Anterior Retroperitoneal Approach for Lumbar Spine Surgery: A Comprehensive Guide
Key Takeaway
The Anterior Retroperitoneal Approach provides direct visualization for lumbar spine surgery, addressing pathologies like degenerative disc disease and spondylolisthesis. It offers biomechanical advantages such as large graft footprints, restoring disc height and sagittal balance. This approach necessitates a profound understanding of musculoskeletal, vascular, and neural anatomy to ensure safe and effective execution.
Introduction and Epidemiology
The anterior retroperitoneal approach to the lumbar spine represents a well-established surgical pathway for addressing various pathologies affecting the anterior column. This approach prioritizes direct visualization of the intervertebral disc space, enabling comprehensive discectomy, thorough endplate preparation, restoration of sagittal balance, and the placement of robust interbody support devices. Historically, anterior lumbar interbody fusion (ALIF) emerged as a direct alternative or adjunct to posterior fusion techniques, offering unique biomechanical advantages. Its evolution has been driven by advancements in surgical technique, instrumentation, and imaging, moving from open, often morbid, exposures to less invasive modifications.
Lumbar degenerative disc disease (DDD) is a significant cause of axial low back pain, with a global point prevalence estimated between 7.2% and 15%. When conservative management fails, surgical intervention is often considered. Conditions such as degenerative spondylolisthesis, instability, sagittal imbalance, and post-laminectomy syndrome frequently necessitate anterior column support. The anterior retroperitoneal approach is particularly advantageous for lumbosacral junction pathology (L5/S1) due to the challenging anatomical access posteriorly and the ability to achieve superior lordosis restoration anteriorly. While the incidence of ALIF procedures varies, its utilization remains consistent for specific indications, especially those requiring large interbody footprints and robust anterior support. The capacity to insert a cage with a large surface area minimizes the risk of subsidence, while the preservation of the posterior tension band optimizes the biomechanical environment for arthrodesis.
Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy of the anterior retroperitoneal space and the associated lumbar spine is paramount for safe and effective execution of this approach. The retroperitoneal space is a complex anatomic corridor demanding meticulous dissection to avoid catastrophic iatrogenic injury.
Musculoskeletal Anatomy
The lumbar spine typically consists of five vertebral bodies (L1-L5) and the sacrum. The intervertebral discs provide cushioning and allow movement. The anterior longitudinal ligament (ALL) runs along the anterior surfaces of the vertebral bodies and discs, providing significant anterior stability. Access to the lumbar spine via the anterior retroperitoneal approach involves navigating through the anterior abdominal wall musculature.
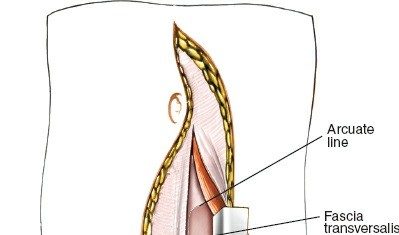
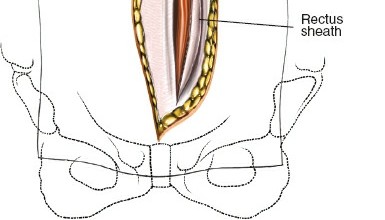
- Rectus Abdominis: A paired muscle running vertically, enclosed by the rectus sheath. The arcuate line, located midway between the umbilicus and the pubic symphysis, marks the transition where the posterior rectus sheath terminates, leaving only the transversalis fascia posteriorly.
- External Oblique, Internal Oblique, and Transversus Abdominis: Layers of muscle lateral to the rectus, whose fibers run in different directions, forming the lateral abdominal wall.
- Psoas Major: A critical landmark in the retroperitoneum. The lumbar plexus is embedded within its substance. The psoas must often be mobilized laterally to expose the lateral margins of the disc spaces, particularly at L4-L5 and above.
Vascular Anatomy
The major vascular structures dictate the surgical windows and represent the most critical anatomical considerations during an anterior approach.
- Aorta: Located on the left side of the vertebral column, bifurcating into the common iliac arteries typically at the lower third of the L4 vertebral body.
- Inferior Vena Cava (IVC): Located on the right side of the vertebral column, formed by the confluence of the common iliac veins, typically at the L5 level. The IVC is thin-walled and highly susceptible to retraction injury.
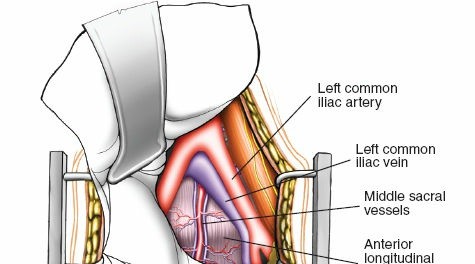
- Common Iliac Arteries and Veins: Originate from the aorta and IVC, respectively. The left common iliac vein is particularly vulnerable as it crosses the midline anterior to the L5 vertebral body to join the right common iliac vein.
- Iliolumbar Vein: A critical tethering vessel that typically drains into the common iliac vein or distal IVC. It courses laterally and must be identified and ligated during an L4-L5 exposure to permit medial mobilization of the left common iliac vein without avulsion.
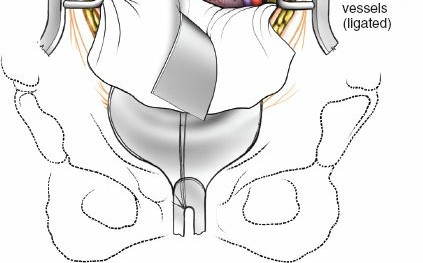
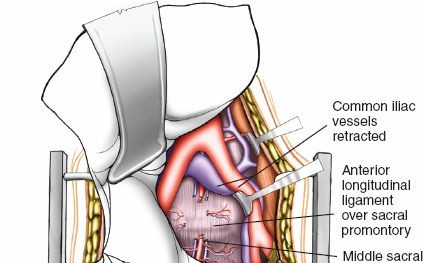
- Middle Sacral Artery and Vein: Typically located directly anterior to the L5/S1 disc space, originating from the distal aorta and draining into the IVC or left common iliac vein. These vessels must be identified, coagulated, and divided to access the L5/S1 disc.
Neural Anatomy
Several critical neural structures traverse the retroperitoneal space and are at risk during dissection and retraction.
- Lumbar Sympathetic Chain: Paired ganglia running anterolateral to the vertebral bodies, medial to the psoas muscle. Injury can lead to sympathetic dysfunction, including altered temperature regulation in the lower extremity.
- Superior Hypogastric Plexus: A network of sympathetic nerves situated anterior to the aortic bifurcation and the L5 vertebral body. Meticulous, blunt dissection and avoidance of monopolar electrocautery in this region are mandatory to prevent injury, which manifests as retrograde ejaculation in male patients (incidence reported up to 10%).
- Genitofemoral Nerve: Pierces the anterior surface of the psoas major muscle. Retraction or direct trauma can result in paresthesias or pain in the groin and anterior thigh.
Biomechanical Principles
The anterior approach offers distinct biomechanical advantages. By placing a large interbody graft within the anterior and middle columns, the surgeon maximizes the surface area for fusion, thereby distributing axial loads over the strong cortical rim of the vertebral endplates. This significantly reduces the risk of cage subsidence compared to the smaller footprints utilized in posterior approaches (PLIF/TLIF). Furthermore, anterior placement allows for the utilization of hyperlordotic cages, leveraging the intact posterior elements as a tension band. This compression across the anterior graft enhances stability and promotes osteogenesis according to Wolff's Law, while simultaneously restoring regional lumbar lordosis and global sagittal balance.
Indications and Contraindications
Patient selection is paramount for the success of the anterior retroperitoneal approach. The primary objective is to address anterior column pathology, restore disc height, decompress the neural foramina indirectly, and achieve solid arthrodesis.
| Category | Specific Conditions |
|---|---|
| Operative Indications | Degenerative Disc Disease (DDD) at L4-L5 or L5-S1 |
| Isthmic or Degenerative Spondylolisthesis (Grade I or II) | |
| Pseudarthrosis following previous posterior fusion | |
| Iatrogenic flatback syndrome / Sagittal plane deformity | |
| Discitis/Osteomyelitis requiring anterior debridement | |
| Absolute Contraindications | Active systemic infection |
| Severe aortoiliac occlusive disease or severe vascular calcification | |
| Prior extensive retroperitoneal surgery or radiation (relative to absolute) | |
| Relative Contraindications | Severe obesity (BMI > 40) |
| High-grade spondylolisthesis (Grade III or higher) | |
| Severe central canal stenosis requiring direct posterior decompression |
The decision to proceed with an anterior approach versus a posterior or lateral approach hinges on the specific level involved. L5-S1 is uniquely suited for ALIF because the iliac crests obstruct lateral access, and the paraspinal musculature makes posterior access to the disc space challenging. Furthermore, the vascular bifurcation typically allows a direct anterior window to L5-S1. Conversely, L4-L5 requires mobilization of the great vessels, carrying a higher risk of vascular injury.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning mitigates intraoperative complications and ensures appropriate implant selection.
Imaging Considerations
Standard orthogonal radiographs (AP and lateral) are required to assess global sagittal alignment, pelvic parameters (Pelvic Incidence, Pelvic Tilt, Sacral Slope), and the degree of spondylolisthesis. Flexion-extension views evaluate dynamic instability.
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating disc hydration, neural element compression, and the presence of a Modic changes. Crucially, axial MRI slices must be scrutinized to map the vascular anatomy. The level of the aortic bifurcation and the confluence of the IVC dictate the surgical window.
Computed Tomography (CT) without contrast is invaluable for assessing bony anatomy, endplate morphology, and the presence of osteophytes that may complicate exposure. In patients with a history of vascular disease, prior abdominal surgery, or advanced age, a CT Angiogram (CTA) or MR Angiogram (MRA) is highly recommended to evaluate vessel patency, calcification, and anatomical variants (e.g., a low-lying bifurcation or a left-sided IVC).
Patient Positioning
Proper patient positioning is a critical preliminary step that facilitates exposure and assists in the restoration of lordosis.
The patient is positioned supine on a radiolucent operating table. A lumbar bump or an inflatable bladder is placed beneath the target lumbar levels to accentuate lumbar lordosis and open the anterior disc space. The arms are extended and secured on arm boards, ensuring they do not obstruct lateral fluoroscopy. The patient's legs are typically spread slightly to allow the surgeon to stand between them if necessary, though many surgeons operate from the patient's left side.
Fluoroscopy is utilized prior to prepping and draping to confirm the precise location of the target disc spaces. The C-arm must be able to freely obtain true AP and lateral images without obstruction from the table base. The abdomen is prepped widely, from the nipples to the pubic symphysis, and laterally to the mid-axillary lines.
Detailed Surgical Approach and Technique
The anterior retroperitoneal approach is frequently performed in conjunction with an access surgeon (General or Vascular Surgeon), although many fellowship-trained spine surgeons perform the exposure independently.
Incision and Superficial Dissection
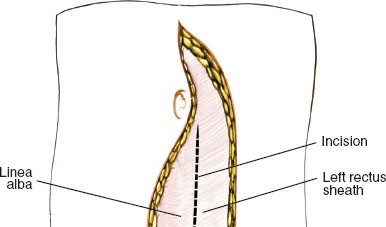
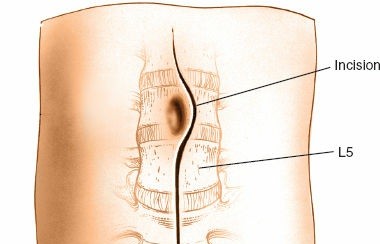
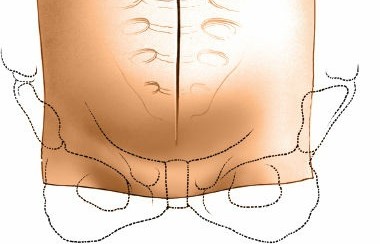
The choice of incision depends on the target levels and patient body habitus. For an isolated L5-S1 ALIF, a transverse Pfannenstiel incision or a low transverse muscle-splitting incision is cosmetically superior and provides excellent access. For multi-level exposures (e.g., L4-S1) or in obese patients, a vertical paramedian or midline incision is preferred for extensibility.
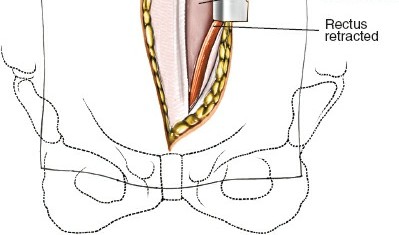
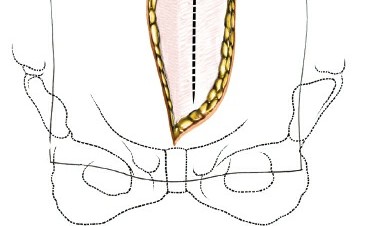
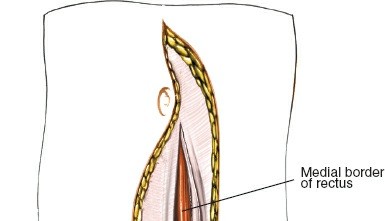
Following the skin incision, the subcutaneous tissue is divided to expose the anterior rectus sheath. If a transverse incision is used, the anterior sheath is incised transversely, and the rectus abdominis muscle is mobilized and retracted laterally. In a vertical paramedian approach, the anterior sheath is incised vertically, the rectus muscle is retracted laterally, and the posterior rectus sheath (if above the arcuate line) or transversalis fascia is exposed.
Retroperitoneal Access
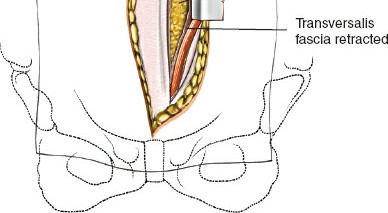
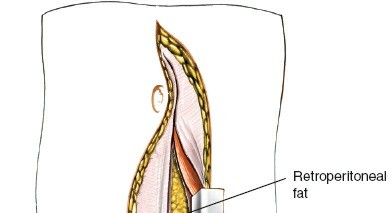
The transversalis fascia is carefully incised to enter the retroperitoneal space. This is a critical juncture; the underlying peritoneum is thin and easily breached.
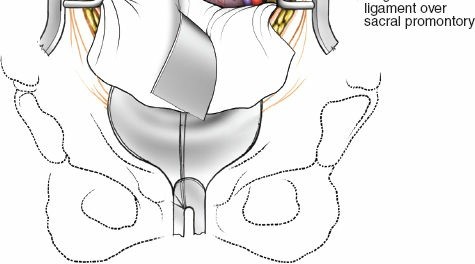
Using blunt dissection with Kittner sponges or the surgeon's fingers, the peritoneal sac is swept medially from the undersurface of the transversalis fascia and the lateral abdominal wall. The dissection proceeds posteriorly along the psoas muscle. The ureter, which adheres to the undersurface of the peritoneum, is swept medially along with the peritoneal contents. Identification of the psoas major muscle confirms entry into the correct anatomical plane.
Self-retaining retractors (e.g., Omni-Tract or SynFrame) are deployed. The blades must be positioned carefully to maintain the medial sweep of the peritoneum without exerting excessive pressure on the viscera or the ureter.
Level Specific Vascular Mobilization
The approach to the disc space is dictated by the vascular anatomy and the target level.
L5-S1 Exposure:
The L5-S1 disc space is typically accessed via the inter-iliac window, located below the aortic bifurcation. The middle sacral artery and vein are identified coursing vertically over the L5-S1 disc. These vessels are isolated, ligated with clips or ties, and divided. The superior hypogastric plexus, a delicate meshwork of nerves anterior to the L5 vertebral body, must be mobilized bluntly using a "peanut" sponge or Kittner. Monopolar electrocautery is strictly contraindicated here to prevent retrograde ejaculation. Gentle lateral retraction of the common iliac vessels exposes the entire width of the L5-S1 disc.

L4-L5 Exposure:
Accessing L4-L5 requires mobilization of the great vessels, typically from left to right. The left common iliac artery and vein, and often the distal aorta and IVC, must be mobilized medially. The critical tethering structure is the iliolumbar vein, which arises from the left common iliac vein or distal IVC and courses deeply into the psoas muscle. The iliolumbar vein must be meticulously isolated, ligated, and divided. Failure to do so can result in catastrophic avulsion from the common iliac vein during retraction. Once divided, the great vessels can be safely retracted medially past the midline to expose the L4-L5 disc space.
Discectomy and Endplate Preparation
Once the disc space is adequately exposed and retractors are secured, a wide anterior annulotomy is performed using a long-handled scalpel (e.g., #15 blade).
A comprehensive discectomy is executed using a combination of pituitary rongeurs, curettes, and Cobb elevators. The cartilaginous endplates must be meticulously removed to expose bleeding subchondral bone, which is essential for osteoinduction and fusion.
However, aggressive decortication that breaches the subchondral bone must be strictly avoided. The structural integrity of the subchondral bone is the primary deterrent to cage subsidence. The posterior annulus is typically preserved to act as a tension band, though it may be released if severe deformity correction is required. Indirect decompression of the neural foramina is achieved through the restoration of disc height.
Implant Insertion and Fixation
Trial spacers are utilized to determine the optimal cage size, height, and lordotic angle. The goal is to achieve a tight press-fit that restores sagittal balance and maximizes annular tension. Fluoroscopy confirms trial positioning.
The definitive interbody cage, packed with bone graft (autograft, allograft, or biologics such as rhBMP-2), is impacted into the disc space. Modern ALIF systems frequently utilize integrated fixation, where screws or blades are deployed through the cage directly into the adjacent vertebral bodies. Alternatively, an anterior neutralization plate can be applied. If integrated fixation is not used, or if biomechanical instability dictates, supplemental posterior pedicle screw instrumentation is performed in a staged or concurrent fashion.
Closure
Prior to closure, the retractor blades are temporarily relaxed to inspect for occult venous bleeding, particularly from the IVC or common iliac veins. A Valsalva maneuver is requested from the anesthesia team to increase venous pressure and unmask any small tears. Hemostasis is achieved with bipolar electrocautery or hemostatic agents. The retroperitoneal space does not typically require a drain unless there is significant oozing. The anterior rectus sheath is closed with heavy, non-absorbable or slowly absorbable continuous sutures. The subcutaneous tissues and skin are closed in a standard layered fashion.
Complications and Management
The anterior retroperitoneal approach is associated with a unique complication profile distinct from posterior spine surgery. Mastery of complication management is mandatory for surgeons utilizing this approach.
| Complication | Incidence | Etiology / Risk Factors | Prevention and Salvage Strategies |
|---|---|---|---|
| Vascular Injury | 1% - 5% | Laceration or avulsion of the left common iliac vein, IVC, or iliolumbar vein. | Prevention: Pre-op CTA, meticulous isolation of the iliolumbar vein, careful retraction. Salvage: Immediate direct pressure, mobilization of proximal/distal control, primary repair with 5-0 or 6-0 Prolene. Vascular surgery consultation. |
| Retrograde Ejaculation | 1% - 10% | Injury to the superior hypogastric plexus at L5-S1. | Prevention: Blunt dissection only over the L5-S1 disc space. Avoid monopolar electrocautery. Salvage: Often transient, but can be permanent. Urological consultation for fertility management. |
| Ureteral Injury | < 1% | Direct laceration or thermal injury during peritoneal sweeping. | Prevention: Identify ureter on the undersurface of the peritoneum. Avoid cautery near the peritoneal reflection. Salvage: Intraoperative urology consult, primary repair over a stent. |
| Deep Vein Thrombosis (DVT) | 2% - 5% | Venous stasis from retraction of the common iliac vein. | Prevention: Minimize retraction time. Release retractors periodically. Post-operative chemical prophylaxis and early mobilization. |
| Sympathetic Chain Injury | 1% - 3% | Disruption of the lumbar sympathetic chain. | Prevention: Careful dissection lateral to the vertebral bodies. Salvage: Results in ipsilateral lower extremity warmth and anhidrosis. Usually self-limiting and well-tolerated. |
| Peritoneal Breach / Ileus | 5% - 10% | Tearing the peritoneum during exposure. | Prevention: Gentle blunt dissection. Salvage: Primary repair of the peritoneum with absorbable suture. Post-operative bowel rest and slow diet advancement to manage ileus. |
| Cage Subsidence | 5% - 15% | Over-decortication of endplates, poor bone quality (osteopenia). | Prevention: Preserve subchondral bone. Use large footprint cages. Optimize bone health pre-operatively. Salvage: May require posterior supplemental fixation if symptomatic or progressing to pseudarthrosis. |
Post Operative Rehabilitation Protocols
Post-operative management focuses on early mobilization, pain control, and monitoring for approach-related complications.

Clinical & Radiographic Imaging
You Might Also Like
