Spinal Stability: Comprehensive Assessment Using Denis Model & White-Punjabi Criteria
Key Takeaway
Spinal stability assessment determines if an injury causes further neurologic damage, chronic pain, or deformity. It involves understanding spinal biomechanics, like the Denis three-column model, which evaluates anterior, middle, and posterior column integrity. The White and Punjabi criteria further assess instability based on radiographic and clinical parameters, guiding appropriate management to prevent secondary neural injury.
Spinal Stability: Assess Spinal Injury & Prevent Damage
Introduction & Epidemiology
Spinal stability is a fundamental concept in orthopedic surgery, particularly in the management of spinal trauma and degenerative conditions. A spinal injury is considered unstable if normal physiologic loads cause further neurologic damage, chronic pain, and unacceptable deformity. The primary goal of evaluating spinal injuries is to accurately determine stability to guide appropriate management, thereby preventing secondary neural injury, progressive deformity, and chronic pain.
Spinal fractures represent a significant public health burden. Thoracolumbar fractures are the most common, accounting for approximately 50-60% of all spinal fractures, with an estimated incidence of 64 cases per 100,000 population annually. Cervical spine injuries, while less frequent (around 10-20% of all spinal fractures), carry a higher risk of severe neurological deficits due to the critical nature of the cervical spinal cord. Lumbar and sacral fractures constitute the remainder. High-energy trauma mechanisms, such as motor vehicle collisions and falls from height, are common etiologies, especially in younger populations. Osteoporosis and metastatic disease contribute significantly to spinal fractures in older individuals, often from low-energy mechanisms. The accurate assessment of stability, rooted in a thorough understanding of spinal biomechanics and validated classification systems, is paramount for optimizing patient outcomes.
Surgical Anatomy & Biomechanics
Understanding the complex interplay of osseous and ligamentous structures is critical for appreciating spinal stability. The spine functions as a flexible column, providing support, protecting the spinal cord, and allowing for a wide range of motion. Stability is derived from the integrity of its three main components: the vertebral bodies, the posterior arch elements (pedicles, laminae, facets, spinous process), and the connecting ligaments and discs.
Denis Three-Column Model
The Denis three-column model, first described in 1983, revolutionized the understanding and classification of thoracolumbar fractures. It posits that the spine can be functionally divided into three distinct columns:
- Anterior Column: Composed of the anterior longitudinal ligament (ALL), the anterior two-thirds of the vertebral body, and the anterior half of the annulus fibrosus. This column primarily resists compressive and distracting forces.
- Middle Column: Composed of the posterior longitudinal ligament (PLL), the posterior one-third of the vertebral body, and the posterior half of the annulus fibrosus. This is the critical column for stability; failure often leads to instability and potential neural compromise.
- Posterior Column: Composed of the posterior bony elements (pedicles, laminae, articular facets, and spinous processes) and the posterior ligamentous complex (PLC), which includes the ligamentum flavum, interspinous and supraspinous ligaments, and facet joint capsules. This column primarily resists tensile and shear forces, and its integrity is a major determinant of stability.
An injury involving only the anterior column is typically stable. However, an injury to two or more columns, particularly if the middle column is involved, strongly suggests mechanical instability. Disruption of the middle column's posterior wall, leading to retropulsed bone fragments, often correlates with spinal canal compromise. Similarly, significant disruption of the Posterior Ligamentous Complex (PLC) in conjunction with bony injury often indicates instability, even if the bony injury itself appears minor.
Illustrations of the Denis Three-Column Model and Spinal Anatomy:

Figure 1: Lateral view illustrating the anterior, middle, and posterior columns as defined by Denis.

Figure 2: Axial view demonstrating the components contributing to each spinal column.

Figure 3: Detailed lateral view highlighting the anatomical structures within each column.

Figure 4: Sagittal anatomical representation of the vertebral column emphasizing the three-column concept.

Figure 5: Coronal view illustrating the bony architecture of vertebral segments.
White and Punjabi Clinical Instability Criteria
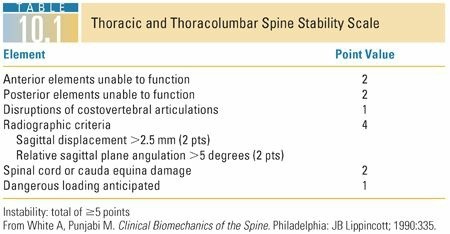
Prior to Denis' work, White and Punjabi developed a comprehensive, biomechanically-driven scoring system for assessing clinical instability, particularly in the cervical spine. Their system assigns points based on various radiographic and clinical parameters, with a higher score indicating greater instability. While initially focused on the cervical spine, the underlying biomechanical principles extend to the entire spinal column. The criteria consider:
- Anterior element destruction: Degree of vertebral body or disc disruption.
- Posterior element destruction: Disruption of facet joints, laminae, or spinous processes.
- Sagittal Plane Translation: Horizontal displacement of one vertebra relative to another.
- Sagittal Plane Angulation: Angular deformity between vertebral bodies.
- Spinal Cord or Nerve Root Injury: Presence and severity of neurological deficit.
- Facet Dislocation/Perched Facets: Indicative of significant ligamentous disruption.
- Interspinous Ligament Widening: A direct sign of PLC disruption.
For the cervical spine, a total score of 5 points or more typically indicates clinical instability requiring surgical stabilization. Similar principles apply to the thoracolumbar spine, albeit with adjusted scoring thresholds and parameters in some adaptations.
Illustrations of White and Punjabi Clinical Instability Criteria:

Figure 6: Table presenting specific radiographic and clinical criteria for spinal instability as proposed by White and Punjabi (part 1 of 3).

Figure 7: Table presenting specific radiographic and clinical criteria for spinal instability as proposed by White and Punjabi (part 2 of 3).

Figure 8: Table presenting specific radiographic and clinical criteria for spinal instability as proposed by White and Punjabi (part 3 of 3).
Modern Classification Systems
Building upon the foundations of Denis and White & Punjabi, more contemporary classification systems have emerged, integrating injury morphology, neurological status, and the integrity of the posterior ligamentous complex (PLC). The
Thoracolumbar Injury Classification and Severity Score (TLICS)
and the
Subaxial Cervical Spine Injury Classification System (SLIC)
are prime examples. Both systems assign points for:
*
Injury Morphology:
Compression, burst, distraction, rotation/translation.
*
Posterior Ligamentous Complex (PLC) Integrity:
Assessed primarily by MRI.
*
Neurological Status:
Intact, root injury, incomplete cord injury, complete cord injury.
A cumulative score above a certain threshold (e.g., ≥ 5 for TLICS, ≥ 4 for SLIC) typically indicates a strong recommendation for surgical intervention, while lower scores often suggest non-operative management. These systems provide a more nuanced, evidence-based approach to decision-making, emphasizing the importance of soft tissue integrity and neurological function alongside bony architecture.
Indications & Contraindications
The decision for operative versus non-operative management of spinal injuries is multifactorial, balancing the risks of surgery against the potential for progressive instability, neurological deterioration, and chronic pain.
Operative Indications
- Mechanical Instability: Defined by established classification systems (e.g., White & Punjabi score ≥5 for cervical, TLICS ≥5, SLIC ≥4), indicating a high risk of future neurological compromise or deformity under physiologic loads.
- Progressive Neurological Deficit: Any new or worsening neurological deficit mandates urgent surgical decompression and stabilization.
- Significant Spinal Canal Compromise: Often >30-50% canal obliteration by bony fragments or disc material, particularly in the setting of neurological deficit or high-risk fracture patterns (e.g., unstable burst fractures).
- Irreducible Deformity: Angulation exceeding physiological limits (e.g., kyphosis >20-30 degrees in the thoracolumbar spine), particularly if progressive.
- Gross Ligamentous Instability: Complete disruption of the posterior ligamentous complex (PLC), often seen with distraction or translation injuries, even with minimal bony injury.
- Persistent Intractable Pain: In certain stable fractures where non-operative management has failed to alleviate severe pain attributed to the injury.
- Failure of Non-Operative Management: Progressive deformity or neurological deficit despite appropriate bracing and conservative care.
Non-Operative Indications
- Stable Fracture Patterns: Injuries demonstrating inherent stability, often involving only the anterior column or stable two-column injuries without significant ligamentous disruption. Examples include isolated transverse process fractures, stable wedge compression fractures (<40-50% height loss, <20 degrees kyphosis, intact PLC), or stable burst fractures without neurological deficits and minimal canal compromise.
- Intact Neurological Status: No signs of spinal cord or nerve root compromise.
- No Significant Canal Compromise: Minimal retropulsion of fragments into the spinal canal.
- Ability to Tolerate Bracing/Immobilization: Patient compliance and tolerance for external support.
- Absence of Progressive Deformity: On serial radiographic imaging.
Contraindications for Operative Intervention
- Severe Comorbidities: Medical conditions that significantly increase anesthetic and surgical risk, outweighing the potential benefits of surgery.
- Terminal Illness: Limited life expectancy where the morbidity of surgery is not justified.
- Patient Refusal: After comprehensive informed consent and discussion of risks/benefits.
- Stable Fracture Patterns: As outlined above, if the injury does not meet operative criteria and is manageable non-operatively.
- Severe Local Infection: Active infection at the surgical site, requiring resolution prior to elective stabilization.
Summary of Indications
| Feature | Operative Management | Non-Operative Management |
|---|---|---|
| Mechanical Stability | Unstable (TLICS ≥5, SLIC ≥4, White & Punjabi ≥5, or gross instability) | Stable (TLICS <5, SLIC <4, White & Punjabi <5, or inherently stable fracture patterns) |
| Neurological Status | Progressive deficit, complete/incomplete cord injury, nerve root injury | Intact neurological status |
| Spinal Canal Compromise | Significant (>30-50%), especially with neurological deficit | Minimal or no compromise, no neurological deficit |
| Deformity | Progressive kyphosis/scoliosis, unacceptable angular deformity (e.g., kyphosis >20-30° in thoracolumbar) | No significant or progressive deformity (e.g., kyphosis <20-25° in thoracolumbar, stable on dynamic imaging if allowed) |
| Ligamentous Integrity | Disrupted Posterior Ligamentous Complex (PLC) | Intact PLC (critical for stability) |
| Pain | Intractable pain refractory to conservative care (rarely sole indication, usually with other instability factors) | Managed effectively with conservative measures |
| Patient Factors | Good surgical candidate, compliant | Significant comorbidities precluding surgery, non-compliant with bracing (if required) |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to ensure patient safety and optimize surgical outcomes.
Imaging Assessment
- Plain Radiographs: Initial assessment (AP, lateral, oblique views) for alignment, vertebral body height, facet integrity, and interspinous widening. Flexion-extension views may be considered in stable-appearing injuries without neurological deficit to assess occult ligamentous instability, but with extreme caution.
- Computed Tomography (CT) Scan: Gold standard for bony detail, fracture morphology, spinal canal compromise, and facet involvement. 3D reconstructions are invaluable for understanding complex fracture patterns and surgical planning.
- Magnetic Resonance Imaging (MRI): Essential for evaluating soft tissue injuries, particularly posterior ligamentous complex (PLC) disruption, disc herniation, epidural hematoma, and direct spinal cord damage (contusion, edema, transection). MRI is paramount for assessing neurological injury and guiding decompression strategies.
Medical Optimization
- Comprehensive medical workup including cardiovascular, pulmonary, renal, and endocrine assessment.
- Management of comorbidities to minimize surgical risk.
- Type and screen for potential blood loss.
Neurophysiological Monitoring
- Somatosensory Evoked Potentials (SSEPs): Monitor dorsal column function.
- Motor Evoked Potentials (MEPs): Monitor corticospinal tract function; generally more sensitive for motor pathway compromise.
- Electromyography (EMG): Used to identify nerve root irritation or injury.
- These modalities are crucial for real-time assessment of neurological function during deformity correction and instrumentation, providing early warning signs of potential iatrogenic injury.
Surgical Strategy
-
Approach:
Anterior, posterior, or combined. Determined by fracture location, need for decompression, desired biomechanical stability, and surgeon preference.
- Anterior: Direct decompression of anterior canal compromise, restoration of anterior column support.
- Posterior: Indirect decompression (ligamentotaxis), direct decompression (laminectomy), posterior tension band fixation.
- Combined: For severe pan-column injuries requiring extensive decompression, reduction, and circumferential stabilization.
- Fusion Levels: Consideration of fusion length to maximize stability while preserving motion segments. Generally, fusion should encompass the injured segment and sufficient adjacent levels to provide stable fixation and prevent adjacent segment disease.
- Instrumentation: Pedicle screws are the workhorse for thoracolumbar and sacral fixation. Cervical instrumentation includes anterior plates, posterior lateral mass screws, and pedicle screws (C7-T1).
- Decompression Strategy: Direct (removing offending elements) vs. indirect (distraction, ligamentotaxis).
Patient Positioning
-
Prone Positioning (for Posterior Approaches):
- Careful log-roll onto a specialized radiolucent table (e.g., Jackson table, OSI Spinal Table).
- Ensure the abdomen is free to minimize intra-abdominal pressure, reduce epidural venous bleeding, and optimize hemodynamics.
- Chest rolls or frame supports positioned to allow free abdominal excursion and prevent lung compression.
- Head and neck maintained in neutral alignment, secured with a Mayfield clamp (cervical) or padded headrest.
- All pressure points (knees, ankles, shoulders, elbows) well-padded to prevent nerve palsies or skin breakdown.
- Arms abducted <90 degrees, forearms supinated, palms down.
- Ensure adequate fluoroscopy access.
-
Supine Positioning (for Anterior Cervical Approaches):
- Head in neutral or slight extension, supported by a gel donut.
- Shoulders taped caudally to improve C7-T1 visualization on fluoroscopy.
-
Lateral Decubitus Positioning (for Lateral Thoracolumbar Approaches):
- Patient positioned with the side of approach facing upwards.
- Axillary roll to protect brachial plexus.
- Pillows between knees.
- Beanbag or similar device for stability.
Detailed Surgical Approach / Technique
The specific surgical approach varies significantly depending on the spinal segment, fracture type, and desired goals (decompression, reduction, stabilization). However, core principles apply.
General Principles of Spinal Stabilization Surgery
- Adequate Exposure: Obtain sufficient anatomical landmarks to perform the procedure safely and effectively.
- Decompression of Neural Elements: Release any impingement on the spinal cord or nerve roots, whether by bone, disc, or hematoma.
- Restoration of Spinal Alignment: Realign the spine to its physiological curvature (sagittal and coronal balance).
- Stable Internal Fixation: Employ instrumentation to provide immediate stability and hold the reduction.
- Achieve Arthrodesis (Fusion): Promote bony union across the unstable segment(s) to provide long-term stability.
Posterior Thoracolumbar Fusion (Example: Unstable Burst Fracture)
-
Incision and Dissection:
- Midline skin incision centered over the fractured segment and adjacent levels to be instrumented.
- Subcutaneous dissection to the thoracolumbar fascia.
- Incision of the thoracolumbar fascia in the midline.
- Subperiosteal dissection of the paraspinal muscles (erector spinae) off the spinous processes, laminae, and transverse processes using monopolar cautery and Cobb elevators. This maintains the internervous plane.
- Exposure extends laterally to the facet joints and medially to the base of the transverse processes, at least two levels above and two levels below the fractured vertebra for standard pedicle screw fixation.
-
Decompression (Laminectomy/Laminotomy):
- For direct decompression of retropulsed bone fragments or disc material: perform a laminectomy at the level of maximal canal compromise.
- Carefully remove ligamentum flavum to expose the dura.
- Using small Kerrison rongeurs and curettes, gently remove posterior vertebral body fragments or disc material causing neural compression. This is often performed after initial distraction and reduction to create more space.
- Indirect decompression can be achieved via ligamentotaxis by applying distraction through pedicle screws, which pulls posterior elements and disc material anteriorly away from the canal.
-
Reduction:
- Pedicle screws are inserted two levels above and two levels below the fractured vertebra, and sometimes one level above and one level below depending on the fracture severity and stability. The trajectory is critical to avoid neural or vascular injury.
- A pilot hole is created with an awl. Pedicle feelers confirm bony margins.
- Screws are placed with careful palpation of bony walls.
- Contouring of two rods (one for each side) to match the desired anatomical lordosis/kyphosis.
- Rods are seated into the screw heads.
- Distraction, compression, or translation maneuvers are applied using rod manipulators and persuaders to reduce the fracture and restore alignment. This can involve reducing kyphosis and de-rotating segments.
- The screws are then tightened to the rods.
-
Fixation and Fusion:
- After reduction and fixation, the posterior elements (transverse processes, laminae, facets) are decorticated using a high-speed burr to create a bleeding bone bed.
- Autograft (local bone from laminectomy or iliac crest) or allograft (demineralized bone matrix, cancellous chips) is packed over the decorticated surfaces to promote fusion.
- In cases of anterior column deficiency (e.g., corpectomy), anterior column reconstruction with a cage or structural allograft is often performed via a staged combined approach.
Anterior Cervical Discectomy and Fusion (ACDF) / Corpectomy and Fusion (Example: Cervical Burst Fracture with Anterior Cord Compression)
-
Incision and Dissection:
- A transverse skin incision is made along a skin crease, typically on the right side.
- Platysma muscle is divided transversely.
- The interval between the sternocleidomastoid muscle laterally and the strap muscles (sternohyoid, sternothyroid) and trachea/esophagus medially is developed.
- The carotid sheath is retracted laterally.
- The prevertebral fascia is identified and incised longitudinally to expose the anterior aspect of the vertebral bodies and discs.
-
Decompression:
- For discectomy: The target disc is removed, including posterior osteophytes and any herniated fragments compressing the cord or nerve roots.
- For corpectomy: The vertebral body is resected using a high-speed burr and Kerrison rongeurs to decompress the spinal cord directly. The posterior longitudinal ligament (PLL) is often removed to ensure complete decompression.
-
Grafting and Fixation:
- After decompression, an appropriately sized interbody graft (e.g., PEEK cage, allograft, autograft fibula) is inserted into the created defect to restore disc height and anterior column support.
- An anterior cervical plate is then applied to the adjacent vertebral bodies and secured with screws, providing immediate stability and promoting fusion.
Complications & Management
Spinal surgery, while often life-saving and function-restoring, carries inherent risks of complications.
Intraoperative Complications
-
Neurological Injury:
- Incidence: Varies, generally <1-2% for transient deficits, lower for permanent. Higher in revision surgery or complex deformities.
- Management: Immediate recognition via neurophysiological monitoring. Stop surgical maneuver, assess implant position, adjust alignment, remove impinging structures. Intraoperative imaging. Wake-up test (if feasible). Post-operative MRI.
-
Vascular Injury:
- Incidence: Rare but potentially catastrophic (e.g., aorta, vena cava, segmental vessels, carotid artery).
- Management: Direct pressure, consultation with vascular surgery, control of bleeding, repair of vessel.
-
Dural Tear / CSF Leak:
- Incidence: 1-10%, more common in revision surgery or multilevel decompression.
- Management: Primary repair with suture (e.g., 6-0 Prolene), dural sealant, fat graft, muscle patch. Strict bed rest post-op, avoidance of Valsalva maneuvers, possible lumbar drain.
-
Visceral Injury:
- Incidence: Rare (e.g., esophagus, trachea, bowel, ureter, diaphragm). More common with anterior approaches.
- Management: Immediate recognition, primary repair by general/thoracic surgeon, antibiotics.
-
Instrumentation Malposition / Failure:
- Incidence: <5% for minor malposition; significant malposition causing neural/vascular compromise is rare.
- Management: Intraoperative fluoroscopy/navigation to verify position. Revision or removal of hardware if malpositioned or loose.
Postoperative Complications
-
Infection:
- Incidence: Superficial (1-5%), Deep (0.5-2%). Higher in open fractures, prolonged surgery, or immunocompromised patients.
- Management: Superficial: wound care, oral antibiotics. Deep: surgical debridement, IV antibiotics, possibly hardware removal (after fusion).
-
Hardware Failure:
- Incidence: 2-10%, including screw pullout, rod fracture, migration. Often associated with pseudarthrosis.
- Management: Revision surgery with removal of failed hardware, new instrumentation, extended fusion, and aggressive bone grafting.
-
Pseudarthrosis / Non-Union:
- Incidence: 5-15%, higher in smokers, multi-level fusions, or patients with poor bone quality.
- Management: Non-operative (electrical stimulation, bracing) for asymptomatic. Revision surgery with refusion, additional instrumentation, and potent bone graft substitutes (e.g., BMP) for symptomatic non-unions.
-
Adjacent Segment Disease (ASD):
- Incidence: 2-4% per year after fusion, up to 20-30% within 10 years.
- Management: Non-operative initially (PT, injections). If symptoms persist or neurological compromise, surgical intervention (decompression, fusion, or disc replacement at the adjacent level).
-
Persistent Pain / Neurological Deficit:
- Incidence: Variable, depends on pre-op status and extent of injury.
- Management: Thorough workup to identify cause (hardware issues, non-union, new compression). Non-operative pain management, physical therapy. May require revision surgery.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: DVT 1-5%, PE 0.5-2%. Higher in trauma, malignancy, prolonged immobilization.
- Management: Prophylactic anticoagulation, early mobilization. Treatment with therapeutic anticoagulation, IVC filter for recurrent PE or contraindication to anticoagulation.
-
Ileus:
- Incidence: Common after anterior thoracolumbar surgery.
- Management: NPO, nasogastric tube decompression, prokinetics.
-
Dysphagia:
- Incidence: Common after anterior cervical surgery (up to 70% transiently, <5% chronic severe).
- Management: Soft diet, speech therapy, corticosteroids.
-
Retrograde Ejaculation:
- Incidence: <1% after anterior L5-S1 approach due to sympathetic nerve plexus injury.
- Management: Counseling, often permanent.
Summary of Complications & Management
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Intraoperative | ||
| Neurological Injury | <1-2% | Immediate assessment, adjust hardware, direct decompression, post-op MRI, wake-up test. |
| Vascular Injury | Rare | Direct pressure, vascular surgery consult, repair. |
| Dural Tear / CSF Leak | 1-10% | Primary repair, dural sealants, fat graft, strict bed rest, lumbar drain. |
| Visceral Injury | Rare | Immediate repair by appropriate surgical specialist, antibiotics. |
| Instrumentation Malposition/Failure | <5% | Intraoperative correction, revision of hardware placement. |
| Postoperative | ||
| Infection (deep) | 0.5-2% | Surgical debridement, IV antibiotics, possible hardware removal after fusion. |
| Hardware Failure | 2-10% | Revision surgery, new instrumentation, extended fusion, aggressive bone grafting. |
| Pseudarthrosis / Non-Union | 5-15% | Non-operative (electrical stimulation) or revision surgery with refusion, potent bone graft. |
| Adjacent Segment Disease (ASD) | 2-4% / year | Non-operative (PT, injections) or surgical intervention (decompression, fusion at adjacent level). |
| Persistent Pain | Variable | Thorough workup, non-operative pain management, physical therapy, possible revision surgery. |
| DVT / PE | 1-5% / 0.5-2% | Prophylactic anticoagulation, early mobilization. Therapeutic anticoagulation, IVC filter for treatment. |
| Ileus | Common | NPO, NG tube decompression, prokinetics. |
| Dysphagia (post-ACDF) | Up to 70% transiently | Soft diet, speech therapy, corticosteroids. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to maximizing functional recovery, preventing complications, and facilitating a safe return to activity. Protocols are individualized based on the patient's age, comorbidities, type of injury, extent of surgery, and fusion achieved.
Phase 1: Acute/Protective (Weeks 0-6)
- Goals: Pain control, wound healing, protecting the surgical construct, early mobilization, preventing deconditioning.
-
Activity:
- Mobilization: Ambulation initiated within 24-48 hours post-surgery, with assistance as needed. Log-roll technique for bed mobility.
- Bracing/Orthotics: Applied as indicated for specific fracture patterns or surgical constructs (e.g., TLSO for thoracolumbar fusions, cervical collar for cervical fusions). Duration typically 6-12 weeks, depending on fusion integrity and surgeon preference.
- Restrictions: Strict avoidance of bending, lifting (>5-10 lbs), and twisting (BLT precautions). No heavy lifting, pushing, or pulling. Emphasis on maintaining neutral spinal alignment during all activities.
-
Physical Therapy:
- Gentle range of motion (ROM) exercises for peripheral joints (ankles, knees, hips, shoulders) to prevent stiffness.
- Light isometric contractions for core muscles (abdominal bracing) within pain limits, without spinal flexion/extension.
- Diaphragmatic breathing exercises.
- Education on proper body mechanics and activity modification.
Phase 2: Subacute/Progressive (Weeks 6-12)
- Goals: Gradual increase in spinal mobility (if not fused), progressive strengthening of core and global musculature, improved posture.
-
Activity:
- Gradual weaning from brace/collar as fusion progresses and stability allows (guided by surgeon, often after 6-8 weeks).
- Increase duration and intensity of ambulation.
- Progressive increase in lifting restrictions as tolerated.
-
Physical Therapy:
- Initiate gentle spinal range of motion (for non-fused segments or if fusion is stable).
- Progress core strengthening exercises (e.g., bird-dog, planks, bridges) focusing on stability and control, avoiding excessive spinal loading.
- Balance and proprioception exercises.
- Aerobic conditioning (e.g., stationary bike, elliptical).
- Continue patient education on spinal hygiene.
Phase 3: Return to Activity / Advanced Strengthening (Months 3-6+)
- Goals: Restore full functional capacity, advanced strengthening, return to sport or demanding occupational activities.
-
Activity:
- Full independence in daily activities.
- Gradual return to recreational activities and work, as appropriate.
- Continued adherence to proper body mechanics.
-
Physical Therapy:
- Advanced core and global strengthening (e.g., resistance training, functional movements).
- Sport-specific or work-specific rehabilitation.
- High-level balance and agility drills.
- Progressive weight lifting and impact activities, guided by fusion status and pain.
- Expected Outcomes: Fusion consolidation typically occurs within 3-12 months. Return to unrestricted activities generally within 6-12 months, though some activities may be permanently modified depending on the extent of fusion and pre-injury activity level.
Summary of Key Literature / Guidelines
The management of spinal instability has evolved considerably, driven by advancements in imaging, surgical techniques, and a deeper understanding of spinal biomechanics. Several key principles and classification systems underpin current practice:
-
Classification Systems are Foundational: The Denis Three-Column Model and White and Punjabi Clinical Instability Criteria laid the groundwork for assessing spinal stability. More recently, the TLICS (Thoracolumbar Injury Classification and Severity Score) and SLIC (Subaxial Cervical Spine Injury Classification System) have become the dominant tools, integrating fracture morphology, posterior ligamentous complex (PLC) integrity, and neurological status into a comprehensive decision-making algorithm for operative vs. non-operative management. These systems aim to standardize assessment and improve consistency in treatment recommendations.
-
Importance of PLC Integrity: MRI assessment of the PLC is a critical factor in determining instability, often superseding bony injury patterns alone. PLC disruption significantly increases the instability score in both TLICS and SLIC, pushing the pendulum towards surgical intervention even in apparently less severe bony injuries.
-
Early Surgical Stabilization: For truly unstable spinal injuries, especially those with neurological deficits, early surgical decompression and stabilization are generally favored. This approach aims to prevent further neurological deterioration, reduce pain, facilitate earlier mobilization, and prevent progressive deformity. Numerous studies support that timely intervention (within 24-72 hours) for incomplete spinal cord injury can optimize neurological recovery, though definitive evidence for improved long-term outcomes remains a subject of ongoing research.
-
Minimizing Morbidity: While surgical intervention is often necessary, the focus is on achieving stability with the least invasive approach possible, balancing direct decompression with indirect techniques (e.g., ligamentotaxis). The development of minimally invasive spinal techniques (MIS) for fracture stabilization is a growing area, aiming to reduce surgical trauma, blood loss, and recovery time, though their applicability varies based on fracture complexity and surgeon experience.
-
Evidence-Based Guidelines: Organizations like AOSpine have developed comprehensive classification systems (e.g., AOSpine Thoracolumbar Spine Injury Classification System) and clinical practice guidelines to aid surgeons in navigating complex decisions, promoting standardized, evidence-based care. These guidelines emphasize individualized treatment plans, considering patient factors, fracture characteristics, and available resources.
In conclusion, assessing spinal instability requires a systematic approach, combining clinical evaluation, advanced imaging, and validated classification systems. The goal remains to identify injuries at risk of neurological damage, chronic pain, or progressive deformity, and to intervene appropriately to restore spinal integrity and optimize patient function. Ongoing research continues to refine our understanding and improve treatment paradigms for these often devastating injuries.
