muscles:
* Multifidus: A segmental muscle with attachments spanning multiple vertebral levels. It plays a crucial role in segmental stability, proprioception, and fine motor control. It is often spared in muscle-sparing approaches (e.g., Wiltse approach).
* Rotatores: Deepest layer, also important for segmental stability and proprioception.
Neurovascular Anatomy
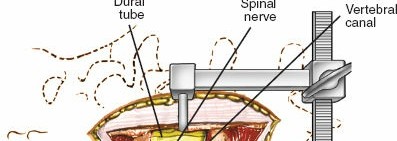
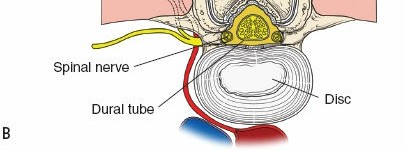
- Spinal Cord and Cauda Equina: The spinal cord typically terminates at the L1-L2 level (conus medullaris), continuing as the cauda equina (horse's tail) below this level. The cauda equina consists of lumbar, sacral, and coccygeal nerve roots. Injury to these structures can result in sensory, motor, or sphincter dysfunction.
- Nerve Roots: Exit the spinal canal via the intervertebral foramina. Each lumbar nerve root exits below its corresponding vertebra (e.g., L4 nerve root exits below L4 vertebra). In the spinal canal, the traversing nerve root (e.g., L5 traversing at L4/L5 disc) and the exiting nerve root (L4 exiting at L4/L5 foramen) must be identified and protected during decompression. The dorsal root ganglion (DRG) is often located within the neural foramen and is highly sensitive to compression.
- Segmental Arteries and Veins: Arise from the aorta and vena cava, respectively, supplying the vertebral bodies, spinal canal, and paraspinal muscles. These vessels can be encountered during deep dissection or pedicle screw placement and require careful management to prevent significant hemorrhage.
- Dorsal Rami: Innervate the facet joints, paraspinal muscles, and skin. Medial branches of the dorsal rami supply the facet joints and are often targeted for denervation procedures.
Biomechanics
The lumbar spine is a complex biomechanical system designed for both mobility and stability.
* Load Bearing: The vertebral bodies and intervertebral discs bear approximately 80% of axial compressive loads, while the posterior elements (facets, laminae, ligaments) bear the remaining 20%.
* Stability: Provided by the bony architecture, ligamentous structures (passive stabilizers), and muscles (active stabilizers). Disruption of these elements can lead to instability.
* Coupling Motion: Lumbar spine motion involves coupled movements. For example, during lateral bending, there is some degree of axial rotation.
* Fusion Principles: The goal of spinal fusion is to create a rigid construct that eliminates motion at a painful or unstable segment. This involves decortication of bony surfaces, application of bone graft, and often internal fixation with pedicle screws and rods to provide immediate stability while fusion occurs. The biomechanical constructs can be either anterior, posterior, or circumferential, with the posterior approach enabling several fusion strategies including posterolateral fusion and posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF).
* 
* 
* 
Indications and Contraindications
The posterior approach offers versatility for managing a broad spectrum of lumbar pathologies. Careful patient selection and comprehensive pre-operative assessment are paramount.
Indications for Posterior Lumbar Spine Surgery
- Degenerative Conditions:
- Lumbar Disc Herniation: Particularly large central or paracentral herniations causing radiculopathy or cauda equina syndrome refractory to conservative management.
- Spinal Stenosis: Central, lateral recess, or foraminal stenosis causing neurogenic claudication or radiculopathy refractory to conservative treatment.
- Degenerative Spondylolisthesis: Grade I or II with instability, radiculopathy, or neurogenic claudication that fails conservative management. Often requires decompression and fusion.
- Degenerative Disc Disease: Intractable axial low back pain with discogenic etiology, often managed with interbody fusion.
- Facet Arthropathy: Disabling facetogenic pain resistant to conservative measures, sometimes requiring facetectomy or fusion.
- Spinal Deformity:
- Adult Degenerative Scoliosis/Kyphoscoliosis: Progressive deformity, intractable pain, or neurological deficits requiring correction and fusion.
- Isthmic Spondylolisthesis: Higher grades (II-V) often require posterior reduction and fusion. Lower grades with persistent symptoms after conservative care may also be indicated.
- Traumatic Injuries:
- Thoracolumbar Fractures: Unstable burst fractures, fracture-dislocations, or chance fractures requiring posterior stabilization, often with decompression if neurological compromise exists.
- Ligamentous Injuries: Severe posterior ligamentous complex disruption leading to instability.
- Infection:
- Spinal Epidural Abscess: Requiring urgent decompression and debridement.
- Vertebral Osteomyelitis/Discitis: Debridement and stabilization, especially if progressive deformity or neurological compromise is present.
- Tumors:
- Primary or Metastatic Spinal Tumors: Requiring decompression, biopsy, and/or stabilization.
- Iatrogenic Conditions:
- Pseudarthrosis: Revision surgery for failed fusion.
- Adjacent Segment Disease: Decompression and/or fusion at levels adjacent to a previous fusion.
Contraindications for Posterior Lumbar Spine Surgery
- Absolute Contraindications:
- Uncorrectable coagulopathy.
- Active systemic infection or local infection not treatable by surgery.
- Severe medical comorbidities precluding safe anesthesia and surgery (e.g., uncontrolled cardiac disease, severe pulmonary dysfunction).
- Psychological overlay or secondary gain issues where surgery is unlikely to provide benefit.
- Relative Contraindications:
- Significant osteoporosis, which may compromise hardware fixation.
- Severe obesity, increasing surgical difficulty and complication rates.
- Prior extensive lumbar surgery, leading to significant scarring and anatomical distortion.
- Active smoking, which significantly impairs bone healing and fusion rates.
- Unrealistic patient expectations regarding surgical outcomes.
- Unilateral symptoms where a minimally invasive endoscopic approach might be more appropriate.
Operative vs Non Operative Indications
A multidisciplinary approach is crucial to determine the most appropriate management strategy.
| Indication Category | Operative Management Criteria | Non-Operative Management Criteria |
|---|---|---|
| Lumbar Disc Herniation | Progressive neurological deficit, Cauda Equina Syndrome, intractable radiculopathy > 6-12 weeks | Radicular pain without progressive deficit, responds to analgesics/PT, no cauda equina |
| Spinal Stenosis | Progressive neurogenic claudication, motor weakness, failure of conservative therapy > 3-6 months | Mild to moderate symptoms, tolerable pain, successful PT/epidural injections, no major deficit |
| Spondylolisthesis | Progressive slip, neurological deficit, intractable pain with instability, failure of 6 months non-op | Asymptomatic, mild symptoms, stable slip, good response to conservative management |
| Spinal Trauma | Unstable fracture (Denis B, C), neurological deficit, progressive deformity | Stable fracture (Denis A), no neurological deficit, managed with bracing/pain control |
| Spinal Infection | Neurological compromise, progressive deformity, uncontrolled sepsis, large abscess | Stable spine, no neurological deficit, responds to IV antibiotics, small, contained abscess |
| Spinal Tumor | Spinal cord compression, progressive neurological deficit, instability, intractable pain | Asymptomatic, stable, responding to radiation/chemotherapy, minimal tumor burden |
| Degenerative Disc Disease | Intractable discogenic pain documented by discography, failure of comprehensive conservative care | Mild to moderate axial back pain, responds to PT/NSAIDs, no neurological deficit |
Pre Operative Planning and Patient Positioning
Thorough pre-operative planning and meticulous patient positioning are fundamental to minimizing complications and optimizing outcomes in posterior lumbar spine surgery.
Pre Operative Planning
- Patient Selection and Optimization:
- Clinical Assessment: Detailed history, physical examination focusing on neurological status (motor, sensory, reflexes, sphincter function), pain characteristics, and functional limitations.
- Medical Optimization: Comprehensive medical clearance. Management of comorbidities (diabetes, hypertension, cardiac disease, pulmonary issues). Smoking cessation is strongly encouraged.
- Medication Review: Discontinuation of anticoagulants/antiplatelets as per institutional protocols. Consideration of perioperative steroids for inflammatory conditions or potential neurological deficits.
- Imaging Review:
- MRI: Essential for visualizing neural structures, disc pathology, ligamentous hypertrophy, and soft tissue involvement.
- CT Scan: Crucial for bony anatomy, assessing pedicle dimensions for screw planning, detecting fractures, evaluating fusion status, and surgical navigation planning.
- Dynamic Radiographs (Flexion/Extension): To assess spinal stability, particularly in cases of spondylolisthesis or suspected instability.
- Full-length Standing Radiographs: For assessment of sagittal and coronal balance, especially in deformity cases.
- Surgical Planning:
- Level Identification: Precise identification of surgical levels using anatomical landmarks on imaging, often corroborated with fluoroscopy intraoperatively.
- Implant Selection: Selection of appropriate pedicle screw lengths and diameters based on CT measurements. Planning for interbody cages, bone graft options (autograft, allograft, synthetic).
- Approach Strategy: Deciding between open vs. minimally invasive, traditional posterolateral fusion vs. interbody fusion (PLIF/TLIF).
- Blood Loss Management: Type and cross-match for potential transfusions, consider tranexamic acid (TXA) administration.
- Antibiotic Prophylaxis: Administer broad-spectrum antibiotics within 60 minutes of incision.
- Neuromonitoring: Plan for somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) or electromyography (EMG) where neurological risk is higher.
- Informed Consent: Detailed discussion with the patient regarding the procedure, potential benefits, risks (including specific neurological injury, infection, bleeding, hardware failure, pseudarthrosis), alternative treatments, and expected recovery.
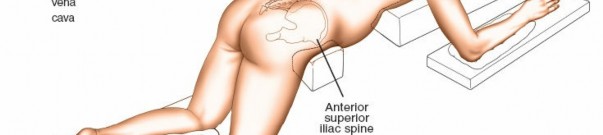
Patient Positioning
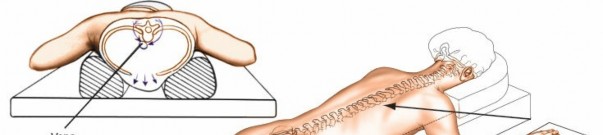
The prone position is standard for posterior lumbar spine surgery. Proper positioning is critical to minimize complications.
1. Anesthesia Induction: Administer general anesthesia and establish appropriate monitoring lines.
2. Prone Positioning Devices:
* Wilson Frame: Contours the patient's body, providing a lordotic curve and allowing the abdomen to hang freely. This reduces intra-abdominal pressure, minimizing epidural venous bleeding and improving surgical visualization.
* Jackson Table (Radiolucent Operating Table): Offers excellent imaging capabilities and adjustable features for desired spinal alignment.
* Chest Rolls/Bolsters: Placed longitudinally from clavicle to iliac crest, ensuring abdominal decompression and preventing pressure on neurovascular structures in the axilla and groin.
3. Padding and Pressure Point Protection:
* Ensure all pressure points (face, eyes, ears, shoulders, elbows, hips, knees, ankles, toes) are meticulously padded to prevent neuropathies (e.g., ulnar neuropathy, peroneal neuropathy) and skin breakdown.
* Maintain head in neutral alignment to prevent cervical spine injury and optimize venous outflow. Use a gel donut or headrest.
* Check breasts and genitalia for undue compression.
4. Spinal Alignment:
* Maintain a neutral or slightly lordotic lumbar alignment. Excessive kyphosis can make instrumentation difficult and increase stress on hardware.
* 
* 
5. Preparation and Draping:
* Surgical site is prepped with an antiseptic solution (e.g., chlorhexidine-alcohol) from the mid-thoracic region to the sacrum, extending laterally.
* Sterile draping to create a wide surgical field.
6. Fluoroscopy Setup:
* C-arm fluoroscopy unit should be positioned to allow for optimal anteroposterior (AP) and lateral views without contamination of the sterile field. This is critical for level localization and pedicle screw placement.
Detailed Surgical Approach and Technique
The posterior lumbar approach encompasses a variety of techniques, ranging from traditional open decompression and fusion to modern minimally invasive procedures. The core principles, however, remain consistent: accurate level localization, meticulous soft tissue dissection, neural decompression, and stable fixation when indicated.
Level Localization and Incision
- Pre-incisional Localization: Utilize fluoroscopy to identify the correct spinal level. A radiopaque marker (e.g., Kocher clamp, needle) is placed on the skin, and AP and lateral images are taken to confirm its position relative to the desired vertebral segment, typically by counting up from the sacrum or down from T12.
- Skin Incision: A midline longitudinal incision is typically made directly over the spinous processes, extending across the desired number of levels. For muscle-sparing approaches (e.g., Wiltse), paramedian incisions are utilized, splitting the multifidus from the longissimus muscles.
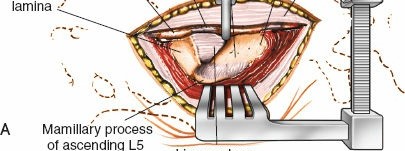
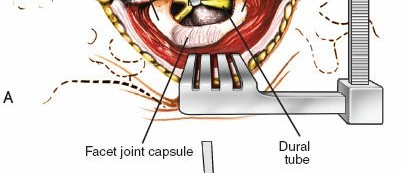
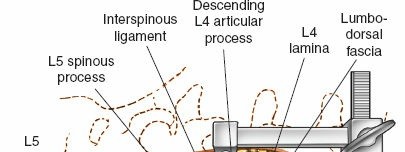
Soft Tissue Dissection and Exposure
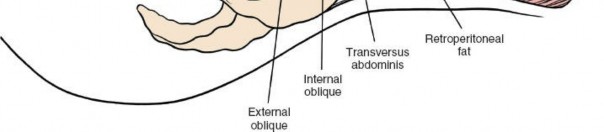
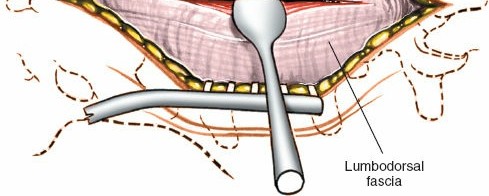
- Subcutaneous Dissection: Incise skin and subcutaneous fat down to the deep fascia (thoracolumbar fascia).
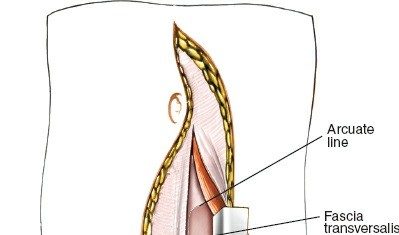
- Fascial Incision: A longitudinal incision is made through the thoracolumbar fascia, usually paramedially for muscle-sparing or directly in the midline for traditional open approaches.
- Muscle Dissection:
- Traditional Open Approach: Subperiosteal dissection of the paraspinal muscles (erector spinae) from the spinous processes and laminae using electrocautery and Cobb elevators. This exposes the posterior elements. Hemostasis is paramount during this stage.
- Minimally Invasive/Muscle-Sparing Approaches:
- Wiltse Approach: A paramedian incision is made, and the plane between the multifidus and longissimus muscles is identified and dissected bluntly. Serial dilators and a tubular retractor system are then used to create a working corridor. This preserves the multifidus innervation and blood supply.
- Endoscopic or microdiscectomy approaches utilize even smaller incisions and specialized instruments.
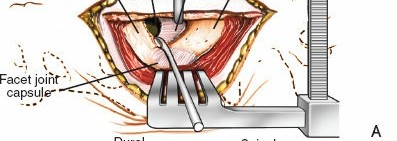
- Exposure: Retractors are carefully placed to maintain exposure of the spinous processes, laminae, facet joints, and transverse processes. Ensure nerve roots are not compressed by retractors.
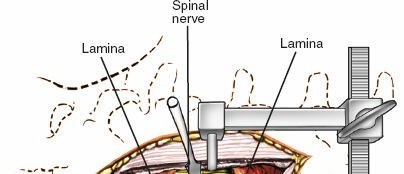
Decompression
The goal of decompression is to relieve neural compression causing radiculopathy or myelopathy.
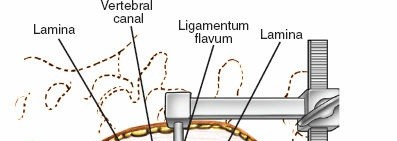
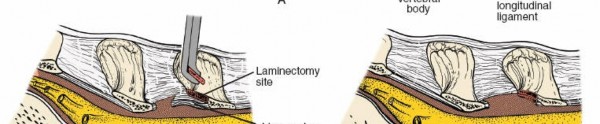
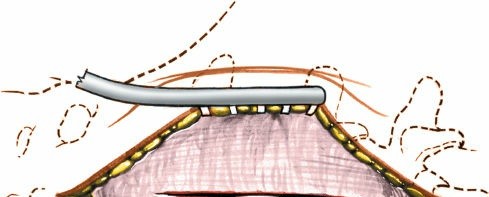
1. Laminotomy/Laminectomy:
* Using Kerrison rongeurs, osteotomes, or high-speed burrs, a laminotomy (partial removal of lamina) or laminectomy (complete removal of lamina) is performed. The ligamentum flavum is carefully resected.
* For central stenosis, bilateral decompression is often necessary.
* 
2. Medial Facetectomy: To relieve lateral recess stenosis or uncover the traversing nerve root, a portion of the medial facet joint may be resected. Care must be taken to preserve facet joint integrity if fusion is not planned.
3. Foraminotomy: Enlargement of the neural foramen to decompress the exiting nerve root, often achieved by removing osteophytes or portions of the superior articular process.
4. Discectomy (for herniation):
* After careful retraction of the nerve root (epiradicular fat often serves as a protective layer), the annulus fibrosus is incised.
* Herniated disc material is removed using pituitary rongeurs. Ensure thorough removal to prevent recurrence, but avoid excessive curettage that might damage the endplates.
* 
Instrumentation and Fusion
Instrumentation provides immediate stability, while fusion aims for biological union of spinal segments.
1. Pedicle Screw Placement:
* Entry Point: Typically located at the junction of the transverse process, superior articular process, and pars interarticularis. Specific entry points vary slightly by vertebral level (e.g., L5 often more medial).
* Awl/Drill: A cortical breach is made with an awl. A pedicle probe is then used to palpate the pedicle walls (medial, lateral, superior, inferior) to ensure contained trajectory.
* Tapping: The pedicle tract is tapped to create threads for the screw.
* Screw Insertion: Pedicle screws are then inserted. Fluoroscopy (AP and lateral) or navigation systems (CT-based, O-arm) are used to confirm accurate placement and trajectory, avoiding medial cortical breach (spinal canal) or lateral cortical breach (neurovascular structures).
* 
* 
* 
* 
2. Interbody Fusion (PLIF/TLIF):
* PLIF (Posterior Lumbar Interbody Fusion): Requires bilateral laminectomy and partial facetectomy. Both nerve roots are retracted to access the disc space from both sides. Two cages are typically inserted.
* TLIF (Transforaminal Lumbar Interbody Fusion): A unilateral approach performed through the neural foramen after a complete unilateral facetectomy. The traversing nerve root is retracted medially, and the exiting nerve root inferiorly. A single banana-shaped cage is typically inserted obliquely across the disc space. This approach is generally preferred for its reduced neural retraction and morbidity.
* Disc Space Preparation: The disc is thoroughly removed (curettage, rongeurs). The endplates are decorticated to expose bleeding bone, promoting fusion.
* Cage Insertion: An interbody cage, packed with bone graft (autograft, allograft, or bone graft substitute), is impacted into the disc space. This restores disc height, provides anterior column support, and indirect neural decompression.
* 
* 
3. Posterolateral Fusion:
* After pedicle screw insertion, the transverse processes and lateral aspects of the laminae are decorticated using a high-speed burr or osteotome to expose cancellous bone.
* Bone graft material (autograft from iliac crest, local decompression bone, or allograft) is then packed over the decorticated posterolateral gutters.
* 
* 
* 
4. Rod Contouring and Fixation:
* Connecting rods are contoured to restore physiological lordosis and connect the pedicle screws.
* Set screws are tightened to secure the rods to the screw heads. Intraoperative compression or distraction maneuvers may be applied to achieve desired spinal alignment or reduction of spondylolisthesis.
* 
* 
* 
* 
Closure
- Hemostasis: Thorough irrigation and meticulous hemostasis of the surgical bed.
- Drain Placement: A suction drain may be placed in the deep muscle layers to reduce hematoma formation, particularly in extensive cases or patients at higher bleeding risk.
- Fascial Closure: The thoracolumbar fascia is meticulously closed with strong, absorbable sutures. This is critical for preventing muscle herniation and providing stability to the posterior musculature.
- Subcutaneous and Skin Closure: Layered closure of subcutaneous tissue and skin using appropriate sutures.
Complications and Management
Despite advancements, posterior lumbar spine surgery carries inherent risks. A comprehensive understanding of potential complications and their management is essential.
Intraoperative Complications
- Dural Tear (CSF Leak): Incidence 1-10%. Can occur during laminectomy, ligamentum flavum resection, or disc removal.
- Management: Primary repair with non-absorbable sutures, fibrin glue, dural sealant, or fat graft. If large, consider a lumbar drain post-operatively.
- Nerve Root Injury: Incidence <1-5%. Can lead to new or worsened radiculopathy, motor weakness, or sensory loss. Caused by direct trauma, excessive retraction, or thermal injury.
- Management: Identify and release compression, meticulous dissection, consideration of intraoperative nerve monitoring. Post-operatively, steroids may be considered.
- Vascular Injury: Rare but serious (e.g., great vessels during anterior annulus perforation for interbody fusion, segmental vessels).
- Management: Immediate compression, vascular surgery consultation, open repair, or angiography/embolization.
- Pedicle Screw Malposition: Incidence 5-20% depending on technique (freehand vs. navigation). Can cause neurological injury if intraspinal, or vascular/visceral injury if extrapedicular.
- Management: Intraoperative fluoroscopy/navigation confirmation. If malposition is significant or symptomatic, revise immediately.
- Excessive Blood Loss: Common in multi-level fusions.
- Management: Meticulous hemostasis, TXA, controlled hypotension, cell saver, blood transfusion.
- Hardware Failure: Intraoperative breakage of screws or rods.
- Management: Replace hardware.
Early Postoperative Complications
- Surgical Site Infection (SSI): Incidence 0.5-5%. Superficial or deep.
- Management: Prophylactic antibiotics. If superficial, oral antibiotics. If deep, surgical debridement, IV antibiotics, and potentially hardware removal if chronic.
- Hematoma/Seroma: Can cause neural compression or wound dehiscence.
- Management: Surgical evacuation if symptomatic or large; observation for small, asymptomatic collections. Drains may prevent this.
- Persistent CSF Leak/Pseudomeningocele: Due to unrepaired or failed dural repair.
- Management: Bed rest, lumbar drain, re-operation for direct repair if conservative measures fail.
- Neurological Deficit (New or Worsened): Due to intraoperative injury, hematoma, or inadequate decompression.
- Management: Urgent investigation (MRI/CT), surgical exploration if mass lesion (hematoma) or unaddressed compression is suspected.
- Ileus: Common after extensive spinal surgery.
- Management: Bowel rest, nasogastric tube (rarely), prokinetics.
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Risk related to prolonged immobility and surgical trauma.
- Management: Prophylactic anticoagulation, pneumatic compression devices, early mobilization.
- Urinary Retention: Common, especially in males.
- Management: Foley catheter, alpha-blockers.
Late Postoperative Complications
- Pseudarthrosis (Non-Union): Incidence 5-30% depending on patient factors and fusion type. Leading cause of persistent pain after fusion.
- Management: Revision surgery with re-debridement, additional bone graft, revised or augmented instrumentation. Bone stimulators, smoking cessation.
- Adjacent Segment Disease (ASD): Degeneration at levels adjacent to a fused segment, due to altered biomechanics. Incidence 2-4% per year.
- Management: Decompression and/or extension of fusion to the affected adjacent segment.
- Hardware Prominence/Failure: Screws or rods may become symptomatic or break, particularly in cases of pseudarthrosis or severe osteoporosis.
- Management: Hardware removal if symptomatic after successful fusion; revision of fusion and instrumentation if associated with pseudarthrosis.
- Chronic Pain: Despite technically successful surgery, pain can persist due to nerve damage, muscle atrophy, psychosocial factors, or other untreated pathology.
- Management: Multidisciplinary pain management, physical therapy, psychological counseling, further diagnostic workup.
Complications and Management Table
| Complication Category | Specific Complication | Incidence (Approximate Range) | Salvage/Management Strategies |
|---|---|---|---|
| Intraoperative | Dural Tear (CSF Leak) | 1-10% | Primary repair with suture, fibrin glue, dural sealant. Consider lumbar drain. |
| Nerve Root Injury | <1-5% | Meticulous dissection, minimize retraction, intraoperative neuromonitoring. Post-op steroids, surgical exploration for compression. | |
| Vascular Injury | <0.1% | Immediate compression, vascular surgery consultation, repair. | |
| Pedicle Screw Malposition | 5-20% | Intraoperative imaging verification (fluoroscopy, O-arm navigation). Immediate revision if intraspinal or critical extrapedicular. | |
| Excessive Blood Loss | Variable | Meticulous hemostasis, TXA, controlled hypotension, cell saver, blood transfusion. | |
| Early Postoperative | Surgical Site Infection | 0.5-5% | Prophylactic antibiotics. Superficial: oral antibiotics. Deep: surgical debridement, IV antibiotics. |
| Hematoma | 1-3% | Surgical evacuation if symptomatic neurological deficit or significant size. | |
| Persistent CSF Leak | 0.5-2% | Bed rest, lumbar drain. Re-operation for direct repair if conservative fails. | |
| Neurological Deficit | <1-5% | Urgent imaging (MRI/CT), surgical exploration for compressive hematoma or inadequate decompression. | |
| DVT/PE | <1-5% | Prophylactic anticoagulation, mechanical compression devices, early mobilization. Treatment with therapeutic anticoagulation. | |
| Late Postoperative | Pseudarthrosis (Non-Union) | 5-30% | Revision surgery with re-debridement, fresh bone graft, instrumentation revision/augmentation. Bone stimulators, smoking cessation. |
| Adjacent Segment Disease | 2-4% per year | Decompression and/or extension of fusion to symptomatic adjacent level. | |
| Hardware Prominence | 5-10% | Hardware removal if symptomatic and fusion is solid. | |
| Chronic Post-Op Pain | Variable | Multidisciplinary pain management, intensive physical therapy, psychological support, further diagnostic evaluation. |
Post Operative Rehabilitation Protocols
A structured and progressive postoperative rehabilitation protocol is crucial for maximizing functional recovery, preventing complications, and achieving long-term success after posterior lumbar spine surgery. Protocols must be tailored to the specific procedure performed (e.g., decompression-only vs. fusion) and individual patient factors.
Immediate Post Operative Phase (Hospital Stay Days 0-3)
- Pain Management: Aggressive multimodal analgesia including opioids, NSAIDs (if no contraindication), acetaminophen, and nerve blocks to facilitate early mobilization.
- Wound Care: Monitor incision for signs of infection, hematoma, or CSF leak. Dressing changes per protocol.
- Mobilization:
- Day 0 (POD 0): Log-roll technique for position changes. Early sitting and short walks with assistance, often within hours of surgery, particularly for decompression-only cases.
- Day 1 (POD 1): Progressive ambulation with increasing distances. Stair climbing practice.
- Activity Restrictions: Reinforce "BLT" precautions (No Bending, Lifting over 5-10 lbs, Twisting) for fusion patients. Decompression-only patients may have fewer restrictions but should still avoid excessive spinal loading.
- DVT Prophylaxis: Continue chemical prophylaxis (e.g., LMWH) and mechanical prophylaxis (sequential compression devices, early ambulation).
- Bladder and Bowel Function: Monitor for urinary retention and resumption of bowel function.
Early Rehabilitation Phase (Weeks 1-6)
- Activity Modification: Strict adherence to "BLT" precautions for fusion patients. Gradual increase in general activity. Avoid prolonged sitting.
- Bracing: For fusion patients, a rigid thoracolumbosacral orthosis (TLSO) or lumbar sacral orthosis (LSO) may be prescribed, especially for multi-level fusions, osteoporotic patients, or those with concerns about compliance. Its utility for routine single-level instrumented fusions is debated.
- Physical Therapy (PT) Referrals:
- Education: Emphasis on proper body mechanics, posture, lifting techniques, and spine protection.
- Gentle Mobility: Gradual introduction of range-of-motion exercises within pain-free limits.
- Core Stabilization: Isometric core exercises (e.g., abdominal bracing, pelvic tilts) without spinal movement.
- Walking: Encourage daily walking as tolerated to build endurance and promote circulation.
- Driving: Typically restricted for 2-4 weeks, or longer if on opioids or unable to safely operate controls.
- Return to Work: Sedentary work may be possible at 2-4 weeks; physically demanding work typically requires 3-6 months.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Progressive Strengthening: Advance core strengthening exercises (e.g., bird-dog, planks) focusing on deep abdominal and multifidus activation. Introduce light resistance exercises for extremities.
- Flexibility: Gentle stretching of hamstrings and hip flexors.
- Endurance Training: Continue increasing duration and intensity of walking, stationary cycling, or swimming (once wound healed).
- Proprioception and Balance: Exercises to improve balance and coordination.
- Occupational Therapy (OT) Referral: May be beneficial for ergonomic assessment and modification of daily activities.
- Radiographic Assessment: Plain radiographs (AP, lateral, flexion/extension) at 6-12 weeks post-fusion to assess alignment, hardware integrity, and early signs of fusion.
Late Rehabilitation Phase (Months 3-6 and Beyond)
- Advanced Strengthening: Progress to more dynamic and functional exercises. Incorporate exercises for hip abductors, gluteals, and upper body.
- Sport-Specific Training: For athletes, a gradual return to sport-specific activities under supervision.
- Return to Full Activities: Gradual return to recreational activities and physically demanding work. Heavy lifting and high-impact activities should be introduced cautiously and based on clinical and radiographic evidence of fusion.
- Long-Term Spinal Health: Lifelong emphasis on maintaining a healthy weight, regular exercise, proper body mechanics, and avoiding smoking.
- Fusion Assessment: A CT scan at 6-12 months post-fusion is the gold standard for assessing fusion mass maturity and bony bridging. Clinical assessment of pain and function remains paramount.
Specific Considerations
- Decompression-Only Patients: Generally have a faster recovery with fewer restrictions, focusing on early mobilization and core strengthening to prevent recurrence.
- Elderly Patients: May require a slower progression, greater emphasis on balance and fall prevention, and consideration of comorbidities.
- Revision Surgery: Rehabilitation may be more challenging due to scar tissue and prior muscle damage, often requiring more intensive and prolonged PT.
Summary of Key Literature and Guidelines
The posterior approach to the lumbar spine is underpinned by extensive clinical research and established guidelines, continually evolving with technological and surgical advancements.
Evidence Based Guidelines
- NASS (North American Spine Society) Clinical Guidelines: Provide evidence-based recommendations for various lumbar spine conditions including lumbar disc herniation, spinal stenosis, and spondylolisthesis. These guidelines systematically review literature to inform best practices for diagnosis, non-operative, and operative management, often specifying the role of posterior decompression and fusion.
- AOSpine International: Offers classification systems for spinal trauma and tumors, which dictate surgical indications and approaches, frequently highlighting posterior stabilization for unstable injuries or tumors causing neural compression.
- Cochrane Reviews: Regularly update systematic reviews on surgical interventions for low back pain conditions. For example, reviews on discectomy for sciatica or fusion for degenerative disc disease provide critical insights into efficacy and comparative outcomes of posterior approaches.
Landmark Studies and Key Literature
- SPORT (Spine Patient Outcomes Research Trial): A seminal series of randomized controlled trials comparing operative and non-operative treatments for lumbar disc herniation, spinal stenosis, and degenerative spondylolisthesis.
- Lumbar Disc Herniation: Demonstrated a clear benefit of surgery (often microdiscectomy via posterior approach) over non-operative care for carefully selected patients with persistent radiculopathy, although initial differences diminished over time.
- Spinal Stenosis: Showed significantly better outcomes with decompressive laminectomy (posterior approach) compared to non-operative treatment for symptomatic lumbar spinal stenosis.
- Degenerative Spondylolisthesis: Found that decompression plus fusion (posterior instrumented fusion) resulted in better outcomes than decompression alone for patients with degenerative spondylolisthesis and spinal stenosis, especially regarding pain relief and functional improvement, reinforcing the role of posterior fusion for instability.
- Studies on Minimally Invasive Spine Surgery (MISS): Numerous comparative studies have evaluated MIS posterior approaches (e.g., tubular microdiscectomy, MIS TLIF) against traditional open techniques. While functional outcomes at long term are often similar, MIS techniques typically demonstrate benefits such as reduced blood loss, shorter hospital stays, less postoperative pain, and potentially reduced muscle damage and quicker return to activity. However, they may have a steeper learning curve and potentially higher initial complication rates for less experienced surgeons.
- Fusion Rates and Bone Grafting Strategies: Extensive literature compares different bone graft materials (autograft, allograft, synthetic osteoinductive/osteoconductive agents) and fusion techniques (posterolateral fusion vs. interbody fusion). Autograft (iliac crest) remains the gold standard for fusion rates but carries donor site morbidity. Contemporary approaches often utilize local autograft mixed with allograft or synthetics, with interbody fusion showing generally higher fusion rates due to provision of anterior column support and increased surface area for fusion.
- Adjacent Segment Disease (ASD) Research: Ongoing research explores the incidence, predictors, and prevention strategies for ASD following lumbar fusion. While a natural history of degeneration, fusion can accelerate it. Techniques like dynamic stabilization, hybrid constructs, and motion-preserving devices are being investigated, though posterior fusion remains the workhorse.
Current Trends and Future Directions
- Enhanced Recovery After Surgery (ERAS) Protocols: Increasingly adopted in spine surgery to optimize patient outcomes through multimodal pain management, early mobilization, and reduced length of hospital stay.
- Robotics and Navigation: Integration of robotic platforms and advanced intraoperative navigation systems for pedicle screw placement enhances accuracy, reduces radiation exposure, and improves surgical efficiency, particularly in complex deformity or revision cases.
- Augmented Reality (AR) and Virtual Reality (VR): Emerging technologies for surgical planning, simulation, and intraoperative guidance, offering immersive and precise anatomical visualization.
- Biological Augmentation: Continued research into novel biological agents (e.g., mesenchymal stem cells, growth factors) to enhance fusion rates and potentially regenerate disc tissue.
- Data Analytics and Artificial Intelligence (AI): Utilization of large datasets to predict surgical outcomes, personalize treatment plans, and identify high-risk patients, aiming to improve patient selection and minimize complications.
In conclusion, the posterior approach remains indispensable in orthopedic spine surgery. Mastery requires a profound understanding of surgical anatomy, biomechanics, a disciplined surgical technique, and an evidence-based approach to patient selection and rehabilitation. Continuous engagement with evolving literature and adoption of validated technological advancements will further refine patient care and outcomes in spinal surgery.
Clinical & Radiographic Imaging
You Might Also Like