Mastering the Posterior Approach to the Subaxial Cervical Spine
Key Takeaway
For anyone wondering about Mastering the Posterior Approach to the Subaxial Cervical Spine, The posterior approach to the subaxial cervical spine is a commonly used surgical method providing safe access to its posterior elements. It's employed for procedures such as spinal fusion, enlarging the spinal canal (laminectomy/laminoplasty), treating tumors, correcting facet joint dislocations, exploring nerve roots, and fixing fractures. Patients are positioned prone with head flexion for optimal access.
Mastering the Posterior Approach to the Subaxial Cervical Spine
Introduction & Epidemiology
The posterior approach to the subaxial cervical spine (C3-C7) is a foundational technique in orthopedic and neurosurgical spine practices, offering direct access to the posterior osteoligamentous complex and the spinal canal. Its versatility makes it indispensable for a broad spectrum of pathologies, ranging from degenerative conditions to trauma, tumors, and deformities. Historically, posterior cervical procedures have evolved significantly, from rudimentary decompressions to sophisticated instrumentation and fusion constructs that restore sagittal balance and provide robust stability.
The midline posterior approach remains the most commonly employed surgical route to the cervical spine, permitting efficient and safe exposure of the posterior elements across the entire cervical column. Its utility is underscored by its application in:
1. Posterior cervical spine fusion for instability, deformity, or as an adjunct to anterior fusion.
2. Decompression of the spinal canal through laminectomy or laminoplasty in cases of cervical myelopathy or radiculopathy.
3. Resection of posterior element tumors.
4. Reduction and stabilization of facet joint dislocations.
5. Exploration of nerve roots for radiculopathy.
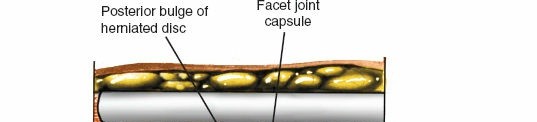
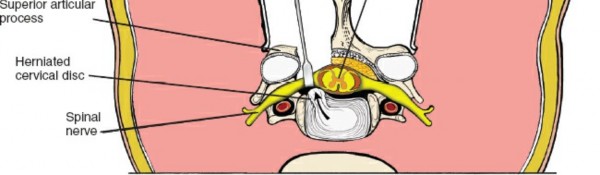
6. Excision of specific posterolateral herniated discs.
7. Open reduction and internal fixation of cervical spine fractures and dislocations.
The incidence of cervical spine pathology requiring surgical intervention is substantial. Degenerative cervical myelopathy, for instance, affects a significant portion of the aging population, with an estimated prevalence of 2-5% in individuals over 50. Traumatic cervical spine injuries, while less common, demand immediate and often complex surgical management. Understanding the nuances of the posterior approach is paramount for all residents and practicing orthopedic surgeons involved in spinal care.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the subaxial cervical spine is critical for safe and effective posterior procedures.
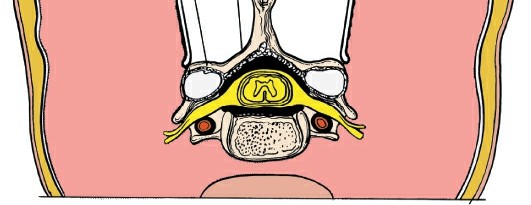
Bony Anatomy
The subaxial cervical vertebrae (C3-C7) share common features:
*
Vertebral Body:
Anteriorly, providing axial load-bearing.
*
Pedicles:
Connect the vertebral body to the posterior elements.
*
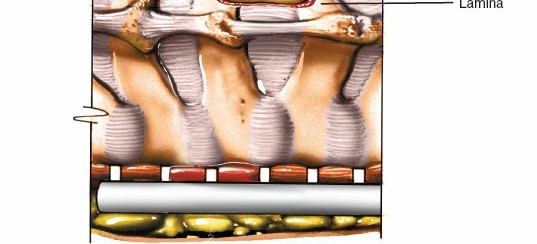
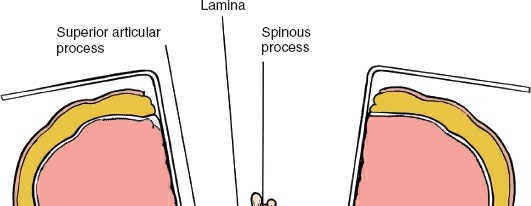
Laminae:
Form the posterior wall of the spinal canal, meeting at the spinous process.
*
Spinous Processes:
Project posteriorly, serving as muscle attachment sites. C7 typically has the longest and most prominent spinous process, often used as a palpable landmark.
*
Articular Pillars / Lateral Masses:
Formed by the superior and inferior articular processes, these are crucial for posterior cervical instrumentation. The facet joints between them are true synovial joints.
*
Transverse Processes:
Contain the foramina transversaria, transmitting the vertebral arteries (from C6 cephalad).
Ligamentous Anatomy
The posterior ligamentous complex provides significant stability:
*
Ligamentum Nuchae:
A thick fibrous septum extending from the external occipital protuberance to C7, continuous with the supraspinous ligament.
*
Supraspinous Ligament:
Connects the tips of the spinous processes.
*
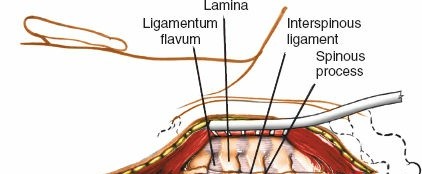
Interspinous Ligament:
Connects adjacent spinous processes.
*
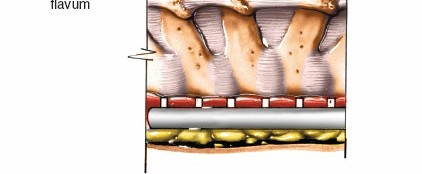
Ligamentum Flavum:
Connects adjacent laminae, characterized by its yellow, elastic properties. Its integrity is crucial for resisting flexion.
*
Capsular Ligaments:
Enclose the facet joints, providing stability and limiting excessive motion.
Muscular Anatomy
A series of muscle layers must be traversed during the posterior approach:
*
Superficial Layer:
Trapezius and sternocleidomastoid.
*
Intermediate Layer:
Splenius capitis, splenius cervicis, levator scapulae.
*
Deep Layer (Intrinsic Back Muscles):
*
Semispinalis Capitis and Cervicis:
Lie superficial to the multifidus.
*
Multifidus:
Lies deep to the semispinalis, attaching to spinous processes and articular pillars.
*
Rotatores, Interspinales, Intertransversarii:
Deepest layers, connecting adjacent vertebrae.
Subperiosteal dissection is typically performed to preserve muscle viability and minimize devascularization, although this varies with the specific technique and extent of exposure required.
Neurovascular Anatomy
- Spinal Cord: The primary structure to protect. Its position within the spinal canal is critical, especially during decompression.
- Cervical Nerve Roots: Emerge through the intervertebral foramina, vulnerable during lateral mass screw placement or foraminotomy. C5 nerve root palsy is a known complication of cervical decompression, particularly after laminoplasty.
- Vertebral Arteries: Traverse the foramina transversaria from C6 upwards. Injury during lateral mass screw placement or extensive lateral dissection is a devastating complication. Their medialization at C1 and C2 makes screw placement in these levels even more precarious.
- Epidural Venous Plexus: Extensive and highly vascularized, contributing significantly to intraoperative bleeding.
Biomechanics
The posterior column contributes significantly to the tensile strength and stability of the cervical spine, resisting flexion.
*
Laminectomy:
Extensive laminectomy without fusion can destabilize the cervical spine, particularly in flexion, and predispose to progressive kyphosis, especially in children and individuals with pre-existing deformity. This risk is higher with removal of more than three laminae.
*
Laminoplasty:
Designed to decompress the spinal cord while maintaining posterior column integrity, thus theoretically reducing the risk of post-laminectomy kyphosis.
*
Posterior Fusion:
Aims to stabilize segments, correct deformity, and promote arthrodesis. Instrumentation (lateral mass screws, pedicle screws) enhances stability and fusion rates. Sagittal balance is a critical consideration in restoring and maintaining spinal alignment.
Indications & Contraindications
The decision for a posterior cervical approach is contingent upon a thorough assessment of the patient's pathology, neurological status, biomechanical stability, and overall health.
Indications for the Posterior Approach
The primary indications for a posterior approach to the subaxial cervical spine include:
-
Degenerative Conditions:
- Multilevel Cervical Spondylotic Myelopathy (CSM): Especially when significant anterior compression cannot be addressed via an anterior approach, or in cases of OPLL (Ossification of the Posterior Longitudinal Ligament) where anterior decompression carries high risk. Laminoplasty or multilevel laminectomy and fusion are common.
- Cervical Radiculopathy: Particularly for multi-level disease, persistent radiculopathy after anterior surgery, or in specific cases of posterolateral disc herniation not amenable to anterior approaches.
-
Trauma:
- Cervical Fractures/Dislocations: For posterior ligamentous complex injuries, unstable fractures (e.g., severe facet disruption, perched/locked facets), or as an adjunct to anterior stabilization.
- Facet Joint Dislocations: Open reduction and internal fixation, often involving direct reduction maneuvers and posterior instrumentation.
-
Deformity:
- Cervical Kyphosis: Correction of kyphotic deformity, especially when flexible or associated with posterior column insufficiency.
- Cervical Spondylolisthesis: Stabilization of translation.
-
Tumors:
- Intradural or Extradural Tumors: When located posteriorly or requiring circumferential decompression.
- Primary Bone Tumors of Posterior Elements: Excision and reconstruction.
-
Infection:
- Posterior Epidural Abscess: Drainage and decompression.
- Revision Surgery: For pseudarthrosis, hardware failure, or adjacent segment disease following previous posterior or anterior procedures.
Contraindications for the Posterior Approach
Absolute contraindications are rare but include:
- Anterior Spinal Cord Compression Not Amenable to Posterior Decompression: If the primary pathology (e.g., large central disc herniation, severe osteophyte formation, tumor) is located predominantly anterior to the spinal cord and cannot be indirectly decompressed by a posterior shift of the cord. Significant fixed kyphosis might also make posterior decompression alone less effective.
- Severe Fixed Cervical Kyphosis: Posterior decompression alone can exacerbate kyphosis. In these cases, a combined anterior-posterior approach or primary anterior approach might be necessary.
- Severe Local Infection: In the surgical field.
- Patient Inability to Tolerate Prone Positioning/Anesthesia: Due to significant comorbidities.
Operative vs. Non-Operative Indications
| Indication Category | Operative Considerations (Posterior Approach) | Non-Operative Considerations |
|---|---|---|
| Degenerative |
- Progressive neurological deficit (myelopathy, severe radiculopathy)
- Multilevel cervical spondylotic myelopathy (CSM) - Opacification of posterior longitudinal ligament (OPLL) - Spinal instability (dynamic imaging) - Persistent pain/radiculopathy despite non-operative treatment |
- Mild to moderate radiculopathy without progressive weakness
- Axial neck pain without neurological deficit - Stable degenerative changes without myelopathy - Initial management with physical therapy, NSAIDs, epidural injections, bracing |
| Trauma |
- Unstable fractures/dislocations (e.g., perched/locked facets, ligamentous disruption)
- Progressive neurological deficit after trauma - Spinal cord injury with ongoing compression - Failure of closed reduction or external immobilization |
- Stable fractures without neurological deficit
- Fractures amenable to external immobilization (e.g., halo vest, rigid collar) - Stable ligamentous injuries without instability on dynamic imaging |
| Deformity |
- Progressive kyphosis causing myelopathy or significant pain
- Fixed kyphosis requiring correction (often combined with anterior surgery) - Sagittal imbalance requiring restoration |
- Mild, non-progressive deformities without neurological compromise or intractable pain
- Flexible kyphosis that responds to conservative measures (e.g., physical therapy) |
| Tumors/Infection |
- Spinal cord compression from posterior/epidural tumor
- Biopsy or excision of posterior element tumors - Epidural abscess causing neurological deficit |
- Small, asymptomatic benign tumors without cord compression
- Localized, non-progressive infections without neurological compromise, managed with antibiotics alone |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and careful patient positioning are paramount to optimize surgical outcomes and minimize complications.
Pre-Operative Assessment
- Clinical Evaluation: A detailed history focusing on neurological symptoms, pain characteristics, and functional limitations. A comprehensive neurological examination, including motor strength, sensory assessment, reflexes, and gait analysis, is essential.
-
Imaging Studies:
- Plain Radiographs: Anteroposterior, lateral, and flexion/extension views to assess alignment, instability, and gross osseous pathology.
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating soft tissue pathology, spinal cord compression, disc herniations, ligamentous injury, and intrinsic cord changes (e.g., T2 signal hyperintensity indicative of myelomalacia).
- Computed Tomography (CT) Scan: Provides superior bony detail, crucial for evaluating fractures, osteophytes, ossification of ligaments (OPLL), and pedicle/lateral mass morphology for instrumentation planning. 3D reconstructions are highly valuable for complex anatomy.
- CT Angiography (CTA): May be considered in cases of trauma or complex deformities to delineate vertebral artery anatomy, especially prior to C1/C2 or subaxial pedicle screw placement.
- Electrophysiological Studies: Somatosensory Evoked Potentials (SSEPs), Motor Evoked Potentials (MEPs), and electromyography (EMG) may be used pre-operatively to establish a baseline and confirm neurological deficits.
- Medical Optimization: Address comorbidities, optimize nutrition, and discontinue antiplatelet/anticoagulant medications as appropriate.
Anesthetic Considerations
- Airway Management: Secure intubation is critical. Oral endotracheal intubation is standard. Fiberoptic intubation may be required for unstable cervical spine injuries or difficult airways.
- Neuromonitoring: Intraoperative neurophysiological monitoring (IONM) with SSEPs and MEPs is highly recommended, if not mandatory, during cervical spine surgery to detect impending neurological compromise. EMG may also be used to monitor nerve root integrity.
- Arterial Line: For continuous blood pressure monitoring.
- Central Venous Access: May be considered for large-volume procedures or in patients with significant comorbidities, particularly if a seated position is contemplated (risk of air embolism).
Patient Positioning
The patient is typically positioned
prone
for the posterior cervical approach.
The goal is to provide adequate exposure, maintain cervical lordosis or neutral alignment, prevent excessive neck flexion, and minimize pressure points.
-
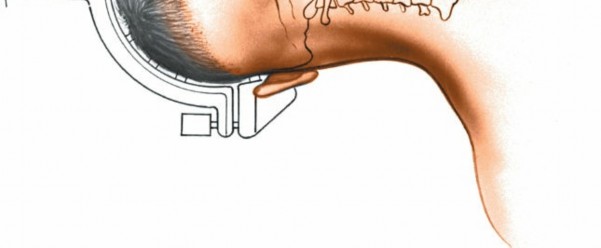
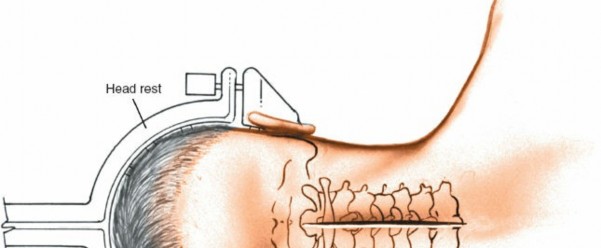
Prone Position Setup:
- Head Fixation: The head is typically secured in a skull traction device such as a Mayfield clamp or a Gardner-Wells tongs, attached to the operating table. This allows rigid fixation and precise control over cervical alignment. It is imperative to ensure the patient's eyes are protected, and the ears are clear of pressure. Avoid excessive traction that might distract the cervical spine, particularly in cases of pre-existing instability.
- Torso Support: Chest rolls or a well-padded operating room frame (e.g., Jackson table, OSI table) are used to elevate the chest, allowing the abdomen to hang freely. This minimizes intra-abdominal pressure, which reduces epidural venous bleeding by decreasing pressure in the inferior vena cava.
- Arm Positioning: Arms are abducted less than 90 degrees and padded to prevent brachial plexus injury. The elbows should be slightly flexed.
- Legs: Padded to prevent pressure neuropathies. The knees are slightly flexed with a pillow underneath.
- Alignment: Ensure the cervical spine is in neutral or slight lordosis, avoiding any undue flexion, which can stretch the spinal cord. Intraoperative lateral fluoroscopy or radiography is used to confirm proper alignment before incision.

-
Alternative Seated Position:
- The patient may be seated upright with the head held in a special brace. This position can offer advantages in terms of decreasing venous bleeding due to gravity, and it might provide a more ergonomic working position for some surgeons.
- Risks: However, the seated position carries a significant risk of venous air embolism, particularly with opening of large venous sinuses, and requires vigilant monitoring (e.g., precordial Doppler, end-tidal CO2). Hypotension can also be more pronounced. Due to these risks, the prone position is generally preferred for most subaxial cervical spine procedures.
Intraoperative Illumination and Imaging
- Illumination: High-quality illumination is crucial. A cold-light headlamp is essential, and the use of an operating microscope or surgical loupes with coaxial illumination adds significant clarity to the operative field, particularly for microdissection, nerve root identification, and fine instrumentation.
- Intraoperative Imaging: Fluoroscopy (AP and lateral views) or an intraoperative CT navigation system is indispensable for confirming vertebral levels, assessing reduction, and guiding accurate placement of spinal instrumentation (e.g., lateral mass or pedicle screws).
Detailed Surgical Approach / Technique
The posterior approach to the subaxial cervical spine involves a series of methodical steps designed to achieve adequate exposure, perform the necessary decompression or stabilization, and minimize tissue damage.
1. Incision and Initial Dissection
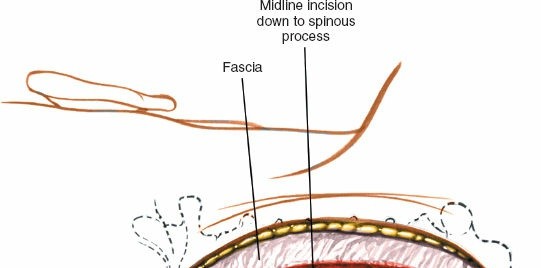
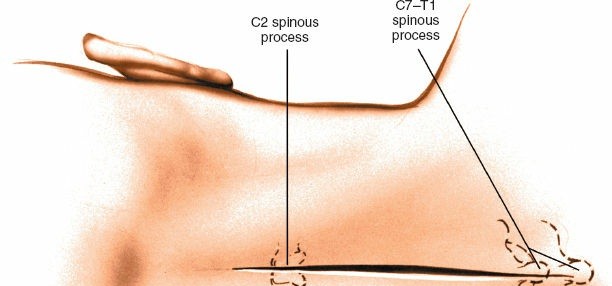
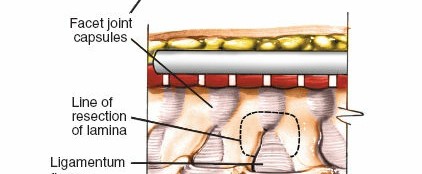
- Skin Incision: A midline posterior incision is made, extending vertically to encompass the necessary number of vertebral levels. Palpation of the C7 spinous process (vertebra prominens) and the external occipital protuberance helps guide the incision length. The incision is carried through the skin and subcutaneous tissue down to the ligamentum nuchae.

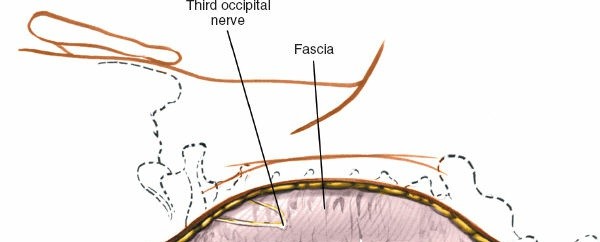
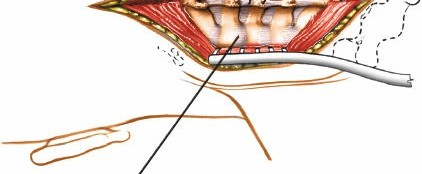
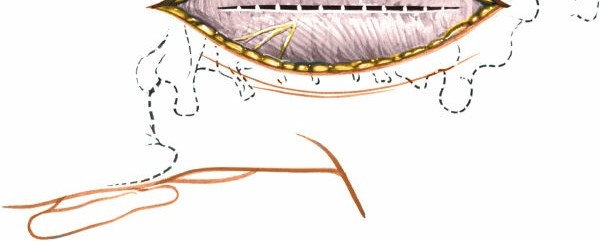
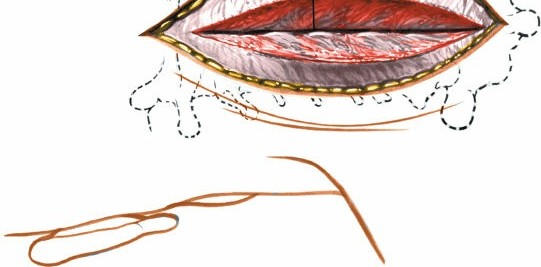
- Subperiosteal Dissection: The midline raphe of the ligamentum nuchae is sharply incised. Subperiosteal dissection is then performed using electrocautery and Cobb elevators to detach the paravertebral muscles (trapezius, splenius, semispinalis cervicis/capitis, multifidus) from the spinous processes and laminae. The dissection proceeds laterally, staying tight on the bone, down to the facet capsules and lateral masses.

- Exposure: Self-retaining retractors (e.g., Weitlaner, cerebellar) are carefully placed and incrementally opened to maintain exposure. Care must be taken to avoid excessive traction on the muscles, which can lead to ischemic injury. The dissection should expose the posterior elements of the target vertebrae: spinous processes, laminae, and lateral masses.
2. Vertebral Level Identification
- Palpation: C2 is identified by its large, bifid spinous process. C7 is often the most prominent spinous process. Counting from these landmarks helps confirm levels.
- Fluoroscopy: Intraoperative lateral fluoroscopy is essential to definitively confirm the vertebral levels and the extent of required exposure. A radiopaque marker can be placed on a specific spinous process to correlate with the fluoroscopic image.
3. Decompression Techniques
a. Laminectomy
- Indications: Multilevel cervical myelopathy, intradural tumors, severe posterior compression.
-
Technique:
Laminectomy involves the complete removal of the lamina and spinous process at the affected levels.
- A high-speed burr or Kerrison rongeurs are used to create troughs at the lateral edges of the laminae, medial to the facet joints.
- The ligamentum flavum is carefully resected.
- The spinous process and laminae are then removed piecemeal or en bloc.
- Extreme caution is exercised to protect the dura and spinal cord. Epidural veins can be copious and must be meticulously coagulated.
- After removal of the laminae, the dura is inspected for any tears and the spinal cord for adequate decompression.
- Considerations: Extensive laminectomy, particularly in children or patients with pre-existing kyphosis, may lead to post-laminectomy kyphosis. Fusion is often combined with laminectomy to prevent this complication.
b. Laminoplasty
- Indications: Multilevel cervical myelopathy, OPLL, where maintenance of posterior column integrity is desired.
-
Technique:
Laminoplasty aims to expand the spinal canal by creating a "door" of laminae that is then held open.
- Open-door laminoplasty: A hinge is created on one side (e.g., by thinning the lamina with a burr), and a trough is created on the contralateral side, allowing the laminae to be lifted and opened like a door. The opened laminae are then secured in the open position with small plates and screws or sutures.
- Double-door laminoplasty: Troughs are created on both sides, and the spinous processes are split to create two "doors" that open laterally. This is less commonly used in the subaxial spine due to challenges in fixation.
- Advantages: Preserves muscle attachments and posterior column elements, potentially reducing the risk of post-operative kyphosis and C5 nerve root palsy compared to laminectomy with fusion.
- Disadvantages: May not be suitable for all cases, such as those with significant instability or kyphosis.

4. Posterior Cervical Fusion
Fusion aims to achieve arthrodesis and provide stability, often coupled with decompression.
a. Facet Joint Reduction (for Dislocations)
- For perched or locked facets, gentle axial traction is applied (often pre-operatively) to unlock the facets. Intraoperative direct manipulation using various instruments (e.g., towel clamps on spinous processes, spreader devices in facet joints) can aid reduction. Care must be taken to avoid cord over-distraction.
- Once reduced, the facets are typically stabilized with instrumentation.
b. Instrumentation
Modern posterior cervical fusion predominantly utilizes screw-rod constructs.
*
Lateral Mass Screws:
The most common method for subaxial cervical instrumentation (C3-C6).
*
Entry Point:
Typically 2-3 mm medial to the midpoint of the lateral mass and 2-3 mm superior to the inferior articular facet.
*
Trajectory:
*
Roy-Camille Technique:
10 degrees cephalad and 30 degrees lateral.
*
Magerl Technique:
0-10 degrees cephalad and 20-30 degrees lateral.
*
Anteroposterior (AP) Technique:
Approximately 10-15 degrees cephalad and 0-5 degrees lateral (more straight forward).
*
Drilling:
A 2.0 mm pilot hole is drilled to a depth of 12-16 mm. Fluoroscopy helps confirm trajectory and depth.
*
Tapping:
The pilot hole is typically tapped.
*
Screw Insertion:
3.5 mm cortical screws are inserted.
*
Pedicle Screws:
Offer superior biomechanical rigidity but carry a higher risk profile due to proximity to the vertebral artery and spinal cord. Typically reserved for C2 and C7, or in cases of revision surgery, deformity, or when lateral mass screws are contraindicated (e.g., fractured lateral mass).
*
C2 Pedicle Screws:
Entry point and trajectory are highly specific and often require intraoperative navigation or meticulous fluoroscopic guidance.
*
C7 Pedicle Screws:
Entry point is usually at the junction of the lamina and the transverse process, targeting the pedicle.
*
Rods:
Pre-contoured or intraoperatively contoured rods are connected to the screw heads and locked into place. Compression or distraction can be applied as needed to achieve desired alignment.




c. Bone Grafting
- Decortication: After instrumentation, the posterior bony elements (laminae, articular masses) are decorticated using a high-speed burr to expose cancellous bone, promoting fusion.
-
Graft Material:
- Autograft: Local autogenous bone (e.g., from spinous processes or iliac crest) remains the gold standard for fusion due to its osteoconductive, osteoinductive, and osteogenic properties.
- Allograft: Demineralized bone matrix (DBM) or cancellous allograft can be used, often with biologics.
- Biologics: Bone morphogenetic proteins (BMPs) can be used to enhance fusion, though their use in the cervical spine remains a subject of ongoing debate due to potential complications (e.g., swelling, heterotopic ossification).
- The bone graft is packed onto the decorticated posterior elements and around the instrumentation.
5. Hemostasis and Closure
- Hemostasis: Meticulous hemostasis is crucial throughout the procedure, particularly from the epidural venous plexus. Bipolar cautery, bone wax, Gelfoam, and other hemostatic agents are employed.
- Drainage: A subfascial drain (e.g., Jackson-Pratt) is typically placed to evacuate post-operative hematoma, especially in more extensive procedures.
- Layered Closure: The muscle fascia (ligamentum nuchae), subcutaneous tissue, and skin are closed in layers.


Complications & Management
Complications following posterior cervical spine surgery, while relatively uncommon, can be significant. Vigilant intraoperative technique and comprehensive post-operative care are essential.
Common Complications and Salvage Strategies
| Complication | Incidence | Description & Risk Factors | Management & Salvage Strategies |
|---|---|---|---|
| Neurological Injury | |||
| Spinal Cord Injury | < 0.5% (fusion), 0.5-2% (laminectomy/plasty) | Direct trauma during decompression, excessive traction/distraction, malposition of hardware, cord contusion during reduction of dislocations, intraoperative ischemia. | Immediate recognition via IONM. Correct inciting factor (remove hardware, revise reduction, decompress). Administer high-dose corticosteroids (if acute SCI protocol), optimize hemodynamics. Post-op MRI for cord edema/hematoma. |
| Nerve Root Injury | 1-5% (C5 palsy most common) | Direct trauma during decompression (e.g., lateral mass screw placement too medial/deep, foraminotomy), C5 nerve root traction/tethering (especially after laminoplasty due to posterior shift of cord). | Monitor IONM. If C5 palsy, observe initially; most resolve spontaneously within 6-12 months. Rarely, surgical exploration and decompression/neurolysis if persistent or severe. Optimize neck posture. |
| Dural Tear / CSF Leak | 1-10% | During laminectomy, laminoplasty, or extensive decompression; often due to thin dura or adhesion to bone/osteophytes. | Intraoperative repair with primary suture (e.g., 6-0 Prolene) reinforced with dural sealant (fibrin glue, dura substitute), fat graft, or muscle patch. Post-op strict bed rest, head elevation, avoiding Valsalva. Lumbar drainage if persistent or large leak. |
| Vascular Injury | Rare (< 0.1%) | ||
| Vertebral Artery Injury | Extremely rare (< 0.01%) | During lateral mass or pedicle screw placement, particularly at C2 or C7, or during aggressive lateral dissection. Can lead to stroke, hemorrhage. | Immediate tamponade, direct repair if possible (vascular surgeon consult), packing, or ligation. Angiography to assess patency and collateral flow. Urgent neurology consultation. |
| Epidural Vein Bleeding | Common, often controlled | Extensive epidural venous plexus. Increased intra-abdominal pressure (e.g., improper prone positioning). | Meticulous hemostasis with bipolar cautery, Gelfoam, Surgicel, bone wax. Optimize positioning to allow free abdomen. Maintain normotension. |
| Infection | 1-5% | ||
| Superficial Wound Infection | 1-3% | Staphylococcus aureus most common. Poor wound care, prolonged surgery, immunocompromised patient. | Oral or IV antibiotics. Local wound care. If abscess, incision and drainage. |
| Deep Surgical Site Infection | < 1% | Involvement of bone or hardware. Same risk factors as superficial. | IV antibiotics (long course). Surgical debridement, wash-out. Removal of hardware if infection is recalcitrant or causes instability/failure of fusion. If hardware must remain, prolonged suppressive antibiotics. |
| Hardware-Related Complications | |||
| Hardware Malposition | Varies with technique (0.5-5%) | Incorrect screw trajectory/depth, especially lateral mass screws (too lateral into nerve root, too medial into spinal cord, too anterior into vertebral artery). | Intraoperative revision with fluoroscopy/navigation. If neurological deficit, immediate removal and repositioning. Post-op: observe, revise if symptomatic or risk to neural/vascular structures. |
| Hardware Failure | 2-10% | Screw pullout, rod fracture, breakage. Often due to pseudarthrosis, poor bone quality, or excessive load. | Revision surgery with stronger construct, longer construct, additional bone graft, or supplemental anterior support if pseudarthrosis. |
| Fusion-Related Complications | |||
| Pseudarthrosis (Non-Union) | 5-20% (higher with poor bone quality, smoking) | Failure of bony fusion. Leads to persistent pain, instability, or hardware failure. | Revision surgery with decortication, additional bone graft, biologics, and potentially stronger or longer instrumentation. Smoking cessation is critical. |
| Adjacent Segment Disease (ASD) | 2-4% per year | Degeneration at levels adjacent to a fused segment, due to altered biomechanics and increased stress. | Initial conservative management. If progressive neurological deficit or severe pain, surgical decompression and fusion of the adjacent segment. |
| Other Complications | |||
| Post-Laminectomy Kyphosis | 5-20% (higher in children, multi-level laminectomy) | Loss of cervical lordosis leading to sagittal imbalance, pain, and sometimes myelopathy. More common with extensive laminectomy without fusion, especially in younger patients or those with poor muscle integrity. | Prevention is key (laminoplasty or laminectomy with fusion). If symptomatic, revision surgery with posterior fusion to restore lordosis, or combined anterior-posterior approach. |
| Hematoma | 1-2% | Post-operative bleeding leading to compression of neural structures (epidural hematoma) or airway compromise. | Prophylactic drain placement. Close post-op neurological monitoring. If compressive symptoms develop (e.g., neurological deterioration, stridor), emergent surgical evacuation of hematoma. |
| Air Embolism | Rare (seated position risk) | Entrainment of air into open venous sinuses, leading to cardiovascular collapse or neurological sequelae. | Prevention: avoid seated position if possible. If detected, immediate flooding of surgical field, Trendelenburg position, CVP line aspiration of air, supportive care. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing patient recovery, achieving successful fusion, and restoring function after posterior cervical spine surgery. Protocols are tailored based on the extent of surgery, stability of the construct, and individual patient factors.
Immediate Post-Operative Period (Days 0-7)
- Pain Management: Multimodal analgesia including NSAIDs (if no contraindications), acetaminophen, and opioids as needed. Regional blocks can be considered.
- Wound Care: Daily inspection for signs of infection (erythema, discharge, fever) or hematoma. Drain removal typically within 24-48 hours when output is minimal.
- Neurological Monitoring: Frequent neurological checks (motor, sensory, reflexes) to detect any new deficits or changes.
-
Mobilization:
- Early Ambulation: Typically encouraged within 24 hours post-operatively to prevent complications such as DVT and pulmonary emboli, and to promote overall recovery.
-
Cervical Orthosis (Bracing):
The use of a cervical collar (soft vs. rigid) varies widely among surgeons and depends on the specific procedure and intraoperative stability.
- No Collar: Often for laminoplasty or single-level fusion with robust fixation and no instability.
- Soft Collar: For comfort, proprioception, and mild support.
- Rigid Collar (e.g., Miami J, Philadelphia collar): Typically used for multi-level fusions, complex reconstructions, trauma cases, or patients at high risk for non-union. Duration varies from 6-12 weeks.
- Activity Restrictions: No heavy lifting (>10 lbs), pushing, pulling, or excessive twisting/bending of the neck. Avoid prolonged sitting.
Early Rehabilitation Phase (Weeks 2-6)
- Physical Therapy (PT) Assessment: Initial PT evaluation to assess range of motion (ROM), pain, muscle strength, and functional limitations.
- Gentle Range of Motion (ROM): If a rigid collar is removed or not used, gentle, protected active and passive ROM exercises (flexion, extension, lateral bending, rotation) within pain limits. Emphasis on maintaining proper posture.
- Isometrics: Gentle isometric neck strengthening exercises as tolerated.
- Scapular Stabilization: Exercises to strengthen periscapular muscles to support cervical posture.
- Aerobic Conditioning: Low-impact activities such as walking to improve endurance and overall well-being.
- Education: Reinforce activity restrictions, proper body mechanics, and pain self-management strategies.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Progression of Strength and ROM: Gradually increase the intensity of neck and upper extremity strengthening exercises. Incorporate resistance bands or light weights.
- Proprioceptive Training: Exercises to improve neck position sense and balance.
- Cardiovascular Endurance: Further increase aerobic activity.
- Gradual Return to Activities of Daily Living (ADLs): Progressively return to light recreational activities.
Advanced Rehabilitation Phase (Months 3-6+)
- Functional Progression: Focus on restoring full functional capacity and preparing for return to work or sport-specific activities.
- Dynamic Strengthening: Incorporate dynamic neck strengthening and core stability exercises.
- Impact Activities: Gradual introduction of impact activities, if appropriate, based on radiographic evidence of fusion and surgeon's discretion.
- Long-Term Follow-up: Regular clinical and radiographic follow-up to assess fusion status, alignment, and adjacent segment health.
Important Considerations:
*
Smoking Cessation:
Absolutely critical for fusion success. Patients should be counseled pre- and post-operatively.
*
Radiographic Assessment of Fusion:
Often performed at 3, 6, and 12 months post-operatively. Dynamic radiographs (flexion/extension) may be used to assess stability if pseudarthrosis is suspected. CT scans provide the most reliable assessment of bony bridging.
*
Individualization:
Rehabilitation protocols must be individualized based on patient progress, surgical findings, and the development of any complications.
Summary of Key Literature / Guidelines
The posterior approach to the subaxial cervical spine is supported by a robust body of literature and has been refined through decades of clinical research. Key areas of investigation and established guidelines include:
1. Laminectomy vs. Laminoplasty for Multilevel Myelopathy
-
Laminoplasty:
Considered by many to be the preferred posterior decompression strategy for multilevel cervical myelopathy without significant kyphosis or instability. Studies have shown comparable neurological outcomes to laminectomy with fusion, with potentially lower rates of pseudarthrosis and less blood loss. It aims to preserve posterior column integrity and muscle attachments, theoretically reducing the risk of post-laminectomy kyphosis.
- Key Literature: Multiple meta-analyses and prospective studies have demonstrated the efficacy of laminoplasty. A systematic review by Hirabayashi et al. (1989) popularized the "open-door" technique, and subsequent studies have validated its long-term benefits in improving neurological function while maintaining cervical lordosis.
- Laminectomy with Fusion: Indicated when instability or significant kyphosis is present, or when laminoplasty is not feasible. While effective for decompression, it historically carried a higher risk of post-operative kyphosis, particularly in older techniques without rigid internal fixation. Modern techniques incorporating robust instrumentation have significantly improved outcomes.
2. Posterior Cervical Instrumentation
- Lateral Mass Screws: The work of Roy-Camille et al. (1991) and Magerl and Grob (1986) established the anatomical basis and technical nuances for lateral mass screw placement. Numerous biomechanical and clinical studies have validated the safety and efficacy of these techniques, making them the standard for subaxial posterior cervical fusion. Current guidelines from organizations like NASS (North American Spine Society) and AOSpine generally support the use of lateral mass screws for most subaxial fusions.
-
Pedicle Screws:
While biomechanically superior, pedicle screw placement in the subaxial cervical spine is technically demanding due to the proximity of the vertebral arteries and spinal cord. Their use is typically reserved for specific indications such as C2 and C7 fixation, cases of lateral mass fracture, revision surgery, or severe deformity. Intraoperative navigation and advanced imaging (e.g., CT guidance) are strongly recommended to enhance safety.
- Key Literature: Studies by Ludwig et al. (1999) and others have detailed the morphometry and techniques for subaxial pedicle screw placement, highlighting the increased risk but potential benefits in specific situations.
3. Management of Cervical Trauma
-
Reduction of Facet Dislocations:
Early reduction (within 72 hours, preferably within 8-12 hours) is critical to optimize neurological recovery in patients with cervical facet dislocations. Closed reduction with gradual traction is often attempted first, followed by surgical reduction and stabilization (typically posterior fusion with instrumentation) if closed reduction fails or for persistent instability.
- Key Literature: Guidelines from the Spine Trauma Study Group and other major trauma centers emphasize early, often emergent, surgical stabilization for unstable cervical spine injuries, with posterior approaches playing a central role in managing posterior ligamentous complex disruption.
4. C5 Nerve Root Palsy
-
C5 nerve root palsy, characterized by deltoid and biceps weakness, is a recognized complication of cervical decompression, particularly after laminoplasty (incidence 5-20%). The etiology is thought to be multifactorial, including direct nerve root manipulation, spinal cord shift and tethering, and ischemia.
- Key Literature: Research by Machino et al. (2014) and others has extensively studied C5 palsy, showing that most cases are transient and resolve spontaneously. Prevention strategies include adequate foraminotomy, avoiding excessive cord shift, and maintaining proper cervical alignment.
5. Sagittal Balance
-
The importance of restoring and maintaining physiological cervical sagittal alignment (lordosis) is increasingly recognized. Loss of cervical lordosis (kyphosis) after posterior surgery can lead to persistent pain, functional limitations, and adjacent segment disease.
- Key Literature: Studies by Glassman et al. (2005) and others in the thoracolumbar spine, and more recently applied to the cervical spine, underscore the biomechanical implications of sagittal alignment on clinical outcomes. Modern posterior fusion techniques aim to achieve or restore appropriate cervical lordosis during instrumentation.
The evolution of surgical techniques, advanced imaging, and intraoperative neuromonitoring has significantly enhanced the safety and efficacy of the posterior approach to the subaxial cervical spine. Continuous education and adherence to evidence-based guidelines remain paramount for optimal patient care.
Clinical & Radiographic Imaging