Expert Guide: Transperitoneal and Retroperitoneal Lumbar Access
Key Takeaway
This topic focuses on Expert Guide: Transperitoneal and Retroperitoneal Lumbar Access, The anterior approach to the lumbar spine employs both **transperitoneal and retroperitoneal** techniques, mainly for L5-S1 fusion. It also addresses L4-L5 fusions (requiring great vessel mobilization), spinal tuberculosis, and disc prosthesis insertion. This surgical method provides direct access to the lumbar vertebrae through an abdominal incision, with general surgeon assistance often recommended due to familiarity with the exposed anatomical region.
Expert Guide: Transperitoneal and Retroperitoneal Lumbar Access
Introduction and Epidemiology
Anterior approaches to the lumbar spine, encompassing both transperitoneal and retroperitoneal techniques, represent fundamental surgical corridors for addressing a wide spectrum of spinal pathologies. These approaches offer direct access to the anterior column, enabling comprehensive discectomy, endplate preparation, restoration of disc height and lumbar lordosis, and robust anterior column support, which are critical for achieving stable fusion and optimizing sagittal balance. Historically, these techniques have been invaluable for managing conditions such as spinal tuberculosis and complex deformities. In contemporary spinal surgery, their utility extends to degenerative disc disease, spondylolisthesis, post-laminectomy syndrome, trauma, tumor resection, and the placement of interbody prostheses.
The choice between a transperitoneal and retroperitoneal approach is predicated on the specific spinal levels targeted, patient anatomy, and surgeon preference. The retroperitoneal approach is generally favored for levels L2-S1, particularly L4-5 and L5-S1, due to its direct trajectory to the anterior spinal column without violating the peritoneal cavity. The transperitoneal approach, while providing excellent access to all lumbar levels, involves traversing the peritoneal cavity and often requires mobilization of intra-abdominal contents, carrying a distinct set of considerations and potential complications. Both approaches necessitate a thorough understanding of abdominal and retroperitoneal anatomy, meticulous surgical technique, and often a multidisciplinary team approach involving a general or vascular surgeon for access. The increasing complexity of spinal pathologies, coupled with advancements in surgical instrumentation and fusion technologies, has solidified the anterior lumbar interbody fusion (ALIF) procedure as a cornerstone in the armamentarium of the orthopedic spinal surgeon.
Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy is paramount for safe and effective anterior lumbar spine surgery. This encompasses the abdominal wall, visceral contents, major vascular structures, and the autonomic nervous system.
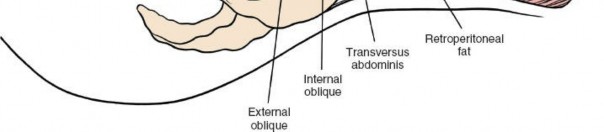
Abdominal Wall Anatomy
The abdominal wall consists of several muscular layers: the rectus abdominis, external oblique, internal oblique, and transversus abdominis. These muscles are segmentally innervated by the T7-T12 intercostal nerves. The rectus abdominis muscles are separated by the linea alba in the midline. The posterior rectus sheath terminates inferiorly at the arcuate line, below which the rectus abdominis lies directly on the transversalis fascia. The internervous plane of a midline incision passes between the bilateral rectus abdominis muscles, allowing for extensive exposure from the xiphisternum to the pubic symphysis without denervation of the abdominal musculature. For retroperitoneal approaches, muscle-splitting or retraction techniques are employed, typically preserving nerve and muscle integrity.
Visceral Anatomy
The peritoneal cavity contains the small and large intestines. In a transperitoneal approach, these contents must be carefully mobilized and retracted. The retroperitoneal space lies posterior to the peritoneum and contains the kidneys, ureters, pancreas, duodenum, major vascular structures (aorta, vena cava, iliac arteries and veins), and lumbar sympathetic chain.
Vascular Anatomy
The great vessels are critical structures. The abdominal aorta typically bifurcates into the common iliac arteries at the L4-L5 disc space, though this can vary from L3 to S1. The inferior vena cava (IVC) lies to the right of the aorta and is formed by the confluence of the common iliac veins, usually at L5-S1. The common iliac vessels further bifurcate into external and internal iliac arteries and veins. The left common iliac vein typically courses posterior to the right common iliac artery and left common iliac artery, making it particularly vulnerable to injury at the L4-5 and L5-S1 levels. Lumbar segmental arteries and veins originate from the posterior aspects of the aorta and IVC, respectively, and must be carefully ligated or coagulated to prevent significant hemorrhage. Preoperative vascular imaging is crucial for identifying anatomical variants and planning vessel mobilization.
Neural Anatomy
The lumbar sympathetic chain runs anterior to the psoas muscle, medial to the ureter, and lateral to the great vessels. Injury to these ganglia, particularly at L4-5 and L5-S1, can lead to retrograde ejaculation in males (due to bilateral injury) or sudomotor dysfunction. The genitofemoral nerve, a branch of the lumbar plexus, courses anterior to the psoas muscle and is susceptible to injury during lateral dissection in the retroperitoneal space. The ureters lie within the retroperitoneal space, crossing the common iliac vessels, and must be identified and protected.
Biomechanical Considerations
Anterior column support is biomechanically advantageous for lumbar fusion. The anterior column bears approximately 80% of the axial load. By restoring disc height and implanting a large footprint cage into the anterior column, ALIF procedures provide immediate structural stability, promote optimal load sharing across the fusion construct, and facilitate indirect decompression of neural elements. This approach also allows for restoration of lumbar lordosis, which is vital for achieving favorable sagittal balance and preventing adjacent segment disease.
Indications and Contraindications
The anterior approach to the lumbar spine is indicated for a range of degenerative, traumatic, neoplastic, and infectious conditions that benefit from direct anterior column access and reconstruction.
Indications for Anterior Lumbar Interbody Fusion
- Degenerative Disc Disease (DDD): Particularly at L4-L5 and L5-S1, refractory to conservative management, presenting with mechanical low back pain or radiculopathy.
- Spondylolisthesis: Low-grade degenerative or isthmic spondylolisthesis (Grade I or II) where reduction and fusion are desired. ALIF offers robust anterior column support and indirect decompression.
- Spinal Deformity: Correction of sagittal imbalance (e.g., flatback syndrome) or restoration of lordosis. Long-segment fusions often incorporate ALIF at specific levels to achieve kyphosis correction.
- Post-Laminectomy Syndrome: Revision surgery for persistent back pain, pseudarthrosis, or recurrent disc herniation following posterior decompression.
- Spinal Trauma: Stabilization of burst fractures or fracture-dislocations with anterior column compromise, often in conjunction with posterior fixation.
- Spinal Tumor Resection: Decompression of the spinal canal and reconstruction of the anterior column following corpectomy for metastatic or primary tumors.
- Spinal Infection: Debridement and fusion for discitis or osteomyelitis (e.g., spinal tuberculosis) where infected material needs to be removed from the anterior column.
- Pseudarthrosis: Salvage of failed posterior or posterolateral fusions.
- Disc Prostheses: As noted in the original content, anterior access is essential for total disc replacement.
Contraindications
- Absolute Contraindications:
- Severe active infection not controlled by antibiotics.
- Severe cardiopulmonary compromise precluding safe general anesthesia.
- Severe coagulopathy that cannot be corrected.
- Anatomical impediments: e.g., significant atherosclerotic disease (aortic aneurysm, severely calcified vessels), previous extensive abdominal surgery with dense adhesions (though not always absolute, increases risk).
- Relative Contraindications:
- Morbid obesity (can increase technical difficulty and complication rates).
- History of multiple previous abdominal surgeries (increases risk of adhesions, bowel injury).
- Inflammatory bowel disease (relative contraindication for transperitoneal approach due to risk of bowel manipulation exacerbation).
- Active abdominal wall hernia at the intended incision site.
- Severe osteoporosis (may compromise implant anchorage).
- Lack of appropriately experienced access surgeon (vascular or general surgeon).
Table 1: Operative vs. Non-Operative Indications for Lumbar Spine Pathologies
| Pathology | Operative Indications (Anterior Approach) | Non-Operative Management |
|---|---|---|
| Degenerative Disc Disease | Refractory axial back pain or radiculopathy, disc height loss, sagittal imbalance | Physical therapy, NSAIDs, epidural injections, activity modification |
| Spondylolisthesis (Grade I/II) | Progressive neurological deficit, intractable pain, segmental instability | Physical therapy, bracing, NSAIDs, pain management |
| Spinal Deformity | Progressive deformity, intractable pain, neurological compromise, sagittal imbalance | Observation, bracing for minor curves, physical therapy |
| Trauma (Burst Fracture) | Neurological deficit, significant canal compromise, instability, kyphosis | Non-displaced stable fractures, bracing, pain management |
| Tumor | Spinal cord compression, intractable pain, instability, tissue diagnosis | Palliative care, radiation therapy for radiosensitive tumors |
| Infection (Discitis/Osteo) | Neurological deficit, abscess formation, spinal instability, failed conservative treatment | Antibiotic therapy, bracing, rest |
| Pseudarthrosis | Persistent intractable pain, demonstrable instability on dynamic imaging | Pain management, activity modification, re-evaluation |
Pre Operative Planning and Patient Positioning
Comprehensive preoperative planning is fundamental to minimize complications and optimize outcomes in anterior lumbar surgery. This includes thorough patient evaluation, diagnostic imaging review, and meticulous surgical setup.
Patient Evaluation and Optimization
A detailed history and physical examination are essential. Co-morbidities such as cardiovascular disease, diabetes, and pulmonary dysfunction should be optimized. Smoking cessation is strongly encouraged to improve fusion rates. Patients on anticoagulants or antiplatelet medications require a specific management plan. Consultation with a vascular or general surgeon for access is mandatory for almost all cases to ensure safe vessel mobilization and minimize visceral complications.
Diagnostic Imaging Review
High-resolution imaging is crucial. MRI provides detailed information regarding disc degeneration, neural element compression, and soft tissue pathologies. CT scans are essential for assessing bony anatomy, facet arthrosis, canal stenosis, and implant planning. For vascular assessment, a CT angiogram (CTA) or MRA is highly recommended to delineate the course of the great vessels, identify anomalies (e.g., retro-aortic left renal vein), assess for significant atherosclerotic disease, and map the lumbar segmental vessels. This allows the surgical team to anticipate potential difficulties in vessel mobilization and identify levels at increased risk of vascular injury.
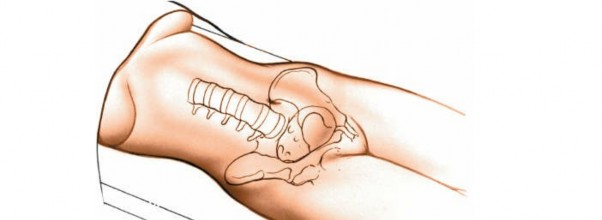
Patient Positioning
The patient is typically positioned supine on a radiolucent operating table. For most ALIF procedures, a slight Trendelenburg position can aid in retraction of the abdominal viscera (transperitoneal approach) or lower the diaphragm (retroperitoneal approach). Proper padding of pressure points is crucial to prevent nerve palsies or skin breakdown. A bolster or gel roll beneath the lumbar spine can aid in maximizing lumbar lordosis and facilitating cage insertion, though this must be balanced with adequate abdominal relaxation. The patient's arms are usually tucked at their sides.
As noted in the original content, for cases involving autograft harvest, ensure two areas remain bare: one for the abdominal incision and one for the anterior iliac crest bone graft.
A urinary catheter is inserted to keep the bladder empty, facilitating pelvic dissection and minimizing the risk of bladder injury.
Prophylaxis for venous thromboembolism (VTE) is critical. This typically involves mechanical calf compression devices (sequential compression devices or SCDs) intraoperatively and postoperatively, often supplemented by chemical prophylaxis (e.g., low molecular weight heparin) based on patient risk factors and institutional protocols.
Intraoperative Imaging
Fluoroscopy or intraoperative navigation is essential to confirm the correct spinal level before incision and throughout the procedure, particularly during discectomy and cage placement. Anteroposterior and lateral views are routinely used.
Detailed Surgical Approach and Technique
The anterior approach to the lumbar spine can be broadly categorized into transperitoneal and retroperitoneal techniques. While both aim to access the anterior vertebral column, their entry points and dissection planes differ significantly.
Landmarks and Incision
Accurate identification of anatomical landmarks is paramount for precise incision placement and efficient dissection.
Landmarks
The umbilicus is typically opposite the L3-4 disc space, but its exact level is variable, influenced by patient body habitus. The pubic symphysis is palpable at the inferior aspect of the abdomen. The pubic tubercle, just lateral to the midline on the superior border of the pubis, can be a more distinct landmark than the superior symphysis. For L5-S1 access, a low transverse incision, often referred to as a Pfannenstiel or modified Pfannenstiel incision, is commonly employed, centered roughly 2-3 cm superior to the pubic symphysis. For higher lumbar levels (L2-3, L3-4, L4-5), a paramedian or oblique incision may be preferred to optimize working angles and reduce retraction.
Incision
The choice of incision depends on the level(s) to be addressed and the surgeon's preference.
- Midline Incision: Extending from the xiphisternum to the pubic symphysis, this incision utilizes the internervous plane between the rectus abdominis muscles. It provides excellent exposure for multiple lumbar levels but involves a transperitoneal approach.
- Transverse Incision (Pfannenstiel type): Typically used for L5-S1, this low transverse incision is made just above the pubic hairline. It offers good cosmesis and can be used for both transperitoneal and retroperitoneal approaches depending on the depth of dissection.
- Paramedian/Oblique Incision: Often made curvilinearly from the rectus border towards the anterior superior iliac spine, this incision can be tailored for single or multiple levels. It facilitates a retroperitoneal approach to higher lumbar levels.
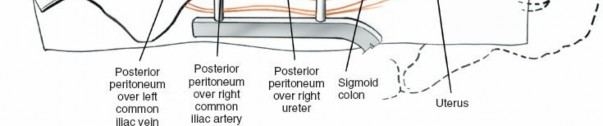
Figure 1: Incision planning, often low transverse or oblique depending on levels and approach.
Transperitoneal Approach
This approach provides a direct view of the anterior lumbar spine and is generally preferred for higher lumbar levels or when extensive exploration of the abdominal contents is required.
Skin and Subcutaneous Dissection
The skin and subcutaneous fat are incised. Electrocautery is used for hemostasis.
Rectus Sheath and Muscle
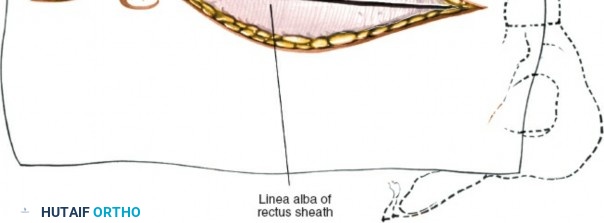
The anterior rectus sheath is incised. The rectus abdominis muscle is retracted laterally. The posterior rectus sheath and transversalis fascia are incised to enter the peritoneal cavity.
Peritoneal Entry and Visceral Mobilization
Once the peritoneal cavity is entered, the small bowel and colon are carefully identified. The bowel is mobilized and retracted cephalad, often using moist laparotomy sponges and a self-retaining retractor system. This provides exposure to the posterior peritoneum overlying the great vessels and lumbar spine.

Figure 2: Schematic showing layered abdominal wall dissection for transperitoneal access.
Retroperitoneal Approach
The retroperitoneal approach is generally favored for L4-S1 access due to its direct path to the great vessels and vertebral bodies without entering the peritoneal cavity. It typically involves a more lateral, oblique incision.
Skin and Subcutaneous Dissection
An oblique incision, often parallel to the inguinal ligament or a curvilinear paramedian incision, is made.

Figure 3: Initial skin incision for a retroperitoneal approach, typically oblique or low transverse.
Muscle Splitting/Retraction
The external oblique, internal oblique, and transversus abdominis muscles are successively incised or split in the direction of their fibers, or bluntly dissected. Care is taken to identify and preserve the iliohypogastric and ilioinguinal nerves.
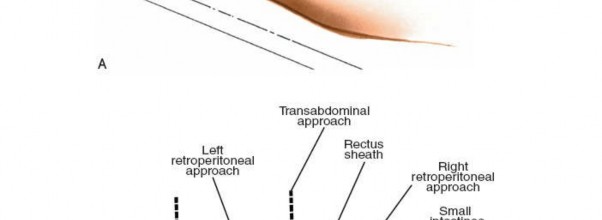
Figure 4: Dissection through the oblique muscle layers for retroperitoneal access.
Retroperitoneal Space Entry
Once the transversus abdominis is traversed, the transversalis fascia is encountered. This is carefully incised, and the retroperitoneal fat is bluntly swept anteriorly and medially, pushing the peritoneum and its contents away from the posterior abdominal wall. This dissection proceeds directly towards the psoas muscle, medial to the ureter.

Figure 5: Blunt dissection into the retroperitoneal space, sweeping the peritoneum medially.
Exposure of the Great Vessels and Lumbar Spine (Common to both approaches after initial entry)
Identification of Key Structures
The ureter is the first critical structure to identify. It crosses the common iliac vessels and must be protected. It is usually adherent to the medialized peritoneum. The psoas muscle, the genitofemoral nerve on its anterior surface, and the iliac vessels are then identified.
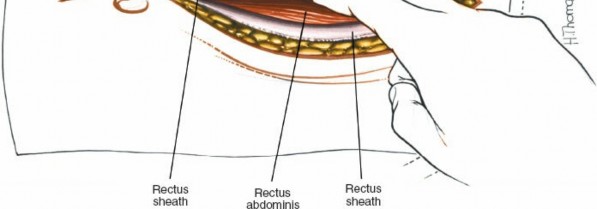
Figure 6: Identifying the ureter (often retracted with the peritoneum) and accessing the great vessels.
The aorta (left) and IVC (right) are the dominant structures. The common iliac arteries and veins are traced caudally. The left common iliac vein is particularly vulnerable at L4-5 and L5-S1.
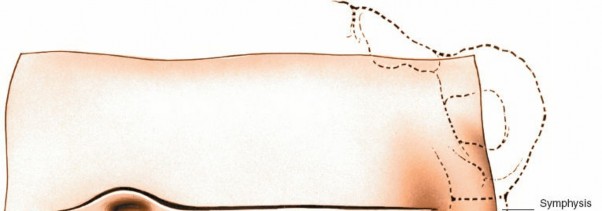
Figure 7: Exposure of the great vessels (aorta and IVC) and their bifurcations.
Vessel Mobilization
Under the guidance of the access surgeon, the great vessels are carefully mobilized to expose the anterior aspect of the disc space. Lumbar segmental arteries and veins, which supply the vertebral body, typically arise from the posterior aspect of the great vessels. These vessels must be identified, ligated (with clips or sutures), and divided to allow for safe retraction of the main vessels.

Figure 8: Careful mobilization of the great vessels, often requiring ligation of segmental vessels.
The vessel retraction technique varies:
* For L5-S1, the left common iliac vein and artery are retracted to the left. The median sacral artery and vein may need to be ligated.
* For L4-5, the left common iliac vein is often the most challenging. The iliolumbar vein, which drains into the common iliac vein, may also need to be ligated.
* For higher levels, direct retraction of the aorta and IVC is performed, often retracting the aorta to the left and IVC to the right. The lumbar sympathetic chain, lying anterior to the psoas and lateral to the great vessels, is identified and protected.

Figure 9: Further retraction of vessels to expose the disc space, showing segmental vessel ligation.
Disc Space Preparation and Fusion
Once the disc space is adequately exposed, the orthopedic surgeon takes over for the spinal procedure.
Annulotomy and Discectomy
An annulotomy is performed to access the disc. The anterior longitudinal ligament is incised. A complete discectomy is then performed using rongeurs, curettes, and pituitary instruments. All disc material, including cartilaginous endplates, must be removed to prepare the vertebral endplates for fusion.
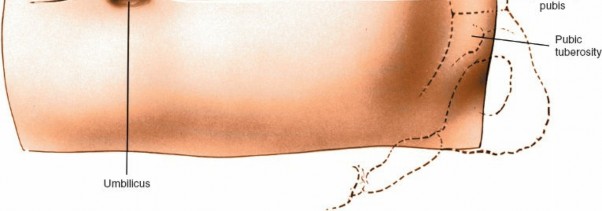
Figure 10: Incision of the anterior annulus fibrosus to access the disc space.
Endplate Preparation
Careful preparation of the vertebral endplates is critical for fusion. The cortical bone of the endplates is preserved while removing the cartilaginous layer. This exposes the bleeding cancellous bone, which is essential for bony ingrowth into the interbody implant.

Figure 11: Discectomy in progress, removing disc material and preparing endplates.
Restoration of Disc Height and Lordosis
Distractors are used to restore disc height and realign the vertebral bodies. This maneuver also indirectly decompresses the neural elements. Trial cages are used to determine the optimal cage size and lordotic angle.
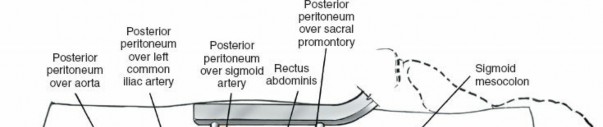
Figure 12: Preparation of the vertebral endplates, removing cartilage to expose cancellous bone.

Figure 13: Using specialized instruments to decorticate and prepare endplates for optimal fusion.
Interbody Cage Insertion
The chosen interbody cage, typically made of PEEK, titanium, or a combination, is packed with autograft, allograft, or bone graft substitute. The cage is then carefully impacted into the prepared disc space. The design of the cage (e.g., lordotic angle, size, surface features) is chosen to match the anatomical requirements and biomechanical goals.
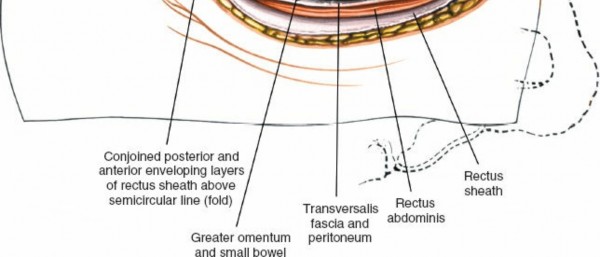
Figure 14: Insertion of the interbody fusion cage into the prepared disc space.
Supplemental Fixation
Depending on the cage design, supplemental fixation may be achieved with anterior plating, integrated screws within the cage, or posterior pedicle screw instrumentation. Anterior plating provides additional rotational and translational stability.

Figure 15: An anterior plate being secured to the vertebral bodies following cage placement.

Figure 16: Final anterior construct with cage and plate providing stable fixation.
Closure
Once the spinal procedure is complete and hemostasis is achieved, the access surgeon meticulously closes the wound.
* Vessel Repositioning: The great vessels are carefully returned to their anatomical position.
* Peritoneal/Retroperitoneal Closure: In a transperitoneal approach, the peritoneum is closed. In a retroperitoneal approach, the transversalis fascia is re-approximated.
* Muscle and Fascial Closure: The muscle layers and fascial planes (e.g., rectus sheath) are meticulously closed in layers with absorbable sutures to prevent herniation.
* Skin Closure: Subcutaneous tissues and skin are closed. A drain may be placed in the retroperitoneal space if significant oozing is anticipated or if there was substantial vessel manipulation.

Figure 17: Close-up of the surgical field during closure, ensuring hemostasis.

Figure 18: Layered closure of the abdominal wall after completing the spinal portion.

Figure 19: Image depicting the final layered closure of the incision.

Figure 20: Example of suture placement during fascial or muscle layer closure.

Figure 21: Another view of the abdominal wall layers during re-approximation.
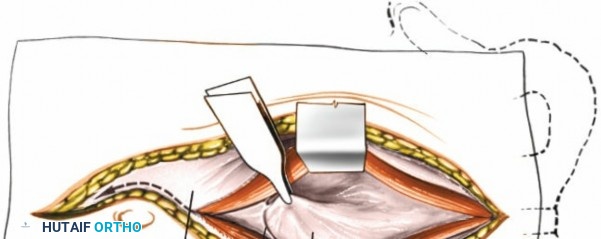
Figure 22: Final superficial closure after deep layers are secured.
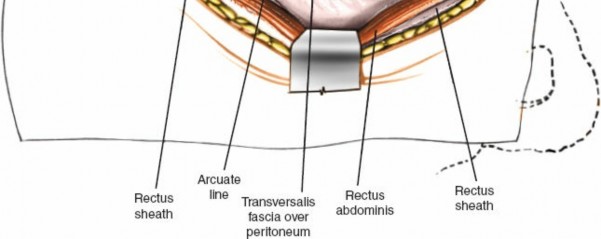
Figure 23: Potential drain placement, if indicated, prior to final skin closure.

Figure 24: Another view of the surgical site, possibly during irrigation or final check.

Figure 25: Detail of a ligated vessel or a hemostatic maneuver during wound closure.

Figure 26: The surgical field just before the final skin closure.

Figure 27: Final appearance of the closed incision.
Complications and Management
While anterior lumbar approaches offer distinct advantages, they are associated with a unique set of potential complications, predominantly due to the close proximity to vital neurovascular and visceral structures. Proactive recognition and management are key.
Table 2: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Vascular Injury | 1-15% (minor), <1% (major) | Immediate vascular repair (suture, patch graft), blood transfusion, emergent laparotomy. Preventative: CTA, access surgeon. |
| Retrograde Ejaculation | 1-30% (males) | Education and counseling. Typically transient, but can be permanent. No direct surgical salvage. |
| Ureteral Injury | <0.5% | Intraoperative recognition and primary repair over a stent. Postoperative: nephrostomy, ureteral reimplantation. |
| Bowel Injury/Ileus | 1-5% (ileus), <0.5% (injury) | Ileus: NPO, NGT, prokinetics. Injury: Primary repair, bowel resection, colostomy. Preventative: careful retraction. |
| Nerve Injury | <1% (sympathetic chain, genitofemoral) | Sympathetic: Conservative for pain. Genitofemoral: Exploration and neurolysis/repair for severe symptoms. |
| Infection | <1% (deep), 1-5% (superficial) | Antibiotics (IV, oral), wound debridement, hardware removal (if persistent), drain placement. |
| Thromboembolism (DVT/PE) | 1-5% (without prophylaxis) | Anticoagulation (heparin, warfarin, DOACs). Preventative: SCDs, chemical prophylaxis. |
| Hernia (incisional) | 1-10% | Surgical repair (mesh hernioplasty). Preventative: meticulous fascial closure. |
| Pseudarthrosis | 5-15% | Revision surgery (re-fusion, posterior augmentation), bone stimulator. |
| Implant Malposition/Failure | <5% | Revision surgery (implant repositioning, exchange, additional fixation). |
| Bladder Injury | Rare | Primary repair, Foley catheter for 7-10 days. |
Vascular Injuries
This is arguably the most feared complication, potentially life-threatening. Injuries can range from minor tears to catastrophic ruptures of the aorta, IVC, or iliac vessels. The left common iliac vein is particularly vulnerable at L4-5 and L5-S1 due to its posterior course to the right common iliac artery.
* Management: Immediate recognition, direct pressure, rapid conversion to open exposure (if not already open), vascular repair by the access surgeon (primary repair, patch angioplasty, or rarely graft interposition). Adequate blood products must be readily available. Prevention relies on meticulous preoperative vascular imaging and experienced access surgeon involvement.
Retrograde Ejaculation
Predominantly affecting males, this occurs due to bilateral injury or disruption of the superior hypogastric plexus and/or lumbar sympathetic chain, which are crucial for bladder neck closure during ejaculation.
* Management: It is usually transient but can be permanent. Prevention involves careful blunt dissection, especially at L5-S1, staying strictly midline anterior to the disc space, and avoiding aggressive lateral electrocautery. Counseling patients preoperatively about this risk is essential.
Ureteral Injury
The ureters lie within the retroperitoneal space and can be inadvertently damaged during dissection or retraction.
* Management: Intraoperative identification and protection are key. If injured, primary repair over a stent is the preferred management. Postoperative recognition may require percutaneous nephrostomy, stent placement, or ureteral reimplantation.
Bowel Injury and Ileus
Bowel injury is a rare but serious complication, more common with transperitoneal approaches or extensive lysis of adhesions. Postoperative ileus is more common, especially after significant bowel manipulation.
* Management: Bowel injury requires immediate surgical repair. Postoperative ileus is typically managed conservatively with nil per os (NPO), nasogastric tube decompression, and prokinetics if necessary.
Neurological Injuries
- Lumbar Sympathetic Chain: As discussed, injury can lead to retrograde ejaculation in males. Unilateral injury may cause ipsilateral lower extremity anhidrosis, warmth, and flushing, typically transient.
- Genitofemoral Nerve: Can be stretched or compressed during lateral retroperitoneal dissection, leading to sensory changes (numbness, dysesthesia) in the anterior thigh. Rarely requires surgical intervention.
Incisional Hernia
A weakness in the abdominal wall closure can lead to an incisional hernia, particularly if fascial closure is not meticulous or if wound healing is impaired.
* Management: Surgical repair, often with mesh.
Infection
Deep space infection (disc space, retroperitoneal space) is rare but devastating. Superficial wound infections are more common.
* Management: Deep infections require aggressive debridement, IV antibiotics, and potentially implant removal. Superficial infections typically respond to oral antibiotics and local wound care.
Pseudarthrosis and Implant-Related Complications
Failure to achieve solid fusion (pseudarthrosis) can occur, necessitating revision surgery. Implant-related issues include malposition, subsidence, or loosening.
* Management: Pseudarthrosis often requires revision with further fusion, sometimes with supplemental posterior fixation. Implant-related issues may necessitate reoperation for adjustment or exchange.
Post Operative Rehabilitation Protocols
A structured rehabilitation protocol is crucial for optimizing patient recovery, promoting fusion, and preventing complications after anterior lumbar surgery. The goals are early mobilization, pain control, core strengthening, and gradual return to activities.
Immediate Postoperative Period (Days 0-7)
- Pain Management: Multimodal analgesia, including epidural catheters, patient-controlled analgesia (PCA), oral opioids, NSAIDs (if not contraindicated), and muscle relaxants.
- Mobilization: Ambulation is encouraged on postoperative day 1. Early mobilization helps prevent VTE, muscle atrophy, and pulmonary complications.
- Activity Restrictions: Strict lifting restrictions (typically <10 lbs/4.5 kg), avoidance of excessive twisting or bending.
- Bracing: A lumbar orthosis (brace) may be prescribed, depending on the number of levels fused, quality of bone, and presence of supplemental posterior fixation. For robust, single-level ALIF, bracing is often optional.
- Wound Care: Routine wound care, monitoring for signs of infection or hematoma. Drain removal usually when output is minimal.
- Bowel Management: Monitoring for ileus, gradual advancement of diet as tolerated. Stool softeners and laxatives are often prescribed.
Early Recovery Phase (Weeks 2-6)
- Activity Progression: Gradual increase in ambulation distance and duration. Light household activities are typically permitted.
- Physical Therapy (PT): May initiate a gentle core stabilization program, focusing on isometric exercises. Avoidance of spinal flexion, extension, and rotation. Emphasis on proper body mechanics.
- Pain Management: Transition from opioid to non-opioid pain medications as tolerated.
- Driving: Typically allowed after 2-4 weeks, provided pain is controlled and patients are off narcotic medications.
Intermediate Recovery Phase (Months 2-4)
- Physical Therapy: Progression to more active core strengthening, balance, and proprioception exercises. Low-impact aerobic activities (walking, stationary bike) are encouraged.
- Return to Work: Sedentary work may resume within 6-8 weeks. Light-duty work with limited lifting may be possible by 3-4 months.
- Radiographic Assessment: Follow-up radiographs (AP and lateral) are typically obtained at 3 months to assess for early signs of fusion and implant position. Dynamic flexion-extension views may be considered if pseudarthrosis is suspected.
Advanced Rehabilitation (Months 4-12+)
- Physical Therapy: Continued progression of strengthening exercises, incorporating functional movements. Gradual return to recreational activities.
- Sport-Specific Training: For athletes, a supervised, progressive return to sport-specific drills and training.
- Radiographic Assessment: Final fusion assessment typically at 6-12 months using CT scan if plain radiographs are inconclusive.
- Full Activity: Most patients can return to full activities, including sports, by 9-12 months, once solid fusion is confirmed and strength is regained. High-impact activities may be modified.
Throughout all phases, patient education regarding proper body mechanics, activity modification, and adherence to the rehabilitation program is paramount for achieving optimal long-term outcomes and minimizing the risk of re-injury or adjacent segment pathology.
Summary of Key Literature and Guidelines
The anterior lumbar approach, particularly ALIF, has a well-established evidence base in the orthopedic and neurosurgical literature. Numerous studies have demonstrated its efficacy in achieving high fusion rates, restoring disc height and lumbar lordosis, and providing significant clinical improvement for a variety of lumbar spinal pathologies.
- Fusion Rates: ALIF typically boasts high fusion rates, often exceeding 90-95%, which are comparable to or superior to posterior or posterolateral approaches, especially with the use of modern interbody cages and biological augmentation. The large surface area for fusion and robust anterior column support contribute to this success.
- Sagittal Balance Restoration: A distinct advantage of ALIF is its ability to restore lumbar lordosis and improve sagittal balance, which is increasingly recognized as a critical determinant of long-term outcomes and prevention of adjacent segment disease. Lordotic cages play a pivotal role in this correction.
- Indirect Decompression: By restoring disc height, ALIF can achieve indirect decompression of neural elements, including the neural foramina, without direct posterior laminectomy or facetectomy, thus minimizing iatrogenic instability.
- Minimally Invasive ALIF (MIS-ALIF): Advancements in surgical techniques have led to the development of minimally invasive ALIF approaches, often using smaller incisions and specialized retractors. These techniques aim to reduce surgical morbidity, blood loss, and length of hospital stay while maintaining the benefits of open ALIF. Endoscopic and robotic-assisted transperitoneal approaches have been described but remain niche and require further validation in routine practice.
- Multidisciplinary Approach: Consensus guidelines from professional organizations like the North American Spine Society (NASS) and the American Academy of Orthopaedic Surgeons (AAOS) emphasize the importance of a multidisciplinary approach, particularly the mandatory involvement of an experienced access surgeon (general or vascular surgeon) for anterior lumbar access to minimize visceral and vascular complications.
- Outcomes Data: Long-term follow-up studies consistently show durable clinical outcomes in appropriately selected patients undergoing ALIF, with sustained pain relief and functional improvement. Comparison studies often highlight reduced paraspinal muscle injury and potentially faster initial recovery compared to purely posterior approaches, though this must be weighed against the specific risks associated with anterior abdominal access.
In conclusion, the transperitoneal and retroperitoneal anterior approaches to the lumbar spine remain indispensable tools for the modern orthopedic spine surgeon. A comprehensive understanding of the indications, contraindications, detailed surgical anatomy, meticulous technique, and potential complications, coupled with a commitment to evidence-based practice and multidisciplinary collaboration, ensures optimal patient care and outcomes.
Clinical & Radiographic Imaging


You Might Also Like