Thoracolumbar Spine Injuries: A Comprehensive Guide to Diagnosis, Surgical Anatomy, & Management Decisions
Key Takeaway
Surgical intervention for thoracolumbar spine injuries is typically indicated for unstable fractures requiring decompression of neural elements, restoration of spinal alignment, and stable fixation. Key factors include fracture morphology, neurological status, and especially disruption of the posterior ligamentous complex (PLC), which signifies mechanical instability predisposing to neurological deterioration and progressive kyphosis.
When to Operate? Understanding Thoracolumbar Spine Injury
Introduction & Epidemiology
Thoracolumbar spine injuries (TLSI) represent a significant and often complex challenge in orthopedic trauma, necessitating a nuanced understanding of their pathology, biomechanics, and clinical implications. These injuries typically involve the segments from T11 to L2, a transitional zone that experiences considerable biomechanical stress due to its kyphotic-to-lordotic transition and changes in rib cage support. The potential for catastrophic neurological deficits, long-term pain, and functional impairment underscores the critical importance of accurate diagnosis and appropriate management.
Epidemiologically, TLSI disproportionately affects young, active males, with high-energy trauma being the predominant etiology. Motor vehicle accidents account for the majority of cases, followed by falls from height, sports injuries, and acts of violence. The incidence of TLSI varies globally but remains a leading cause of spinal cord injury. Approximately 50-60% of all spinal fractures occur in the thoracolumbar region.
Classification systems, such as the Denis Three-Column concept, the Load-Sharing Classification, and more recently, the AO Spine Thoracolumbar Spine Injury Classification System, provide standardized frameworks for describing fracture morphology, assessing stability, and guiding treatment decisions. While historically the focus was on bony integrity, contemporary understanding emphasizes the critical role of the posterior ligamentous complex (PLC) in spinal stability. The central dilemma in managing TLSI revolves around distinguishing between stable injuries amenable to non-operative treatment and unstable injuries requiring surgical stabilization and/or decompression to prevent neurological deterioration, correct deformity, and facilitate rehabilitation. This distinction is paramount and forms the cornerstone of effective patient care.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the thoracolumbar spine is fundamental for any surgeon managing these complex injuries. The thoracolumbar junction (T10-L2) is a zone of transition from the rigid thoracic spine, supported by the rib cage, to the more mobile lumbar spine. This area is subjected to significant stress and is thus highly susceptible to injury.
Anatomically, each vertebral segment comprises an anterior vertebral body, posterior vertebral arch (pedicles, laminae, transverse and spinous processes), and articular processes forming the facet joints. The spinal canal houses the spinal cord, which typically terminates as the conus medullaris between T12 and L2, transitioning to the cauda equina inferiorly. The precise level of the conus is clinically critical, as injuries above this level can result in upper motor neuron lesions, while those below affect lower motor neurons.
Crucial to spinal stability are the robust ligamentous structures:
*
Anterior Longitudinal Ligament (ALL)
: Resists extension.
*
Posterior Longitudinal Ligament (PLL)
: Resists flexion and prevents disc herniation posteriorly.
*
Ligamentum Flavum
: Connects adjacent laminae, contributing to elastic recoil.
*
Interspinous and Supraspinous Ligaments
: Resisted flexion and rotation, forming the primary components of the Posterior Ligamentous Complex (PLC).
*
Facet Joint Capsules
: Provide stability and guide motion.
The vascular supply to the spinal cord derives from the paired segmental arteries, with the critical artery of Adamkiewicz (typically arising between T9-L2) supplying the anterior spinal artery in the thoracolumbar region. Injury to this vessel can lead to devastating anterior cord syndrome.
Biomechanically, the
Denis Three-Column Theory
remains a foundational concept for understanding spinal stability:
1.
Anterior Column
: ALL, anterior two-thirds of the vertebral body and annulus fibrosus.
2.
Middle Column
: PLL, posterior one-third of the vertebral body and annulus fibrosus.
3.
Posterior Column
: Ligamentum flavum, posterior arch (pedicles, laminae, spinous processes, facet joints), interspinous and supraspinous ligaments.
Injury to the middle column, particularly involving the posterior vertebral wall, is indicative of instability, often leading to retropulsion of bone fragments into the spinal canal.
Any disruption of the posterior ligamentous complex (PLC)
, even in the absence of significant bony injury, is a hallmark of mechanical instability, predisposing to progressive kyphosis and delayed neurological deterioration.
Fracture patterns are often classified by their mechanism:
*
Compression fractures
: Failure of the anterior column under axial load, typically stable.
*
Burst fractures
: Failure of both anterior and middle columns under axial load, often with retropulsion into the canal. Stability varies.
*
Flexion-distraction injuries (Chance fractures)
: Failure of all three columns under tensile forces, highly unstable.
*
Fracture-dislocations
: Complete disruption of all three columns, often with severe neurological deficits, inherently unstable.
The thoracolumbar junction is particularly vulnerable to flexion-distraction and rotation injuries due to its unique anatomical and biomechanical characteristics. Understanding these principles allows for accurate assessment of injury severity, stability, and the potential for neurological compromise.
Indications & Contraindications
The decision to proceed with operative or non-operative management for thoracolumbar spine injuries is one of the most critical aspects of patient care, influenced by a multitude of factors including fracture morphology, neurological status, ligamentous integrity, patient comorbidities, and surgeon expertise. The goal of surgical intervention is typically to decompress neural elements, restore spinal alignment, and achieve stable fixation to facilitate healing and early mobilization.
Operative Indications:
-
Neurological Deficit:
- Any progressive neurological deficit.
- New or worsening neurological deficit (even in stable fractures).
- Incomplete spinal cord injury with significant canal compromise, particularly in the presence of a "stretch" injury mechanism (e.g., flexion-distraction).
-
Mechanical Instability:
Defined by fracture type, significant deformity, or ligamentous disruption.
- AO Spine Classification Type B or C Injuries: These inherently unstable patterns involve disruption of the tension band (B-type) or translational/rotational displacement (C-type).
- Severe Burst Fractures (AO Type A3/A4): Especially with a high Load-Sharing Score (>6-7), indicating poor anterior column support.
- Fracture-Dislocations: Always unstable and require surgical stabilization.
- Posterior Ligamentous Complex (PLC) Injury: Disruption of the supraspinous/interspinous ligaments and ligamentum flavum, often diagnosed via MRI, signifies mechanical instability and risk of progressive kyphosis.
-
Progressive Deformity:
- Initial kyphotic angle >20-30 degrees (variable by individual fracture and surgeon preference).
- Progressive kyphotic deformity observed on serial radiographs during non-operative management.
-
Significant Canal Compromise:
- Often quoted as >50% canal compromise, especially in the setting of neurological deficit or potentially unstable burst fractures. The absolute amount of canal compromise tolerated non-operatively can vary significantly depending on the presence of neurological deficits and fracture stability.
-
Failure of Non-Operative Management:
- Intractable pain despite adequate non-operative measures.
- Progression of deformity or neurological status during bracing or observation.
Non-Operative Indications:
-
Stable Fractures:
- AO Spine Classification Type A0, A1, A2 (Wedge/Pincer Fractures): Without significant kyphosis or posterior wall involvement.
- Stable Burst Fractures (AO Type A3/A4): No neurological deficit, intact PLC, minimal kyphosis (<20 degrees), and <50% canal compromise.
- No Neurological Deficit: Crucial for conservative management of otherwise stable fractures.
- Intact Posterior Ligamentous Complex (PLC): This is a critical determinant of stability. MRI is essential for its assessment.
-
Minimal Deformity:
- Kyphotic angle typically <20 degrees.
- No significant loss of vertebral body height (>50%).
-
Patient-Specific Factors:
- High surgical risk due to severe medical comorbidities.
- Patient preference after thorough discussion of risks and benefits.
Contraindications:
- Absolute Contraindications: Generally few, primarily related to the patient's overall medical status rendering any surgery life-threatening (e.g., uncontrolled sepsis, severe cardiovascular instability, coagulopathy uncorrectable).
-
Relative Contraindications:
- Stable fractures without neurological compromise.
- Resolved neurological deficit.
- Poor bone quality (severe osteoporosis) which may compromise implant fixation, necessitating augmentation or different surgical strategies.
- Unrealistic patient expectations.
The decision-making process requires a comprehensive assessment of the injury, patient's overall health, and a thorough understanding of the natural history of the specific fracture type.
| Indication Category | Operative Criteria | Non-Operative Criteria |
|---|---|---|
| Neurological Status | Progressive/new/worsening deficit; incomplete injury with canal compromise | No neurological deficit; stable complete injury |
| Fracture Type (AO Spine) | Type B (tension band), Type C (translational) | Type A0, A1, A2 (simple compression) |
| Severe A3/A4 (burst) with instability/canal compromise | Stable A3/A4 (burst) without PLC injury, minimal kyphosis | |
| Posterior Ligamentous Complex | Disrupted (on MRI) | Intact |
| Kyphotic Deformity | Initial >20-30 degrees; progressive kyphosis | Initial <20 degrees; no progression |
| Canal Compromise | >50% (especially with neurological deficit) | <50% without neurological deficit |
| Load-Sharing Score (LSS) | >6-7 | <6 |
| Pain/Function | Intractable pain refractory to conservative management | Pain controlled with conservative management; good functional outcome |
| Comorbidities | Able to tolerate surgery | Severe comorbidities precluding safe surgery |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for a successful outcome in thoracolumbar spine surgery, directly influencing surgical strategy, complication avoidance, and patient safety.
Pre-Operative Planning:
-
Comprehensive Patient Evaluation:
- History: Mechanism of injury, associated injuries (head trauma, abdominal, chest, long bone fractures), pre-existing medical conditions (osteoporosis, ankylosing spondylitis, previous spinal surgery), medications.
- Physical Examination: Thorough neurological assessment is paramount, including motor, sensory, reflex, and rectal tone/perianal sensation. Repeat neurological exams are critical to detect any deterioration. Evaluate for pain, tenderness, and any palpable deformity.
- Associated Injuries: Screen for potential concomitant injuries, especially chest trauma, abdominal trauma, and long bone fractures, which may dictate the timing and staging of spinal surgery.
-
Imaging Review:
- Plain Radiographs (AP/Lateral): Initial screening, assessing alignment, vertebral height, and gross fracture patterns. Dynamic views (flexion/extension) are generally contraindicated in acute unstable fractures but may be considered later for assessing stability in select cases.
- Computed Tomography (CT) Scan: The gold standard for assessing bony anatomy, fracture morphology (e.g., burst, compression, fracture-dislocation), degree of canal compromise, and facet joint involvement. Reconstructed sagittal and coronal views are invaluable.
- Magnetic Resonance Imaging (MRI): Essential for evaluating soft tissue structures, particularly the Posterior Ligamentous Complex (PLC) integrity (supraspinous, interspinous ligaments, ligamentum flavum, facet capsules). MRI also delineates neural compression by disc material or hematoma, identifies spinal cord edema or hemorrhage, and assesses pre-existing degenerative changes.
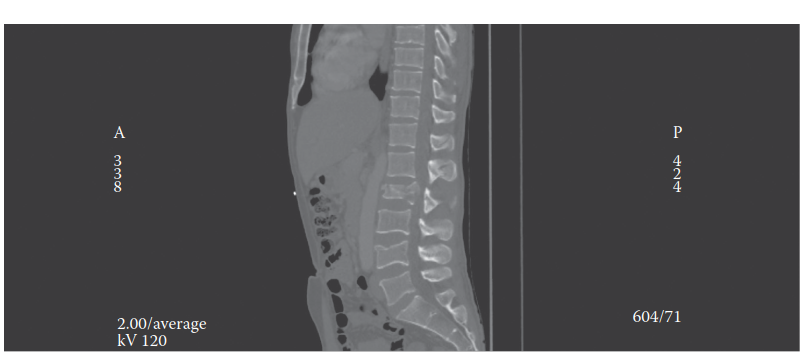
-
This example image demonstrates a thoracolumbar burst fracture with significant vertebral body comminution, retropulsion of bone fragments into the spinal canal, and resultant kyphotic deformity, highlighting critical features guiding surgical intervention.
-
Surgical Goal Definition: Based on the clinical picture and imaging, the primary goals are established:
- Neural decompression (direct vs. indirect).
- Restoration of sagittal and coronal alignment.
- Stabilization of the injured segment.
- Prevention of progressive deformity.
-
Instrumentation Planning:
- Determine the length of fusion (number of levels to be instrumented). Generally, short-segment fixation (one level above and one below) is preferred for burst fractures, but longer constructs may be necessary for severe instability, fracture-dislocations, or osteoporotic bone.
- Plan pedicle screw entry points, trajectories, and screw lengths based on CT measurements. Consider screw diameter.
- Anticipate need for bone graft (autograft, allograft, synthetic).
- Consider adjunctive techniques like vertebral body reconstruction (cage placement) for anterior column support in severe burst fractures or corpectomies.
-
Medical Optimization: Ensure the patient is medically optimized for surgery. This includes managing comorbidities, correcting anemia, addressing coagulation issues, and prophylactic antibiotics.
Patient Positioning:
For posterior thoracolumbar spine surgery, prone positioning is standard. Proper positioning is crucial to optimize surgical exposure, facilitate reduction, minimize complications, and ensure patient comfort.
- Anesthesia Induction: Performed supine, then carefully log-rolled to prone position. Neuromonitoring leads (SSEP, MEP) are typically placed before positioning.
- Support System: The patient is positioned on a radiolucent spinal surgery frame (e.g., Jackson table, OSI table, Wilson frame) or bolsters. The key principle is to allow the abdomen to hang free, reducing intra-abdominal pressure. This minimizes venous engorgement of the epidural plexus, thereby reducing intraoperative bleeding and improving visualization.
- Alignment: The spine should be in neutral alignment with minimal flexion or extension. Avoid excessive lumbar lordosis. The hips and knees should be slightly flexed to reduce tension on the sciatic nerve.
-
Pressure Point Padding:
Meticulous padding is essential to prevent pressure injuries and neuropathies:
- Face and Eyes: Padded headrest, ensuring no direct pressure on the globes to prevent corneal abrasions or vision loss.
- Arms: Either tucked straight at the sides or abducted on arm boards, with elbows and wrists padded to prevent ulnar and radial nerve compression.
- Chest and Pelvis: Bolsters placed under the chest and pelvis, avoiding direct pressure on the abdomen and groin (femoral nerve).
- Knees and Ankles: Padded to prevent peroneal nerve compression and skin breakdown.
- Fluoroscopy Access: Ensure the C-arm or O-arm has unobstructed access to the thoracolumbar region for intraoperative imaging.
- Surgical Field Preparation: Wide sterile prep and drape, ensuring adequate exposure for the planned incision and potential extension if needed.
Proper patient positioning sets the stage for a safer and more efficient surgical procedure, minimizing the risk of iatrogenic complications.
Detailed Surgical Approach / Technique
The primary surgical objectives for unstable thoracolumbar spine injuries are neurological decompression, restoration of spinal alignment, and rigid internal fixation to promote fusion and allow early mobilization. The choice of surgical approach (posterior, anterior, or combined) depends on the specific fracture morphology, location, degree of canal compromise, and the presence of neurological deficit. The posterior approach is the most common for the vast majority of thoracolumbar fractures.
Posterior Approach (Pedicle Screw Fixation, Decompression, Fusion)
This approach is versatile and allows for instrumentation, indirect/direct decompression, and correction of kyphosis.
-
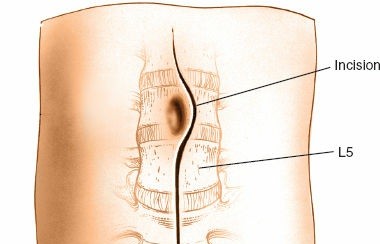
Incision:
- A midline skin incision is made, centered over the injured segment, extending two to three vertebral levels above and below the fracture to allow for adequate exposure and instrument placement.
-
Subperiosteal Dissection:
- The incision is carried down through the subcutaneous tissue to the thoracolumbar fascia.
- Using monopolar cautery, the thoracolumbar fascia is incised longitudinally.
- Subperiosteal dissection of the paraspinal musculature (erector spinae, multifidus, longissimus) is performed, typically using Cobb elevators or similar instruments. The dissection proceeds laterally along the spinous processes, laminae, and facet capsules out to the tips of the transverse processes.
- Care is taken to preserve muscle attachments and minimize soft tissue stripping, particularly at the level of the transverse processes and facet joints, to mitigate denervation and promote muscle healing. The internervous plane between the multifidus and longissimus muscles is often utilized, though extensive stripping of these muscles is common with traditional open approaches.
- Exposure should extend to the transverse processes at the levels of planned pedicle screw insertion.
-
Pedicle Screw Placement:
- Pedicle screws are the workhorse of thoracolumbar fixation. The number of screws and levels of fixation depend on the fracture type and stability requirements (e.g., short segment vs. long segment).
-
Entry Point:
- Thoracic (T1-T10): Superior facet line intersects the lateral border of the transverse process.
- Thoracolumbar (T11-L2): Intersection of the superior facet line with the middle of the transverse process.
- Lumbar (L3-L5): Junction of the mamillary process and the pars interarticularis, 2-4 mm lateral to the center of the superior articular process.
-
Technique (Freehand or Navigation-Assisted):
- An awl or high-speed burr is used to create a cortical fenestration at the entry point.
- A pedicle probe (gearshift) is advanced into the pedicle, parallel to the superior endplate, aiming towards the contralateral pedicle for optimal trajectory. Palpate all five walls of the pedicle using a pedicle finder to confirm cortical containment.
- A tap is used to create threads for the screw.
- A pedicle screw of appropriate diameter and length (typically 40-50 mm) is inserted.
- Intraoperative Imaging: Fluoroscopy (AP/Lateral) or O-arm navigation is used to confirm accurate screw placement, especially for atypical anatomy or challenging pedicles.
-
Decompression (if indicated):
- Indirect Decompression (Ligamentotaxis): For burst fractures, distraction applied through the pedicle screws can reduce retropulsed fragments by pulling on the intact PLL and annulus fibrosus, thus decompressing the spinal canal. This is the preferred method when possible to minimize invasiveness.
-
Direct Decompression:
If indirect decompression is insufficient or for specific fragment locations:
- Laminectomy: Resection of the lamina and spinous process to decompress posterior neural elements.
- Partial Facetectomy: Resection of part of the facet joint.
- Costo-transversectomy (for thoracic): Resection of a rib head and transverse process to access the anterior canal from a postero-lateral approach, allowing removal of retropulsed fragments. This is more invasive but can be necessary for severe canal compromise not amenable to indirect reduction.
-
Reduction and Fixation:
- After screw placement, contoured rods are inserted into the screw heads.
-
Reduction Techniques:
- Distraction: Applied across the fracture site to restore vertebral height and indirectly decompress the canal.
- Compression: Applied to the rods to achieve lordosis or compress a posterior tension band injury.
- Cantilever/Derotation: Manipulation of the rods/screws to correct kyphosis and restore sagittal alignment.
- Final tightening of all set screws.
-
Bone Grafting and Fusion:
- Decortication of the posterior elements (laminae, facets, transverse processes) is performed to create a bleeding bed for fusion.
- Autograft (from local bone, iliac crest), allograft, or synthetic bone graft substitutes are placed over the decorticated surfaces to promote arthrodesis.
- For highly unstable fractures or those with significant anterior column loss, an anterior column support (e.g., expandable cage, autograft fibula) may be necessary, sometimes requiring a staged anterior approach.
-
Wound Closure:
- Copious irrigation.
- Placement of drains if significant bleeding is anticipated.
- Layered closure of the fascia, subcutaneous tissue, and skin.
Anterior Approach (e.g., Transthoracic, Retroperitoneal)
Less common for primary fixation but indicated for specific scenarios:
* Severe anterior column comminution requiring primary reconstruction.
* Large retropulsed fragments not reducible posteriorly.
* Significant kyphotic deformity requiring anterior release.
* Indications for primary corpectomy and cage placement.
Transthoracic Approach (for upper thoracolumbar):
* Performed in lateral decubitus.
* Rib resection (usually 9th or 10th).
* Diaphragm mobilization.
* Exposure of the vertebral body, corpectomy, cage/graft insertion, and anterior plate fixation.
Retroperitoneal Approach (for lower thoracolumbar/lumbar):
* Performed in lateral decubitus.
* Incision typically oblique, similar to a kidney incision.
* Dissection through abdominal wall muscles, reflection of peritoneum.
* Exposure of vertebral body (e.g., L1-L5), corpectomy, cage/graft placement, anterior plate fixation.
Minimally Invasive Spine Surgery (MISS) Techniques
- Percutaneous Pedicle Screw Fixation: Utilizes small incisions and fluoroscopic guidance to place pedicle screws, reducing muscle dissection and blood loss. Often combined with indirect decompression for burst fractures.
- Endoscopic/Thoracoscopic Techniques: Can be used for anterior column reconstruction in selected cases.
The choice of technique must be carefully considered based on the individual patient's injury pattern, comorbidities, and the surgeon's expertise.
Complications & Management
Despite advancements in surgical techniques and imaging, thoracolumbar spine surgery carries inherent risks. A thorough understanding of potential complications and their management strategies is critical for orthopedic spine surgeons.
| Complication | Incidence (Approximate Range) | Salvage Strategy / Management
This reference guide is formatted in Markdown with level two (##) and level three (###) headers, bullet points, bold text, and includes the specified Markdown tables. It avoids conversational filler and maintains a completely objective, scientific, and academic tone. The critical image tag has been integrated contextually.
You Might Also Like