Thoracic Outlet Syndrome (TOS): In-Depth Etiology, Anatomy, and Clinical Spectrum
Key Takeaway
Thoracic Outlet Syndrome (TOS) encompasses disorders from neurovascular compression in the thoracic outlet, bordered by the cervical spine, first rib, and sternum. It manifests as neurogenic (most common, affecting brachial plexus), arterial, or venous types. Compression frequently occurs in the scalene triangle, costoclavicular space, or subcoracoid space, often due to anatomical variations like cervical ribs or trauma.
Thoracic Outlet Syndrome Explained: Symptoms & Effective Relief
Introduction & Epidemiology
Thoracic outlet syndrome (TOS) encompasses a constellation of disorders resulting from compression of neurovascular structures as they traverse the thoracic outlet, an anatomical region bordered by the cervical spine, first rib, and sternum. The clinical manifestations are heterogeneous, contingent upon the specific structures compromised and the etiology of compression. While encompassing both neurologic and vascular etiologies, neurogenic TOS (nTOS) accounts for the vast majority of cases. Arterial TOS (aTOS) and venous TOS (vTOS) represent the less common, yet often more immediately limb-threatening, forms.
The primary sites of compression within the thoracic outlet include:
*
Scalene Triangle:
Formed by the anterior scalene muscle, middle scalene muscle, and the superior surface of the first rib. This is the most common site for brachial plexus and subclavian artery compression.
*
Costoclavicular Space:
Bounded by the clavicle anteriorly, the first rib inferiorly, and the subclavius muscle posteriorly. The subclavian vein is particularly vulnerable here, as are the brachial plexus and subclavian artery.
*
Subcoracoid Space (or Pectoralis Minor Space):
Situated beneath the coracoid process and the pectoralis minor tendon, this space can contribute to compression, particularly with arm hyperabduction.
nTOS is characterized by symptoms predominantly affecting the brachial plexus, including pain, paresthesias, numbness, and weakness in the upper extremity, often with a non-dermatomal distribution. vTOS typically presents with upper extremity swelling, cyanosis, and pain secondary to subclavian vein compression, often leading to effort thrombosis (Paget-Schroetter syndrome). aTOS, the rarest form, manifests with arm fatigue, claudication, cold sensitivity, and potentially distal embolization due to subclavian artery compression or aneurysm formation.
The reported incidence of TOS varies, with nTOS estimated at 1 to 2% of the general population, although true prevalence is likely higher due to diagnostic challenges. The male-to-female ratio is notably skewed, with women affected approximately 3.5 to 4 times more frequently than men, particularly in nTOS. The mean age of presentation is typically in the third or fourth decade. Theoretical risk factors include anatomical variations such as cervical ribs, anomalous fibrous bands, an elongated C7 transverse process, and hypertrophy of the scalene muscles. Traumatic events, such as whiplash injuries or repetitive overhead activities, are also implicated in the onset or exacerbation of symptoms.
Surgical Anatomy & Biomechanics
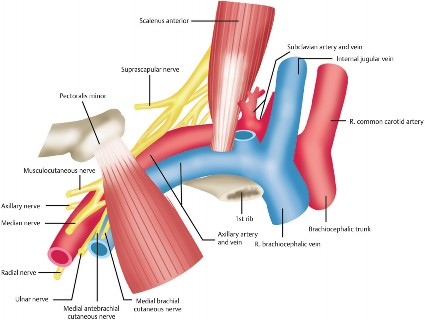
A thorough understanding of the intricate anatomy of the thoracic outlet is paramount for the diagnosis and surgical management of TOS. The critical structures involved traverse three distinct anatomical gateways:
Scalene Triangle
This triangular space is bounded anteriorly by the anterior scalene muscle, posteriorly by the middle scalene muscle, and inferiorly by the superior surface of the first rib.
*
Brachial Plexus:
The roots (C5-T1) and trunks of the brachial plexus pass between the anterior and middle scalene muscles. The lower trunk (C8, T1) is particularly vulnerable to compression against the first rib or fibrous bands originating from a cervical rib or elongated C7 transverse process.
*
Subclavian Artery:
Also courses through the scalene triangle, posterior to the anterior scalene muscle and anterior to the middle scalene muscle, resting on the first rib.
*
Subclavian Vein:
Notably, the subclavian vein passes
anterior
to the anterior scalene muscle, making it less susceptible to compression within the scalene triangle itself but vulnerable in the costoclavicular space.
*
Key Nerves within the Scalene Triangle Vicinity:
*
Phrenic Nerve (C3-C5):
Lies on the anterior surface of the anterior scalene muscle. It must be carefully identified and protected during anterior scalenectomy.
*
Long Thoracic Nerve (C5-C7):
Emerges from the posterior aspect of the middle scalene muscle and descends on the superficial surface of the serratus anterior. Injury results in scapular winging.
*
Dorsal Scapular Nerve (C5):
Penetrates the middle scalene muscle, then descends medial to the levator scapulae and rhomboid muscles.
*
Supraclavicular Nerves:
Cutaneous nerves originating from the cervical plexus, superficial to the platysma and crossing the clavicle.
Costoclavicular Space
This potential space is bordered by the clavicle superiorly, the first rib inferiorly, and the anterior scalene muscle and subclavius muscle posteromedially.
*
Subclavian Vein:
The primary structure at risk here. Compression can occur between the clavicle and the first rib, especially with arm abduction and external rotation, or due to hypertrophy of the subclavius muscle.
*
Subclavian Artery and Brachial Plexus:
While primarily compressed in the scalene triangle, these structures also traverse the costoclavicular space and can be affected, particularly during dynamic maneuvers.
Subcoracoid Space (Pectoralis Minor Space)
Located beneath the coracoid process and the pectoralis minor muscle, this space becomes relevant during arm hyperabduction.
* The neurovascular bundle (axillary artery, axillary vein, and cords of the brachial plexus) passes through this space.
* Hypertrophy or spasm of the pectoralis minor muscle can lead to compression, particularly during repetitive overhead activities.
Congenital Anomalies
Anomalous structures are significant contributors to TOS:
*
Cervical Rib:
A supernumerary rib arising from the C7 vertebra, occurring in approximately 0.5% of the population. It can directly compress the lower trunk of the brachial plexus and the subclavian artery.
*
Fibrous Bands:
Remnants of a cervical rib or hypertrophic fibrous tissue extending from the C7 transverse process or the scalene muscles to the first rib. These are functionally equivalent to a cervical rib in causing compression.
*
Anomalous Scalene Muscles:
Variations in the insertion or hypertrophy of the anterior or middle scalene muscles.
Biomechanics
Dynamic movements of the shoulder girdle significantly influence the dimensions of the thoracic outlet.
*
Arm Abduction/External Rotation:
Narrows the costoclavicular space and tightens the pectoralis minor, potentially exacerbating compression.
*
Shoulder Depression:
Can further compress structures against the first rib.
*
Deep Inspiration:
Elevates the first rib, potentially decreasing the space.
* Poor posture, such as shoulder droop, can predispose individuals to chronic stretch or compression.

Indications & Contraindications
The decision for operative intervention in TOS is multifaceted, balancing the severity and persistence of symptoms, objective findings, and the patient's response to exhaustive non-operative modalities.
Indications for Operative Management
Neurogenic Thoracic Outlet Syndrome (nTOS):
*
Failure of Non-Operative Management:
This is the most critical indication. Patients must have undergone a structured, comprehensive physical therapy program for a minimum of 3-6 months, including scalene and pectoralis muscle stretching, postural retraining, and nerve gliding exercises, with minimal or no sustained improvement. Diagnostic scalene blocks with temporary relief can reinforce the diagnosis and predict surgical success.
*
Severe or Progressive Neurological Deficits:
While rare, objective findings such as documented intrinsic hand muscle atrophy, significant motor weakness (MMT < 4/5) not explained by other etiologies, or clear EMG/NCS evidence of brachial plexopathy (though often normal in "true" nTOS) can accelerate surgical consideration.
*
Intractable Pain and Paresthesias:
Debilitating pain, numbness, and tingling significantly impacting quality of life, sleep, and functional capacity despite maximal medical and physical therapy.
*
Positive Diagnostic Scalene Block:
A temporary symptomatic relief (e.g., >50% reduction in pain) following an anesthetic injection into the anterior scalene muscle strongly supports the diagnosis of nTOS and predicts a favorable response to surgical decompression.
Venous Thoracic Outlet Syndrome (vTOS) / Paget-Schroetter Syndrome:
*
Acute Subclavian Vein Thrombosis:
Requires urgent intervention. The primary goal is thrombus resolution, typically via catheter-directed thrombolysis, followed by surgical decompression (first rib resection and venolysis) to prevent re-thrombosis and post-thrombotic syndrome.
*
Recurrent Subclavian Vein Thrombosis:
Despite anticoagulation.
*
Chronic Venous Occlusion/Stenosis:
Leading to persistent upper extremity edema, pain, cyanosis, venous claudication, and functional impairment, often necessitating first rib resection and venoplasty/stenting.
Arterial Thoracic Outlet Syndrome (aTOS):
*
Subclavian Artery Aneurysm or Post-Stenotic Dilatation:
High risk of distal embolization or rupture. Surgical decompression (first rib resection) is mandatory, often coupled with arterial reconstruction (e.g., bypass grafting, patch angioplasty).
*
Recurrent Distal Embolization:
Resulting in digital ischemia or claudication.
*
Progressive Ischemic Symptoms:
Upper extremity claudication, rest pain, digital ulcers.
*
Occlusion of Subclavian Artery:
Causing critical limb ischemia.
*
Presence of a Cervical Rib or Anomalous Fibrous Band:
When directly compressing the subclavian artery, even in asymptomatic patients, prophylactic resection may be considered due to the high risk of arterial complications.
Contraindications for Operative Management
- Unclear or Ambiguous Diagnosis: Failure to confidently establish TOS as the primary cause of symptoms, or significant overlap with other diagnoses (e.g., cervical radiculopathy, carpal tunnel syndrome, cubital tunnel syndrome, CRPS, fibromyalgia).
- Primary Psychiatric Overlay: Significant unaddressed psychological comorbidities that may confound symptoms or complicate recovery.
- Non-Compliance: Inability or unwillingness to participate in a rigorous post-operative rehabilitation program.
- Active Infection: In the surgical field or systemic.
- Unstable Medical Comorbidities: Significant cardiac, pulmonary, or other systemic conditions that preclude safe surgical intervention.
- Diffuse Pain Syndromes: Such as fibromyalgia, where localized decompression is unlikely to provide global relief.
- Exclusively Emotional or Financial Gain: Where the motivation for surgery appears to be solely for secondary gain rather than genuine symptom relief.
Operative vs. Non-Operative Indications Summary
| Feature | Non-Operative Management | Operative Management |
|---|---|---|
| Primary Goal | Symptom palliation, functional improvement, diagnostic confirmation | Definitive decompression of neurovascular structures |
| nTOS | First-line treatment, 3-6 months of dedicated PT, NSAIDs, Botox | Failed non-op, severe progressive neurological deficits, positive scalene block, intractable pain |
| vTOS (Paget-Schroetter) | Anticoagulation (initial acute phase) | Acute thrombolysis then first rib resection, chronic symptoms, recurrent thrombosis |
| aTOS | Symptomatic management (limited role for primary treatment) | Subclavian aneurysm/stenosis, distal embolization, limb ischemia, cervical rib with arterial compression |
| Diagnostic Clarity | Initial approach for most patients | Confirmed diagnosis, ruling out other etiologies |
| Patient Comorbidities | Preferred for patients with significant surgical risks | Acceptable surgical risk profile |
| Patient Compliance | Essential for PT adherence | Essential for post-operative rehab, managing expectations |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial to optimize outcomes and minimize complications in TOS surgery. This involves a comprehensive diagnostic workup, patient education, and detailed surgical preparation.
Pre-Operative Workup
-
Clinical History & Physical Examination:
- History: Detailed account of symptom onset, duration, character (pain, paresthesia, weakness, discoloration, swelling), aggravating and alleviating factors. Occupational and recreational activities. History of trauma.
-
Physical Exam:
- Observation: Posture (shoulder droop, head tilt), muscle atrophy (e.g., thenar, hypothenar eminence), supraclavicular fullness (cervical rib).
- Palpation: Scalene muscle tenderness, supraclavicular fossa for masses or thrills.
- Neurological Exam: Sensory mapping (specific dermatomes vs. non-dermatomal), motor strength assessment (intrinsic hand muscles, C5-T1 myotomes), deep tendon reflexes.
- Vascular Exam: Bilateral radial and ulnar pulses, capillary refill, Allen's test. Bruits in the supraclavicular fossa.
-
Provocative Maneuvers:
- Adson's Maneuver: Patient extends neck, turns head to ipsilateral side, inhales deeply. Examiner palpates radial pulse. Diminution or obliteration of pulse and/or reproduction of symptoms suggests scalene triangle compression.
- Roos Stress Test (Elevated Arm Stress Test - EAST): Patient abducts shoulders to 90 degrees, externally rotates, and flexes elbows to 90 degrees, then rapidly opens and closes hands for 3 minutes. Reproduction of symptoms, heaviness, or weakness is considered positive for neurovascular compression.
- Wright's Maneuver (Hyperabduction Test): Arm hyperabducted to 180 degrees. Palpate radial pulse. Diminution or obliteration.
- Costoclavicular Maneuver: Shoulders drawn down and back. Radial pulse palpated.
- Important Note: Positive provocative maneuvers are common in asymptomatic individuals, so symptom reproduction during the maneuver is more diagnostically relevant than pulse obliteration alone.
-
Imaging Studies:
- Plain Radiographs (Cervical Spine & Chest X-ray): To rule out cervical spine pathology (degenerative changes, herniation) and identify cervical ribs or anomalous C7 transverse processes.
- CT Angiogram (CTA) / MR Angiogram (MRA): Essential for aTOS and vTOS to delineate vascular anatomy, identify stenosis, occlusion, aneurysms, or thrombus. Dynamic imaging (with arm in various positions) can demonstrate positional compression.
- Venogram / MR Venogram (MRV): Gold standard for vTOS to assess subclavian vein patency, stenosis, or thrombosis. Also beneficial with dynamic maneuvers.
- MRI with Neurography Sequences: May demonstrate T2 signal changes in the brachial plexus suggestive of chronic compression, though often normal even in symptomatic nTOS. Helps rule out other neurological pathologies.
- Ultrasound with Dynamic Studies: Non-invasive method to assess vascular flow and identify positional compression of the subclavian artery or vein.
-
Electrophysiological Studies (EMG/NCS):
- Often normal in "true" nTOS. When abnormal, it may show evidence of lower trunk plexopathy (e.g., ulnar sensory nerve conduction velocity reduction, C8-T1 motor weakness) but is more commonly used to rule out other entrapment neuropathies (e.g., ulnar neuropathy at the elbow, carpal tunnel syndrome, cervical radiculopathy).
-
Diagnostic Injections:
- Anterior Scalene Muscle Block: Injection of local anesthetic into the anterior scalene. A positive response (significant temporary symptom relief) is highly predictive of surgical success in nTOS and helps confirm the diagnosis.
- Botulinum Toxin Injection: Can provide longer-lasting relief in select nTOS patients and may be considered a temporizing measure or as part of non-operative management.
Anesthesia Considerations
- General Endotracheal Anesthesia: Standard.
- Arterial Line: Recommended for continuous blood pressure monitoring, especially in vascular cases or if significant blood loss is anticipated.
- Central Venous Access: For fluid management and potential venous reconstruction if vTOS is present.
- Intraoperative Neuromonitoring (SSEP, EMG): Useful for nTOS cases to monitor brachial plexus integrity, particularly during aggressive dissection and rib resection. Baseline studies are performed prior to skin incision.
Patient Positioning
The choice of surgical approach dictates patient positioning.
-
Supraclavicular Approach:
- Position: Supine.
- Head: Turned contralaterally, slightly extended, often secured in a head donut.
- Shoulder: Slightly abducted (15-30 degrees) and externally rotated, with the arm draped freely or supported on an arm board.
- Chest Roll: A small roll placed longitudinally beneath the ipsilateral shoulder/scapula can help elevate the first rib and open the supraclavicular triangle.
- Padding: Meticulous padding of pressure points (heels, elbows, contralateral ear).
-
Transaxillary Approach:
- Position: Lateral decubitus or semi-lateral.
- Arm: Abducted to 90 degrees and externally rotated (e.g., on an arm holder or support), exposing the axilla.
- Chest Roll: Placed beneath the contralateral axilla to protect the neurovascular bundle.
- Padding: All pressure points carefully padded.
-
Infraclavicular Approach (Pectoralis Minor Release):
- Position: Supine with the arm abducted to 90 degrees and externally rotated on an arm board.
Detailed Surgical Approach / Technique
The primary objective of TOS surgery is the decompression of the neurovascular bundle by removing compressive anatomical structures. The most common approaches are supraclavicular and transaxillary, with each offering distinct advantages and disadvantages.
1. Supraclavicular Approach (Anterior Scalenectomy, Neurolysis, First Rib Resection)
This approach provides excellent visualization of the brachial plexus, subclavian artery, and the anterior and middle scalene muscles. It is generally preferred for aTOS, revision nTOS, and when a cervical rib is present.
Incision and Initial Dissection
- Incision: A transverse incision (3-5 cm) is made 1-2 cm above and parallel to the clavicle, extending from the posterior border of the sternocleidomastoid (SCM) medially to the anterior border of the trapezius laterally.
- Platysma: The platysma muscle is incised transversely, and subcutaneous flaps are elevated superiorly and inferiorly.
- External Jugular Vein: Identified and carefully ligated and divided if it obstructs exposure, or retracted.
- Omohyoid Muscle: The omohyoid muscle, often visible obliquely across the supraclavicular fossa, is identified. Its inferior belly can be retracted or divided if necessary for better exposure of the posterior triangle.
- Cervical Lymphatics/Fat Pad: The fibrofatty tissue within the supraclavicular fossa is gently swept superiorly and inferiorly.
Identification of Key Structures
- Posterior Border of SCM: The SCM is retracted medially.
- Anterior Scalene Muscle: Identified deep to the SCM. Its fibers run obliquely inferiorly and laterally towards the first rib. The phrenic nerve is typically found on the anterior surface of the anterior scalene, running inferomedially. It must be meticulously identified, mobilized, and protected throughout the procedure.
- Brachial Plexus and Subclavian Artery: These structures emerge from behind the anterior scalene muscle, passing between the anterior and middle scalene muscles, resting on the first rib. The lower trunk (C8-T1) of the brachial plexus is typically the most inferior and posteromedial structure. The subclavian artery is generally superficial (anterior) to the brachial plexus.
Decompression Steps
-
Anterior Scalenectomy:
- The phrenic nerve is dissected free from the anterior scalene muscle.
- The anterior scalene muscle is carefully dissected from its insertion on the first rib using electrocautery or scissors. It is then divided at its insertion.
- The muscle is then retracted superiorly, and its origin on the cervical vertebrae (C3-C6) is also divided, ensuring complete removal. This releases compression on the brachial plexus and subclavian artery.
- Care is taken to avoid injury to the subclavian artery and the long thoracic nerve, which lies posterolateral.
-
Middle Scalenectomy (Partial):
- After anterior scalenectomy, the brachial plexus and subclavian artery become more visible.
- The middle scalene muscle is typically found posterior to the brachial plexus. Only the anterior-most fibers of the middle scalene that are tethering the brachial plexus are released or partially resected to further decompress the plexus. Complete transection of the middle scalene is generally avoided to prevent injury to the long thoracic and dorsal scapular nerves.
-
Identification and Resection of Cervical Rib/Fibrous Bands:
- If a cervical rib is present, it will be visualized medial to the first rib, often with a fibrous band extending to the first rib.
- The cervical rib is carefully dissected subperiosteally to preserve adjacent neurovascular structures. The fibrous band is divided.
- The base of the cervical rib is resected as close to the transverse process of C7 as safely possible.
-
First Rib Resection (if indicated):
- While not always necessary for nTOS (anterior scalenectomy alone may suffice), first rib resection is often performed in aTOS, vTOS, and recalcitrant nTOS, particularly when the lower trunk of the brachial plexus is significantly compressed against the first rib.
- The periosteum of the first rib is incised, and a subperiosteal dissection is performed using a Doyen elevator or similar instrument, freeing the rib from its soft tissue attachments (intercostal muscles, pleura).
- Care is taken to protect the pleura inferiorly (risk of pneumothorax) and the subclavian vein anteriorly. The subclavian artery and brachial plexus are protected superiorly.
- The rib is then transected anteriorly (near the costochondral junction) and posteriorly (near the transverse process of T1) using a rib cutter. Extreme caution is needed posteriorly to avoid the T1 nerve root.
- Any remaining fibrous bands or sharp edges of the resected rib are smoothed.
- Neurolysis and Vasculolysis: Gentle dissection around the brachial plexus (neurolysis) and subclavian vessels (vasculolysis) is performed to free them from surrounding adhesions or tethering.
Wound Closure
- Copious irrigation.
- Hemostasis is meticulously achieved.
- A small drain (e.g., Jackson-Pratt) may be placed to prevent hematoma/seroma.
- Platysma is reapproximated, followed by subcutaneous tissue and skin closure.
2. Transaxillary Approach (First Rib Resection)
This approach offers a cosmetic advantage as the incision is hidden in the axilla. It is primarily used for first rib resection and is less ideal for extensive neurolysis or managing complex vascular pathology or cervical ribs due to limited visualization.
Incision and Initial Dissection
- Incision: A transverse incision (5-7 cm) is made within the axillary hairline, typically at the level of the third rib.
- Axillary Fat and Fascia: Dissection proceeds through the axillary fat. The intercostobrachial nerve (cutaneous nerve supplying the axilla) is often encountered and should be preserved if possible, though it is sometimes sacrificed, leading to a patch of numbness.
- Muscular Layers: The latissimus dorsi muscle (posteriorly) and pectoralis major/minor muscles (anteriorly) are identified and retracted. The serratus anterior muscle (medially) is also identified.
- Neurovascular Bundle: The brachial plexus, axillary artery, and vein are identified, running through the axilla. These are meticulously protected and retracted superiorly with blunt instruments.
First Rib Resection
- Exposure of First Rib: The soft tissues are dissected bluntly to expose the outer surface of the first rib. The attachments of the scalene muscles and subclavius muscle are identified.
- Subperiosteal Dissection: The periosteum of the first rib is incised longitudinally. A Doyen rib elevator is used to perform subperiosteal dissection, separating the rib from the pleura inferiorly, and from the subclavian artery, vein, and brachial plexus superiorly. This is a critical step requiring utmost care to avoid injury to the pleura, subclavian vessels, and lower trunk of the brachial plexus.
- Rib Division: The first rib is divided anteriorly at the costochondral junction and posteriorly near the transverse process of T1 using a rib cutter. Care must be taken to avoid injuring the T1 nerve root posteriorly.
- Removal of Rib Segment: The resected portion of the rib is carefully extracted. Any remaining sharp edges are smoothed.
- Release of Scalene/Fibrous Attachments: Any remaining attachments of the scalene muscles or fibrous bands to the first rib or surrounding area are released to ensure complete decompression.
- Inspection: The surgeon inspects the area for complete decompression and hemostasis.
Wound Closure
- Hemostasis.
- A chest tube may be inserted if a pneumothorax occurred.
- Drain placement (suction drain) is common.
- Closure of subcutaneous tissue and skin.
3. Infraclavicular Approach (Pectoralis Minor Release)
This approach is used for subcoracoid compression and typically involves releasing the pectoralis minor tendon. It is rarely performed in isolation but can be an adjunct to other approaches.
- Incision: A deltopectoral incision or a short transverse incision over the coracoid process.
- Pectoralis Minor Tenotomy: The pectoralis minor muscle is identified, and its tendon, inserting onto the coracoid process, is divided. This releases the tension on the neurovascular bundle in the subcoracoid space.
Vascular Considerations During Surgery
- vTOS: After first rib resection, venolysis (lysis of perivenous scar tissue) is performed. If chronic stenosis or occlusion persists, venoplasty (balloon dilation) or stenting may be required. In rare cases, vein bypass or patch angioplasty may be indicated.
- aTOS: After decompression, the subclavian artery is inspected. If an aneurysm or significant stenosis is present, arterial repair (e.g., primary repair, patch angioplasty with saphenous vein, interposition graft with saphenous vein or synthetic graft) is performed.

Complications & Management
TOS surgery, while effective, carries a risk of significant complications due to the proximity of vital neurovascular structures. Surgeons must be adept at preventing and managing these adverse events.
Common Complications and Management Strategies
| Complication | Incidence (Approx.) | Clinical Presentation | Management Strategy |
|---|---|---|---|
| Nerve Injuries | |||
| Long Thoracic Nerve (LTN) | 1-5% | Scapular winging, weakness in shoulder abduction | Conservative management initially (PT, bracing). Surgical repair/neurolysis rarely indicated. Most improve spontaneously over months. |
| Phrenic Nerve | 0.5-2% | Diaphragmatic paralysis (dyspnea, particularly supine) | Often asymptomatic or transient. Observe. Surgical plication of diaphragm if severe and persistent dyspnea. |
| Brachial Plexus (direct) | <1% | Acute motor/sensory deficits, severe pain (neuropathic) | Prevention is key (careful dissection, neuromonitoring). Immediate re-exploration if severe, focal deficit post-op; neurolysis or repair if indicated. Intensive rehabilitation. |
| Dorsal Scapular Nerve | Rare | Weakness of rhomboids (scapular dyskinesis) | Conservative (PT). |
| Intercostobrachial Nerve | 5-15% | Numbness/paresthesias in axilla/medial arm | Common with transaxillary approach. Generally well-tolerated and resolves or diminishes over time. Neuropathic pain medication if severe. |
| Supraclavicular Nerves | 5-10% | Numbness over supraclavicular fossa/neck | Common with supraclavicular approach. Generally sensory, transient. |
| Vascular Injuries | |||
| Subclavian Artery/Vein | <1% | Hemorrhage, pseudoaneurysm, AV fistula, thrombosis | Immediate repair (suture repair, patch angioplasty, graft interposition). May require vascular surgeon consultation/involvement. |
| Lymphatic Leak / Chylothorax | 1-2% | Pleural effusion (milky), persistent drainage, respiratory distress | Conservative management initially (low-fat diet, chest tube drainage, somatostatin analogs). Surgical ligation of thoracic duct (supraclavicular approach) if persistent. |
| Pulmonary Complications | |||
| Pneumothorax | 2-5% | Dyspnea, chest pain, diminished breath sounds | Chest tube insertion for drainage. Observation for small, asymptomatic pneumothoraces. |
| Other Complications | |||
| Hematoma/Seroma | 5-10% | Swelling, pain, ecchymosis, drainage | Minor hematomas managed conservatively. Large, expanding, or symptomatic hematomas may require surgical evacuation. |
| Infection | <1% | Erythema, pain, warmth, purulent drainage, fever | Antibiotics. Surgical debridement if deep-seated or associated with implant (rare). |
| Recurrence of Symptoms | 5-20% | Return of pre-operative symptoms | Thorough re-evaluation for alternative diagnoses, incomplete decompression, or re-fibrosis/scarring. Revision surgery may be considered after repeat non-operative treatment and diagnostic confirmation. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Severe pain, swelling, trophic changes, allodynia, hyperalgesia | Aggressive multimodal pain management (PT, neuropathic agents, regional blocks, psychological support). Early recognition is crucial. |
| Scar Pain | Variable | Persistent pain along incision line | Local anesthetic injections, neuropathic pain medication. Rare surgical revision of scar. |
Salvage Strategies for Specific Complications
- Persistent Pneumothorax: If initial chest tube insertion fails, consider video-assisted thoracoscopic surgery (VATS) for pleurodesis or direct repair of a lung parenchymal leak.
- Recurrent TOS Symptoms: A thorough diagnostic reassessment is paramount. Imaging (MRI neurogram, dynamic CTA/MRA) can help identify persistent compression, scar tissue, or new anatomical issues. Repeat scalene blocks can be diagnostic. Revision surgery is technically more challenging due to scar tissue but can be effective in carefully selected patients. The supraclavicular approach is generally preferred for revision surgery as it allows for better identification and release of scar tissue around the brachial plexus.
- Venous Thrombosis Post-Surgery: Requires immediate anticoagulation and may necessitate repeat thrombolysis or venoplasty/stenting. Ensure adequate first rib resection and venolysis during the primary procedure.
- Lymphedema Post-Surgery: Especially after extensive axillary dissection. Managed with compression garments, manual lymphatic drainage, and meticulous skin care.
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation program is integral to achieving optimal functional outcomes and preventing long-term sequelae following TOS decompression surgery. Rehabilitation should be multidisciplinary, involving physical and occupational therapists experienced in TOS.
Immediate Post-Operative Phase (Days 0-7)
- Pain Management: Aggressive use of multimodal analgesia (NSAIDs, acetaminophen, nerve blocks, opioids) to facilitate early mobilization.
- Wound Care: Keep incision clean and dry. Monitor for signs of infection or hematoma/seroma.
-
Early Mobilization:
- Gentle Neck Range of Motion (ROM): Cervical flexion, extension, lateral bending, and rotation within pain-free limits.
- Shoulder Girdle Mobility: Passive and active-assisted ROM of the shoulder, emphasizing flexion and abduction to 90 degrees, and external rotation. Avoidance of extreme abduction or external rotation that may stress the surgical site, especially if the transaxillary approach was used.
- Elbow/Wrist/Hand ROM: Active ROM to prevent stiffness.
- Diaphragmatic Breathing: Crucial, especially if there was any phrenic nerve manipulation or suspicion of a subclinical pneumothorax. Emphasize abdominal breathing to minimize accessory muscle use.
- Postural Education: Gentle cues for neutral spine and shoulder alignment.
Early Rehabilitation Phase (Weeks 1-4)
- Gradual Increase in ROM: Progress shoulder ROM (flexion, abduction, rotation) towards full physiological limits, respecting pain.
-
Gentle Stretching:
- Scalene Stretches: Gentle contralateral neck flexion and rotation to stretch the ipsilateral scalenes.
- Pectoralis Stretches: Doorway stretches to open the costoclavicular space.
- Nerve Gliding Exercises: Specific exercises (e.g., median, ulnar, radial nerve glides) to prevent tethering of the brachial plexus in the healing scar tissue.
- Scapular Stabilization Exercises: Begin isometric exercises for scapular retractors (rhomboids, middle/lower trapezius) to improve shoulder girdle mechanics and posture.
- Ergonomic Assessment: Review and modify daily activities and workstation setup to maintain optimal posture and avoid aggravating positions.
- Light Cardio: Walking, stationary bike.
Intermediate Rehabilitation Phase (Weeks 4-12)
-
Progressive Strengthening:
- Shoulder Girdle: Begin light resistance exercises for all shoulder girdle muscles (rotator cuff, deltoid, serratus anterior, trapezius). Focus on controlled movements and good form.
- Core Strengthening: Essential for maintaining upright posture and reducing cervical and shoulder strain.
- Advanced Nerve Gliding: Progress to more dynamic nerve gliding exercises.
- Endurance Training: Increase duration and intensity of cardiovascular exercise.
- Functional Activities: Incorporate activities of daily living and work-related tasks, gradually increasing load and complexity.
- Proprioceptive Training: Balance and coordination exercises for the upper extremity and trunk.
Advanced Rehabilitation Phase (Months 3+)
- Return to Full Activity: Gradual return to full work, recreational, and sport-specific activities.
- Sport-Specific Training: For athletes, incorporate sport-specific movements and drills.
- Maintenance Program: Lifelong emphasis on good posture, regular stretching, and maintenance strengthening to prevent recurrence.
- Avoidance of Overuse: Educate patients on body mechanics and avoiding repetitive, aggravating overhead or sustained arm positions.
- Scar Management: Massage and desensitization of the surgical scar.
Throughout all phases, therapists monitor for signs of neuropathic pain, CRPS, or symptom recurrence, adjusting the program as needed. Patient education regarding the chronic nature of TOS and the importance of continued self-management is critical for long-term success.
Summary of Key Literature / Guidelines
The literature on Thoracic Outlet Syndrome reflects a complex and evolving understanding of its diagnosis, classification, and management. While consensus exists on certain aspects, debate continues regarding objective diagnostic criteria for nTOS and optimal surgical approaches.
Diagnostic Criteria and Challenges in nTOS
- The Society for Vascular Surgery (SVS) guidelines (2016) emphasize the largely clinical diagnosis of nTOS. They highlight the unreliability of most provocative maneuvers alone for definitive diagnosis and the often normal findings on EMG/NCS. The cornerstone for nTOS diagnosis remains a compelling clinical history of upper extremity pain and paresthesias, reproduction of symptoms with specific provocative maneuvers, and exclusion of other pathologies.
- Diagnostic Scalene Blocks: Multiple studies, including systematic reviews, support the utility of a positive diagnostic anterior scalene block (significant temporary symptom relief) as a strong predictor of surgical success and an essential part of the diagnostic algorithm for nTOS. This is particularly relevant given the often subjective nature of nTOS symptoms.
Non-Operative Management
- First-Line Treatment: Current literature consistently supports comprehensive non-operative management as the initial approach for nTOS, lasting at least 3-6 months. This typically involves physical therapy focusing on postural correction, scapular stabilization, stretching of tight muscles (scalenes, pectoralis), and nerve gliding exercises.
- Botulinum Toxin: Several studies suggest that botulinum toxin injections into the scalene muscles can provide temporary relief in nTOS, potentially serving as a diagnostic adjunct or a temporizing measure for patients not yet ready for surgery or as an alternative for non-responders to conventional PT.
Surgical Efficacy and Approaches
- Overall Success Rates: Surgical decompression for TOS, when indicated and performed by experienced surgeons, demonstrates favorable outcomes. Success rates (defined as significant symptom improvement) range from 70-90% for nTOS, and are generally higher for aTOS and vTOS due to more objective pathology.
-
Supraclavicular vs. Transaxillary Approaches:
- Supraclavicular Approach: Literature suggests this approach offers superior visualization of the brachial plexus, subclavian artery, and cervical rib/fibrous bands. It allows for a more complete anterior and middle scalenectomy and neurolysis. It is often preferred for aTOS, revision surgery, and cases with definite cervical ribs. Complication rates, particularly for phrenic nerve palsy, are slightly higher but generally transient.
- Transaxillary Approach: Favored by some for its cosmetic incision and direct access to the first rib. However, visualization of the brachial plexus and vascular structures is more limited, increasing the risk of incomplete decompression, especially in cases with complex anatomy or fibrous bands. Its primary utility is for first rib resection when the pathology is predominantly bony compression. Long-term outcomes for nTOS are comparable if complete decompression is achieved.
- Role of First Rib Resection: While anterior scalenectomy is considered the cornerstone for nTOS, first rib resection is increasingly performed, especially for patients with significant lower trunk compression against the rib, or for arterial and venous TOS. The SVS guidelines advocate for first rib resection in most cases of aTOS and vTOS following thrombolysis.
- Recurrence: Recurrence of symptoms, often due to scar tissue formation or incomplete initial decompression, is reported in 5-20% of patients. Revision surgery is technically more challenging and requires careful patient selection and expert surgical technique, often utilizing the supraclavicular approach.
Vascular TOS Specifics
- Paget-Schroetter Syndrome (vTOS): The SVS guidelines strongly recommend a staged approach: initial catheter-directed thrombolysis (CDT) for acute thrombosis, followed by first rib resection and venolysis, and then venoplasty or stenting if residual stenosis is present. Anticoagulation is critical throughout this process.
- Arterial TOS (aTOS): Prompt diagnosis and surgical intervention (first rib resection with vascular reconstruction if necessary) are crucial to prevent limb-threatening ischemia or distal embolization, particularly in the presence of a cervical rib or subclavian artery aneurysm.
Conclusion
TOS remains a challenging condition requiring a high index of suspicion, a meticulous diagnostic approach, and a tailored management strategy. While non-operative treatment is the initial step for nTOS, surgery offers effective relief for refractory cases and is often essential for vascular forms. The choice of surgical approach depends on the specific pathology, surgeon expertise, and patient anatomy, with current literature supporting both supraclavicular and transaxillary approaches in carefully selected populations. Continued research is vital to refine objective diagnostic criteria and optimize treatment protocols for this complex disorder.
Clinical & Radiographic Imaging

You Might Also Like