Master the Anterolateral Retroperitoneal Approach to Lumbar Spine
Key Takeaway
Here are the crucial details you must know about Master the Anterolateral Retroperitoneal Approach to Lumbar Spine. The anterolateral retroperitoneal approach is a surgical technique providing anterior access to the lumbar spine, from L1 to the sacrum. This approach safely allows infection drainage without peritoneal contamination. Key uses include spinal fusion, vertebral body or disc resection, psoas abscess drainage, and disc prosthesis insertion, typically performed with the patient in a semilateral position.
Introduction and Epidemiology
The anterolateral retroperitoneal approach to the lumbar spine represents a cornerstone in the armamentarium of spinal surgeons, offering direct anterior access to the vertebral bodies and intervertebral discs from L1 to S1. This surgical corridor has evolved significantly since its inception, providing distinct advantages over other anterior access routes, particularly the transperitoneal approach. Its utility spans a broad spectrum of spinal pathologies, making it an indispensable technique for comprehensive anterior column reconstruction and stabilization.
The retroperitoneal approach to the anterior part of the lumbar spine has several advantages over the transperitoneal approach. First, it provides access to all vertebrae from L1 to the sacrum, whereas the transperitoneal approach is very difficult to use above the level of L4. Second, it allows drainage of an infection, such as a psoas abscess, without the risk of contaminating the peritoneal cavity and causing a postoperative ileitis. Because of the arrangement of the vascular anatomy of the retroperitoneal space, however, it is slightly more difficult to reach the L5-S1 disc space using this retroperitoneal approach.
Epidemiologically, conditions necessitating anterior lumbar access, such as degenerative disc disease, adult spinal deformity, trauma, infection, and tumors, continue to represent a substantial global health burden. The precise incidence of procedures utilizing the anterolateral retroperitoneal approach is often conflated with overall anterior lumbar interbody fusion (ALIF) rates. However, its adoption has steadily increased, particularly with advancements in instrumentation, minimally invasive techniques, and a clearer understanding of sagittal balance restoration. The left-sided retroperitoneal approach is generally preferred due to the more favorable anatomy of the great vessels, specifically the ability to mobilize the descending aorta more readily than the inferior vena cava.
Surgical Anatomy and Biomechanics
A thorough understanding of the regional surgical anatomy and the biomechanical principles of the lumbar spine is paramount for the safe and effective execution of the anterolateral retroperitoneal approach.
Retroperitoneal Space Anatomy
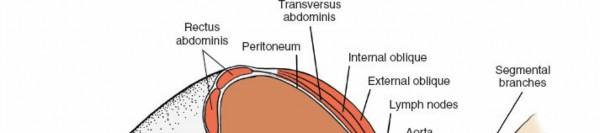
The retroperitoneal space is a complex anatomical compartment located posterior to the peritoneum and anterior to the vertebral column, extending from the diaphragm superiorly to the pelvic brim inferiorly. Key structures within this space include:
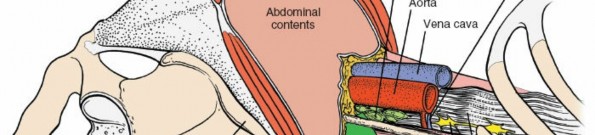
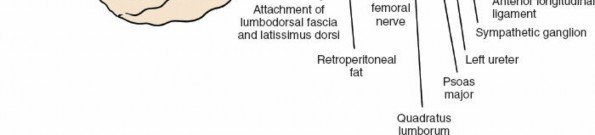
- Great Vessels: The abdominal aorta descends along the left anterior aspect of the vertebral bodies, bifurcating into the common iliac arteries typically at the L4-L5 level. The inferior vena cava (IVC) lies to the right of the aorta, forming from the confluence of the common iliac veins. Segmental lumbar arteries and veins arise directly from these major vessels and course laterally over the vertebral bodies, necessitating careful identification and often ligation during exposure. The left common iliac vein typically crosses anterior to the L5-S1 disc space, often complicating exposure at this level, particularly from a right-sided approach.
- Muscles: The psoas major muscles originate from the transverse processes and lateral aspects of the lumbar vertebral bodies, forming a significant anatomical landmark. The quadratus lumborum muscles lie lateral to the psoas.
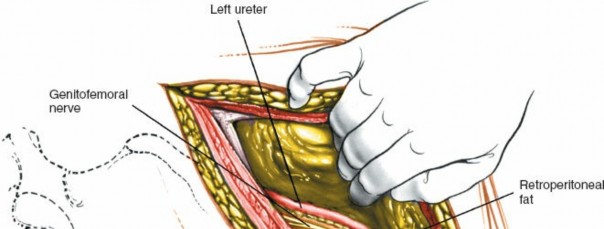
- Nerves: The lumbar plexus, derived from the anterior rami of L1-L4, lies within the psoas muscle. Key nerves to identify and protect include the genitofemoral nerve, which typically courses on the anterior surface of the psoas, and the sympathetic chain, which runs along the anterolateral aspect of the vertebral bodies medial to the psoas. Damage to the sympathetic chain can lead to retrograde ejaculation in males, a significant potential complication. The femoral nerve, emerging from the lateral border of the psoas, is at risk with aggressive lateral retraction.
- Ureters: The ureters descend retroperitoneally, typically lying anterior to the psoas muscle and often adherent to the posterior peritoneum. Their identification and gentle mobilization are crucial to prevent injury.
- Lymphatics: Numerous lymph nodes and lymphatic channels are present within the retroperitoneal space, particularly around the great vessels.
Lumbar Vertebral Anatomy
The lumbar vertebral bodies are large and kidney-shaped, designed to bear axial loads. The intervertebral discs consist of an annulus fibrosus and nucleus pulposus, providing flexibility and shock absorption. The endplates, comprising a thin layer of hyaline cartilage overlying compact bone, are critical for disc nutrition and fusion. Preservation of the bony endplate during discectomy is essential for robust fusion and minimizing subsidence.
Biomechanical Considerations
The anterior column of the lumbar spine is the primary load-bearing structure, supporting approximately 80% of axial compressive loads in an upright posture. Anterior column pathologies, such as severe disc degeneration, osteomyelitis, or tumor, compromise this structural integrity, leading to instability, pain, and progressive deformity.
The anterolateral retroperitoneal approach facilitates:
* Direct Decompression: Unimpeded access to the anterior aspect of the spinal canal for decompression of neural elements, particularly in cases of burst fractures or large central disc herniations.
* Restoration of Anterior Column Height: Placement of large interbody grafts or cages allows for restoration of disc space height, correction of regional lordosis, and indirect decompression of neural foramina.
* Increased Fusion Surface Area: The ability to insert wide, lordotic interbody devices spanning the entire endplate offers a significantly larger surface area for fusion compared to posterior approaches, theoretically enhancing fusion rates.
* Sagittal Balance Restoration: Anterior column support is critical for maintaining or restoring physiological lumbar lordosis, which is a key determinant of sagittal balance and functional outcomes.
Indications and Contraindications
The anterolateral retroperitoneal approach provides a versatile corridor for treating a variety of lumbar spinal pathologies. Careful patient selection is crucial to optimize outcomes and minimize complications.
Operative Indications
The uses of this approach include the following:
* Spinal Fusion (ALIF): Anterior Lumbar Interbody Fusion for degenerative disc disease, spondylolisthesis (degenerative or low-grade isthmic), post-discectomy syndrome, or pseudarthrosis. This is often performed in conjunction with posterior instrumentation for circumferential fusion in complex cases or high-grade spondylolisthesis.
* Drainage of Psoas Abscess and Curettage of Infected Vertebral Body: Direct access allows for debridement of infected tissue, culture collection, and placement of local antibiotics, without contaminating the peritoneal cavity. This is particularly relevant for discitis or vertebral osteomyelitis.
* Resection of all or part of a Vertebral Body and/or Intervertebral Disc and Associated Bone Grafting: Indicated for tumor resection (e.g., metastatic disease, primary bone tumors), severe burst fractures requiring anterior column reconstruction, or correction of severe kyphotic deformities.
* Biopsy of a Vertebral Body when a needle biopsy is either not possible or hazardous: Open biopsy provides a larger tissue sample and is safer in cases with challenging anatomy or proximity to critical neurovascular structures.
* Insertion of Disc Prosthesis: For total disc replacement in select patients with single-level degenerative disc disease who meet specific criteria.
* Correction of Spinal Deformity: As part of a multi-stage correction for severe adult spinal deformity, particularly to achieve anterior column lengthening and lordosis correction.
Contraindications
- Absolute Contraindications:
- Severe vascular disease: Aortic aneurysm, severe atherosclerosis, or prior vascular surgery with extensive scarring that makes mobilization of great vessels hazardous.
- Prior extensive retroperitoneal surgery or radiation: May result in dense adhesions, obliterating anatomical planes and increasing the risk of organ and vascular injury.
- Active intra-abdominal infection or peritonitis: Increases the risk of spreading infection.
- Uncorrected coagulopathy.
- Severe medical comorbidities precluding major surgery.
- Relative Contraindications:
- Obesity: Can make exposure more challenging due to increased depth of field.
- Previous abdominal surgery (laparotomy): May increase the risk of peritoneal adhesions.
- Inexperienced surgical team: The procedure requires a proficient spinal surgeon, and often co-management with a vascular surgeon, particularly for L5-S1 or revision cases.
- Single-level pathology amenable to a less invasive posterior or lateral approach without compromising biomechanical goals.
Operative vs Non Operative Indications for Anterior Lumbar Access
| Indication Category | Operative Criteria | Non-Operative Considerations |
|---|---|---|
| Degenerative Disc Disease | Intractable axial low back pain refractory to conservative management, imaging evidence of severe disc degeneration or instability, sagittal imbalance. | Mild to moderate pain, initial trial of NSAIDs, physical therapy, epidural injections, lifestyle modifications. |
| Spondylolisthesis | Progressive slip, neurological deficit, intractable pain despite conservative treatment, high-grade slips requiring reduction. | Stable, low-grade slip (Grade I-II), no neurological compromise, pain controlled with conservative measures. |
| Spinal Infection | Abscess formation, neurological deficits, spinal instability, failure of antibiotic therapy, severe pain. | Early, localized infection responsive to IV antibiotics, no neurological deficit or instability. |
| Spinal Tumors | Spinal cord compression, progressive neurological deficit, intractable pain, spinal instability, biopsy required. | Asymptomatic incidental findings, non-aggressive tumors without instability, patient unfit for surgery. |
| Spinal Trauma | Neurological deficit, spinal instability (e.g., burst fracture with retropulsion), severe kyphotic deformity. | Stable fractures, no neurological deficit, managed with bracing and rehabilitation. |
| Disc Herniation | Large central herniation, recurrent herniation, contained annulus, or calcified disc not amenable to posterior approaches, neurological deficit. | Radicular symptoms responsive to conservative care, small contained herniations. |
| Failed Back Surgery Syndrome | Pseudarthrosis, hardware failure, adjacent segment disease, recurrent disc herniation, severe pain. | Persistent pain without clear surgical target, psychological factors, failed comprehensive conservative care post-op. |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning and appropriate patient positioning are essential for optimizing exposure, minimizing complications, and achieving favorable surgical outcomes.
Preoperative Evaluation
A comprehensive evaluation is critical:
* Detailed History and Physical Examination: Assess pain characteristics, neurological deficits, functional limitations, and prior surgical history. Special attention to a history of vascular disease, prior abdominal surgery, or radiation.
* Advanced Imaging:
* Plain Radiographs: Standing AP/Lateral views to assess global and regional spinal alignment, segmental lordosis, and stability. Flexion/extension views may be indicated for instability.
* Magnetic Resonance Imaging (MRI): Provides detailed visualization of neural elements, disc pathology, soft tissues, and presence of infection or tumor.
* Computed Tomography (CT) Scan: Essential for bony detail, assessment of fracture patterns, tumor extent, and integrity of endplates. A CT angiogram (CTA) is strongly recommended, especially for L5-S1 cases or revisions, to precisely map the great vessels and their relationship to the surgical target. This helps identify aberrant vascular anatomy, significant calcification, or aneurysms.
* Vascular Surgery Consultation: Routinely indicated for L5-S1 approaches, cases with complex vascular anatomy (e.g., significant atherosclerosis, tortuous vessels), revisions, or in patients with a history of vascular disease. The vascular surgeon can assist with exposure, vessel mobilization, and repair in case of injury.
* Laboratory Investigations: Routine blood work, coagulation profile.
* Medical Clearance: Optimization of patient comorbidities by internal medicine or anesthesia.
Anesthesia Considerations
- Arterial Line: For continuous blood pressure monitoring.
- Central Venous Access: May be considered for complex cases, significant blood loss anticipation.
- Fluid Management: Judicious fluid management to maintain hemodynamic stability.
- Neuromonitoring: SSEP/MEP monitoring may be used, particularly in deformity correction or if posterior instrumentation is also planned.
- Blood Availability: Cross-matched blood should be readily available.
Patient Positioning
The primary goal of positioning is to allow the abdominal contents to fall away from the retroperitoneal space, facilitating exposure and minimizing retraction.
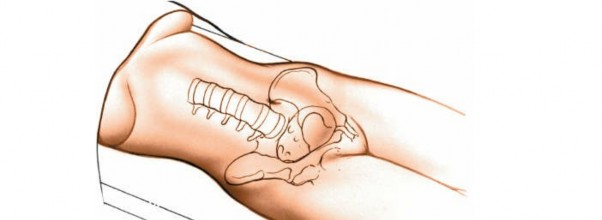
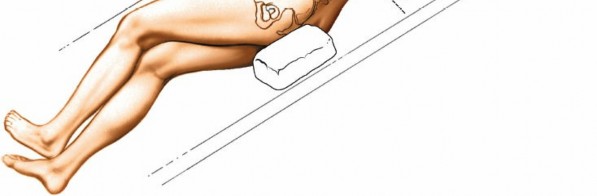
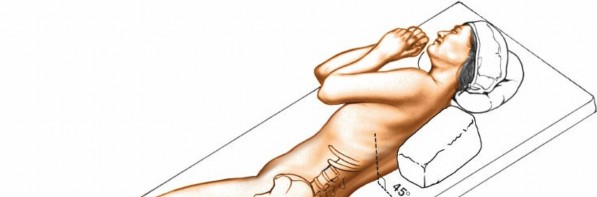
Place the patient on a radiolucent operating table in the semilateral position. The patient’s body should be at about a 45- to 90-degree angle to the horizontal, facing away from the surgeon. Keep the patient in this position throughout the surgery by placing sandbags under the hips and shoulders or by using a kidney rest brace to hold the patient. The angle allows the peritoneal contents to fall away from the incision. Alternatively, place the patient supine on the operating table and tilt the table at 45 degrees to the horizontal away from the surgeon. This position has the advantage of not putting the psoas muscle on stretch (Fig. 6-37). Ensure that you can obtain adequate radiographs of the area of the spine to be approached before prepping and draping.
Specific positioning considerations:
* Table Type: Use a flat, radiolucent table for C-arm access.
* Side of Approach: The left-sided approach is generally preferred due to the more mobile aorta and the more easily controlled lumbar vessels originating from the left. The IVC on the right is thinner-walled and more prone to injury and often less mobile. Additionally, the descending colon is on the left, which is easier to mobilize than the ascending colon on the right.
* Padding: Meticulous padding of all pressure points (axilla, knees, ankles) to prevent nerve compression or skin breakdown.
* C-arm Access: Crucially, confirm unimpeded C-arm access for both AP and lateral views before prepping and draping. The table and patient position must allow for accurate radiographic confirmation of the spinal level.
Incision Planning and Landmark Identification
The incision location and orientation depend on the target spinal level.
* L1-L2, L2-L3: Incision typically centered over the 12th rib, extending inferomedially.
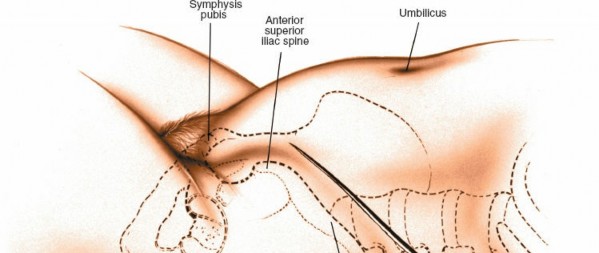
* L3-L4, L4-L5: Incision usually starts 2-3 cm anterior to the anterior superior iliac spine (ASIS) and courses obliquely towards the umbilicus, extending several centimeters above and below the target disc space.
* L5-S1: A lower, more horizontal or slightly oblique incision, approximately 3-4 cm superior and parallel to the iliac crest, extending towards the umbilicus.
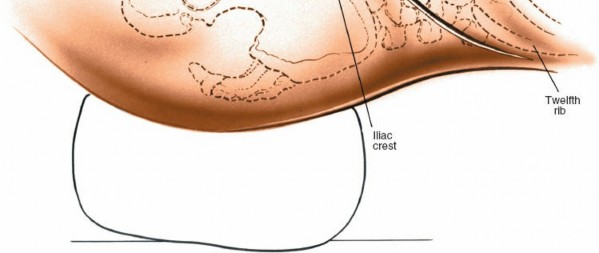
Landmarks:
* Costal margin
* Iliac crest
* Umbilicus
* ASIS
Preoperative localization using fluoroscopy or palpable anatomical landmarks helps guide the incision.
Detailed Surgical Approach and Technique
The retroperitoneal approach involves a systematic dissection through the abdominal wall musculature, identification of retroperitoneal structures, mobilization of the peritoneum and great vessels, and finally, direct access to the anterior lumbar spine.
Incision and Initial Dissection
-
Skin Incision: Make an oblique incision in the left lower quadrant of the abdomen (or right, if chosen), roughly parallel to the external oblique fibers, centered over the target disc space. The length varies but is typically 8-15 cm depending on patient habitus and the extent of exposure needed.

-
Subcutaneous Tissue: Incise the subcutaneous fat down to the external oblique fascia. Electrocautery is used for hemostasis.

-
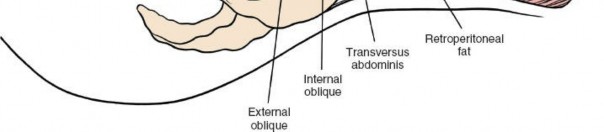
Muscle Layers:
-
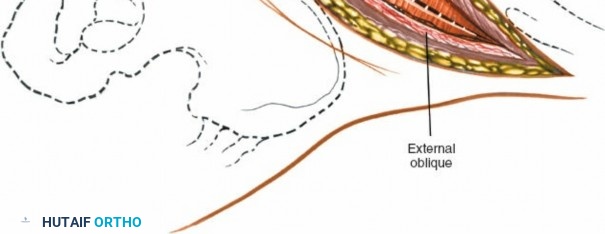
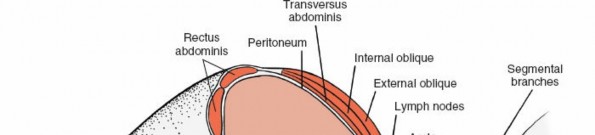
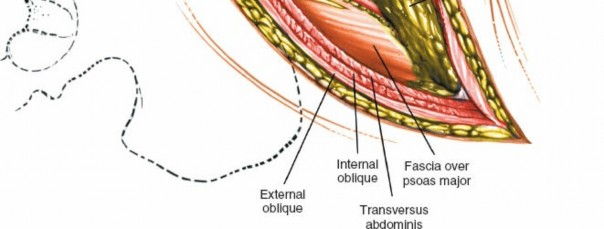
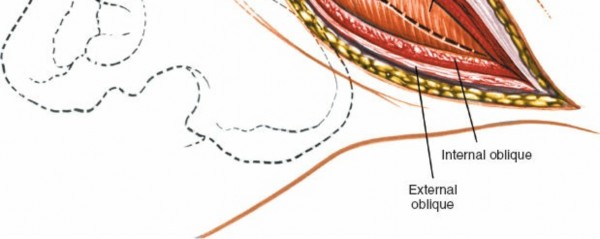
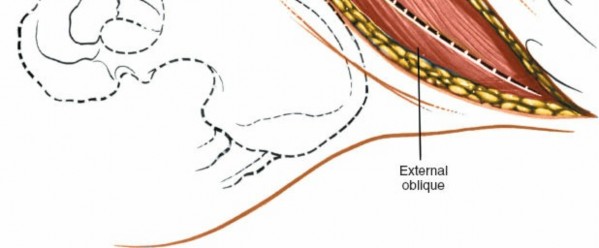
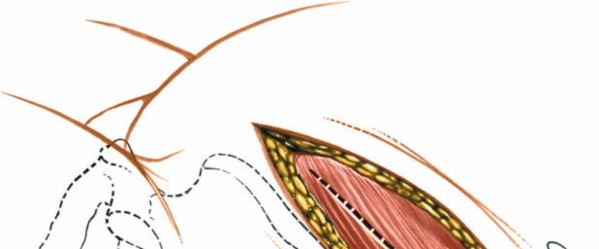
External Oblique: Incise the external oblique muscle and its aponeurosis along the line of the skin incision.
-
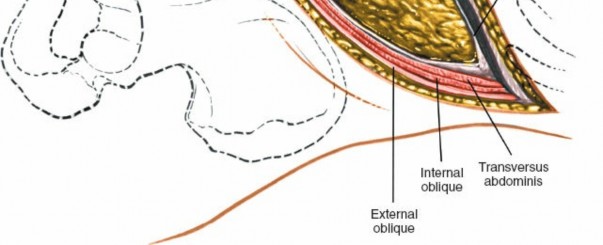
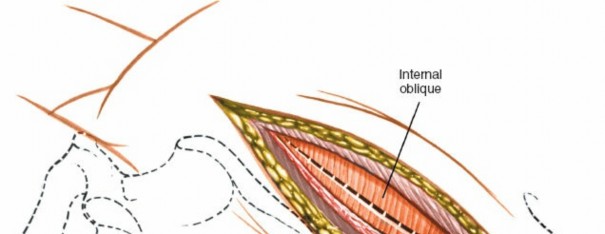
Internal Oblique: Retract the external oblique and carefully incise the internal oblique muscle. Identify the neurovascular bundles (iliohypogastric, ilioinguinal nerves) that run between the internal oblique and transversus abdominis. These should be identified and protected, typically retracted superiorly or inferiorly.
-
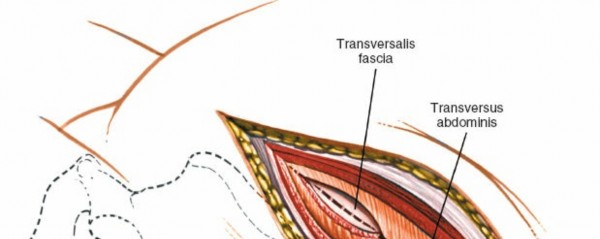
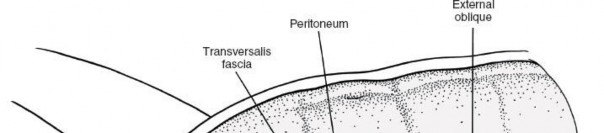
Transversus Abdominis: The deepest muscle layer is the transversus abdominis. Incise this muscle carefully, revealing the underlying transversalis fascia. The muscle fibers run transversely.

-
Retroperitoneal Entry
-
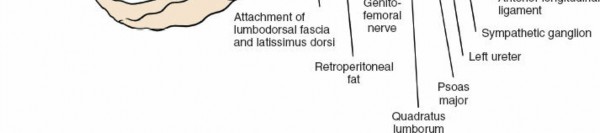
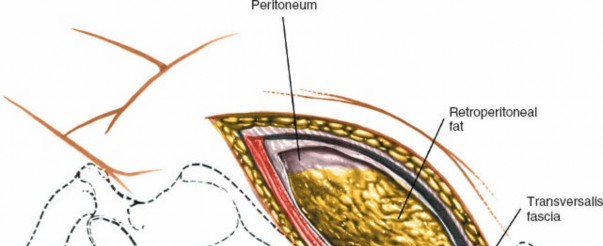
Transversalis Fascia and Peritoneum: Once the transversus abdominis is incised, the transversalis fascia is encountered. Directly deep to this is the retroperitoneal fat and the parietal peritoneum.
-
Peritoneal Mobilization: Gently bluntly dissect the peritoneum from the anterior abdominal wall muscles. This dissection is performed posteriorly and medially, mobilizing the peritoneal sac (containing the intestines) anteriorly and contralaterally. The goal is to avoid perforating the peritoneum. If a small tear occurs, it should be repaired immediately with absorbable suture to prevent herniation of bowel contents and minimize postoperative ileus.

-
Ureter Identification: As the peritoneum is mobilized, identify the ureter. It typically adheres to the posterior aspect of the peritoneum and should be gently swept away with the peritoneal contents, ensuring its continuous visualization or palpation to prevent injury.
Exposure of Lumbar Spine
-
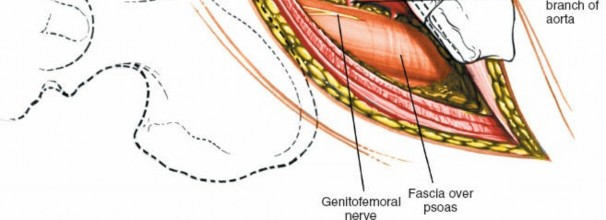
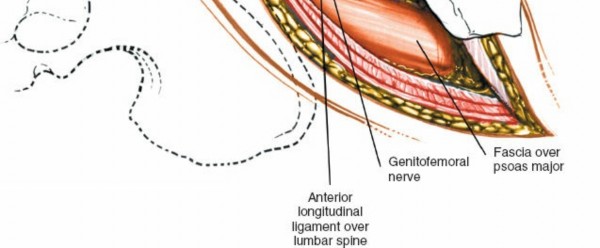
Psoas Muscle Identification: Deep to the peritoneal sac, the psoas major muscle is a prominent landmark, running longitudinally.

-
Sympathetic Chain and Genitofemoral Nerve: The sympathetic chain lies anterolateral to the vertebral bodies, medial to the psoas. The genitofemoral nerve courses on the anterior surface of the psoas muscle. Both should be identified and protected. The sympathetic chain typically does not require mobilization unless directly obstructing exposure.
-
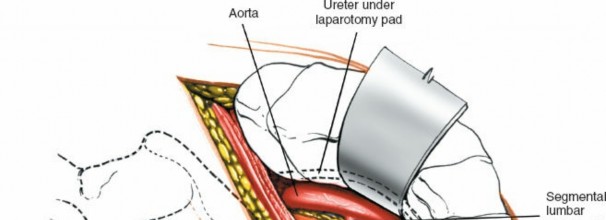
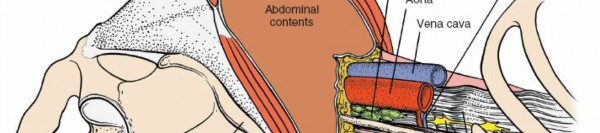
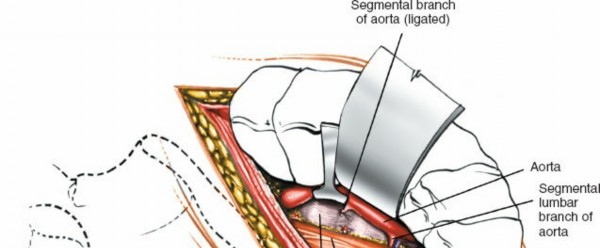
Great Vessel Identification: Once the retroperitoneal fat is cleared, the great vessels—aorta on the left, IVC on the right—become visible, lying on the anterior surface of the vertebral column. Use blunt dissection to separate the great vessels from the anterior longitudinal ligament (ALL).

-
Segmental Vessel Ligation: Segmental lumbar arteries and veins typically course over the middle of the vertebral bodies. For disc space exposure, these vessels need to be ligated and divided. Usually, one pair of segmental vessels per level is encountered. For L5-S1, the middle sacral artery and vein may need ligation. Meticulous hemostasis is paramount. Double ligation with non-absorbable sutures and/or clips is recommended.

-
Retractor Placement: Specialized ALIF retractors (e.g., self-retaining blades) are then placed. The medial blade retracts the great vessels and peritoneal contents, while the lateral blade retracts the psoas and abdominal wall. Ensure no undue tension on the vascular structures or nerves. Confirm the correct spinal level with fluoroscopy.

Disc Space Preparation and Intervention
-
Annulotomy and Discectomy: Incise the anterior longitudinal ligament and the anterior annulus fibrosus using a scalpel. Perform a complete discectomy using rongeurs, pituitary forceps, and curettes. Remove all nuclear material and cartilaginous endplates.
-
Endplate Preparation: Carefully prepare the vertebral endplates. Remove the cartilaginous endplate to expose bleeding bone, which is crucial for promoting fusion. Avoid excessively deep curettage into the bony endplate, which can compromise graft stability and lead to subsidence.


-
Measurement and Trial Implants: Use paddle distractors and trial sizers to determine the appropriate height, width, and lordosis of the interbody cage. Ensure adequate distraction to restore disc height and correct deformity, while avoiding over-distraction.
-
Graft/Cage Insertion: Pack the interbody cage with autograft, allograft, or bone morphogenetic protein (BMP) if permitted and indicated. Insert the chosen interbody device (e.g., PEEK cage, titanium cage, expandable cage, allograft ring) carefully into the prepared disc space. Confirm satisfactory placement and alignment with fluoroscopy.

-
Anterior Plate/Screw Fixation: If additional anterior fixation is desired or required (e.g., for spondylolisthesis reduction, multi-level constructs), an anterior plate may be applied. Ensure screws are of appropriate length and trajectory, avoiding penetration into the spinal canal or adjacent endplates.


Wound Closure
- Hemostasis: Ensure meticulous hemostasis throughout the surgical field, particularly around the great vessels and along the psoas.
- Retractor Removal: Carefully remove the self-retaining retractors.
- Peritoneal Inspection: Inspect the peritoneum for any defects and repair as needed. Allow the peritoneum to fall back into its anatomical position.
-
Muscle Closure: Close the abdominal wall muscle layers anatomically. The transversus abdominis fascia and muscle, then internal oblique, and finally external oblique aponeurosis and muscle. Use interrupted absorbable sutures. This reconstruction is crucial to prevent incisional hernia.

-
Subcutaneous and Skin Closure: Close the subcutaneous fat with absorbable sutures and the skin with appropriate sutures, staples, or adhesive strips. A drain is usually not necessary unless there is significant concern for hematoma or infection.

Complications and Management
Despite its advantages, the anterolateral retroperitoneal approach is not without potential complications, requiring thorough understanding and preparedness for their management.
Vascular Injuries
- Incidence: Varies widely but can be as high as 10-20% for minor vessel injuries (e.g., segmental vessels) and 1-5% for major vessel injury (aorta, IVC, iliacs).
- Mechanism: Direct laceration during dissection, retraction injury, avulsion of segmental vessels, or injury during discectomy or cage insertion. L5-S1 is particularly vulnerable due to the confluence of the common iliac veins.
- Management: Immediate recognition, direct pressure, prompt vascular surgery consultation/repair. Preparedness with vascular clamps, sutures (e.g., Prolene), and vascular bypass grafts is essential. Conversion to open laparotomy may be necessary for complex repairs.
Neurologic Injuries
- Genitofemoral Nerve (GFN):
- Incidence: Up to 10-15%.
- Mechanism: Traction injury during retraction or direct injury during psoas dissection.
- Presentation: Sensory deficit in the anterior thigh (lateral to femoral triangle) and groin region; motor deficit is rare.
- Management: Usually self-limiting; symptomatic treatment for neuropathic pain. Prevention is key through careful identification and protection.
- Femoral Nerve:
- Incidence: Rare (<1%).
- Mechanism: Aggressive lateral retraction of the psoas muscle.
- Presentation: Quadriceps weakness, loss of patellar reflex, sensory deficit in anterior thigh.
- Management: Immediate release of compression, physiotherapy.
- Sympathetic Chain (Hypogastric Plexus):
- Incidence: 1-5% in males.
- Mechanism: Direct injury or excessive cautery during dissection of the great vessels and anterior longitudinal ligament.
- Presentation: Retrograde ejaculation in males (loss of emission due to impaired internal urethral sphincter contraction). Female counterparts are less symptomatic but may experience dry orgasm.
- Management: Prevention by careful dissection and avoidance of electrocautery directly over the sympathetic chain. No effective treatment once established.
Ureteral Injury
- Incidence: Rare (<1%).
- Mechanism: Direct laceration or crush injury during peritoneal mobilization, aggressive retraction, or during closure if entrapped.
- Management: Immediate recognition (e.g., urine leak), urological consultation for primary repair or stenting.
Peritoneal Breach and Ileus
- Incidence: Peritoneal tears: 5-10%. Ileus: 5-15%.
- Mechanism: Accidental perforation of the peritoneal sac during anterior dissection. Postoperative ileus is often multifactorial, including bowel manipulation, anesthesia, and inflammation.
- Management: Small tears should be immediately repaired with absorbable sutures. Larger tears or frank bowel injury necessitates general surgery consultation. Ileus is managed conservatively with bowel rest, nasogastric decompression if necessary, and prokinetics.
Infection
- Incidence: Surgical site infection (SSI) 1-3%. Discitis <1%.
- Mechanism: Contamination during surgery.
- Management: Superficial infections respond to antibiotics. Deep infections or discitis may require debridement, washout, and targeted antibiotics.
Fusion Related Complications
- Nonunion/Pseudarthrosis:
- Incidence: Varies widely (5-20%) depending on patient factors, surgical technique, and follow-up duration.
- Mechanism: Inadequate bony apposition, poor graft vascularity, tobacco use, systemic comorbidities, insufficient anterior column support.
- Management: Revision surgery with additional grafting, decompression, or supplementation with posterior fixation.
- Hardware Failure:
- Incidence: Less common with modern robust instrumentation.
- Mechanism: Pseudarthrosis, poor bone quality, excessive stress on hardware.
- Management: Revision surgery, potentially involving implant removal, re-grafting, and stronger fixation.
- Subsidence:
- Incidence: 5-15%.
- Mechanism: Graft/cage settling into the vertebral endplates, particularly with over-resection of bony endplate, osteoporotic bone, or inadequate initial fixation.
- Management: Mild subsidence may be asymptomatic. Significant subsidence can lead to loss of correction, recurrence of pain, or neuroforaminal stenosis, potentially requiring revision.
Common Complications of Anterolateral Lumbar Approaches
| Complication | Incidence (%) Range | Salvage Strategies / Management Principles |
|---|---|---|
| Vascular Injury | 1-20 (major 1-5) | Immediate direct pressure, vascular surgeon consultation, primary repair, graft interposition. |
| Genitofemoral Nerve Injury | 5-15 | Identification and protection, symptomatic treatment for neuropathic pain. Often self-limiting. |
| Sympathetic Chain Injury | 1-5 (males) | Careful dissection, avoid electrocautery near chain. No specific treatment for retrograde ejaculation. |
| Ureteral Injury | <1 | Immediate identification, urology consultation, primary repair, stenting. |
| Peritoneal Breach | 5-10 | Immediate primary repair of tear to prevent herniation and minimize ileus. |
| Postoperative Ileus | 5-15 | NPO, NGT decompression if needed, prokinetics, judicious fluid management. |
| Surgical Site Infection | 1-3 | Antibiotics (superficial), debridement and washout (deep), culture-guided therapy. |
| Nonunion / Pseudarthrosis | 5-20 | Revision surgery (re-grafting, stronger fixation), biological augmentation. |
| Hardware Failure | <5 | Revision surgery, removal/replacement of hardware, enhanced fusion construct. |
| Graft / Cage Subsidence | 5-15 | Prevention via careful endplate preparation. Revision for symptomatic cases (pain, neurological deficit, recurrent deformity). |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation following an anterolateral retroperitoneal lumbar spine procedure is crucial for promoting fusion, restoring function, and preventing long-term complications. Protocols vary based on the specific procedure (e.g., single-level ALIF vs. multi-level vertebrectomy with plating), bone quality, and patient comorbidities, but general principles apply.
Immediate Postoperative Period (Days 0-7)
- Pain Management: Multimodal analgesia including opioids, NSAIDs (if not contraindicated for fusion), acetaminophen, and nerve blocks to control acute pain and facilitate early mobilization.
- Mobilization: Ambulation initiated on postoperative day 1 or 2, with assistance as needed. Progressive increase in walking distance.
- Bowel Regimen: Early advancement of diet as tolerated. Prophylactic stool softeners and laxatives to prevent constipation and straining, which can increase intra-abdominal pressure.
- Bracing: Typically, a soft lumbar corset is used for comfort and proprioception. Rigid bracing is usually not required for a stable single-level ALIF, but may be considered for multi-level fusions, osteoporotic patients, or complex deformity corrections, often in conjunction with posterior instrumentation.
- Wound Care: Standard wound care. Monitor for signs of infection or hematoma.
- Activity Restrictions: No lifting >5-10 lbs, no bending, no twisting (BLT precautions). Avoid prolonged sitting.
Early Rehabilitation (Weeks 1-6)
- Activity Progression: Gradual increase in ambulation. Light household activities are generally permissible.
- Physical Therapy (PT) Initiation: Focus on postural awareness, gentle core activation (e.g., diaphragmatic breathing, transverse abdominis contractions), and gentle range of motion exercises for hips and shoulders. Avoid aggressive stretching or spinal loading.
- Cardiovascular Fitness: Low-impact activities such as stationary biking (upright position) or elliptical training can be introduced once pain is controlled.
- Pain Management: Transition from opioid to non-opioid analgesia.
Mid Rehabilitation (Months 2-4)
- Progressive Core Strengthening: Supervised physical therapy focusing on progressive core stability exercises (planks, bird-dog, pelvic tilts) and strengthening of gluteal and hip musculature. Avoid full sit-ups or aggressive rotational movements.
- Gradual Increase in Activity: Return to more demanding daily activities. Light stretching and flexibility exercises for the hamstrings and hip flexors.
- Fusion Assessment: First radiographic follow-up (plain films) typically at 6 weeks and 3 months to assess graft position and early signs of fusion.
- Weight Bearing: Gradual progression of weight-bearing exercises.
Late Rehabilitation (Months 4-12+)
- Return to Activity/Sport Specific Training: Once radiographic signs of fusion are evident (typically 6-12 months), a gradual return to higher impact activities and sports can be considered, based on clinical judgment and patient's functional status. This phase often involves sports-specific conditioning and strengthening.
- Long-Term Spinal Health: Emphasis on maintaining core strength, proper body mechanics, and a healthy lifestyle to prevent adjacent segment pathology and recurrence of symptoms.
- Radiographic Follow-up: Periodic radiographs (e.g., at 6 months, 1 year, 2 years) to monitor fusion progression and overall spinal alignment. A CT scan may be indicated if there is suspicion of nonunion despite clinical improvement.
Summary of Key Literature and Guidelines
The anterolateral retroperitoneal approach to the lumbar spine is well-established, supported by a significant body of literature demonstrating its efficacy and defining its role in modern spinal surgery.
Numerous studies have highlighted the advantages of the retroperitoneal approach, particularly for ALIF procedures. Meta-analyses and systematic reviews comparing ALIF to posterior lumbar interbody fusion (PLIF) or transforaminal lumbar interbody fusion (TLIF) have generally shown ALIF to achieve higher fusion rates, especially when supplemented with posterior fixation, due to the larger graft footprint and direct anterior column support. ALIF has also been demonstrated to be superior in restoring disc height and lumbar lordosis, which are critical for optimal sagittal balance. However, these benefits must be weighed against the unique complication profile, particularly vascular and sympathetic nerve injuries.
Key Findings from Literature:
* Fusion Rates: ALIF with or without posterior instrumentation consistently demonstrates high fusion rates, often exceeding 90%. The larger graft-endplate interface, coupled with robust anterior fixation, contributes to superior biomechanical stability.
* Restoration of Sagittal Parameters: ALIF is highly effective in restoring segmental lordosis and correcting sagittal imbalance, which is challenging to achieve solely with posterior approaches. This is particularly relevant in adult spinal deformity correction.
* Minimally Invasive ALIF (MIS-ALIF): Advancements in instrumentation and technique have led to the development of MIS-ALIF, utilizing smaller incisions and specialized retractors. While potentially reducing soft tissue dissection and blood loss, MIS-ALIF still requires a skilled access surgeon and carries similar vascular risks.
* Comparison to Lateral Approaches (DLIF/XLIF): While lateral approaches offer advantages for indirect decompression and deformity correction, they involve dissection through the psoas muscle, with associated risks to the lumbar plexus (e.g., transient thigh weakness, numbness). The direct anterior retroperitoneal approach avoids traversing the psoas, potentially reducing these specific neurological complications, though it has its own unique set of vascular and sympathetic risks.
* L5-S1 Considerations: The vascular anatomy at L5-S1 (iliac bifurcation, crossing left iliac vein) often makes this level the most challenging from a retroperitoneal perspective. The presence of a vascular access surgeon is often recommended for this level.
Guidelines and Recommendations:
* Multidisciplinary Approach: Current best practices advocate for a multidisciplinary team approach, particularly for complex cases, involving spinal surgeons, vascular surgeons (for L5-S1 and revisions), and pain management specialists.
* Preoperative Imaging: Detailed preoperative imaging, including CT angiogram for vascular mapping, is a standard recommendation to identify anatomical variations and plan the safest approach.
* Sympathetic Chain Preservation: Emphasis is placed on meticulous dissection and judicious use of electrocautery to minimize the risk of sympathetic chain injury and subsequent retrograde ejaculation.
* Thorough Hemostasis: Meticulous attention to hemostasis, especially during segmental vessel ligation, is critical to prevent hematoma formation and associated complications.
* Surgeon Experience: The anterolateral retroperitoneal approach is technically demanding, and outcomes are highly dependent on the experience of the surgical team. Training in accredited centers and mentorship are crucial for surgeons learning this technique.
In conclusion, the anterolateral retroperitoneal approach to the lumbar spine remains a powerful and effective technique for addressing a wide array of anterior column pathologies. Its proven ability to achieve high fusion rates, restore sagittal balance, and decompress neural elements makes it an invaluable tool in the spinal surgeon's repertoire. Continued refinement of surgical techniques, advanced imaging, and a collaborative multidisciplinary approach will further enhance its safety and efficacy.
Clinical & Radiographic Imaging


You Might Also Like